











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por email
 Permalink
Permalink
INTRODUCTION
Medicine has domains that require complex learning. 1 The complexity of learning involves the understanding of intricate physiological systems, which can subsidize the development of adaptive expertise and the acquisition of technical skills necessary for good clinical practice, such as performing a physical examination, interpreting imaging examinations, and performing clinical and / or surgical reasoning. 1 , 2 Anatomy is at the core of some of these domains of knowledge and processes of clinical-surgical rationality, and this should not be discussed. 3 Over the past 400 years, anatomy has been one of the world’s leading health learning tools, traditionally taught through conventional lectures, textbooks, picture atlases, and cadaveric dissections. 4 , 5
Despite this scope, even nowadays, there are important educational problems related to the teaching of anatomy: 4 , 5 1) Restriction of the acquisition of corpses by educational institutions, mainly because of budgetary, ethical, cultural, and social reasons, or even due to their unavailability; 4 , 5 2) Significant shortage of qualified professionals for the dissection method; 3) Risk of acquiring serious diseases due to the use of chemicals (e.g., formaldehyde); 4) Great logistical and financial burden regarding the storage conditions of corpses; 6 and 5) The profound curriculum reformulation that many medical schools around the world have experienced, essentially characterized by the introduction of active learning methodologies. 2
All these reasons led to the need to rethink the teaching of anatomy. 2 Additionally, they have allowed the adoption of a wide range of learning resources, especially technological ones. 2 These measures have resulted in the proposal of a series of complementary innovative approaches to the teaching of anatomy, including: computational software; problem situations that simulate real clinical cases; simulator models; plastic models; and three-dimensional (3D) models. 7
3D anatomical models have a close relationship with the essentially visual field 1 , 8 and this visual-spatial nature of learning is justified by the presence of two factors: stereopsis (perception of depth when something is viewed with both eyes) and dynamic exploration. 2 , 9 , 10 When properly applied, these principles can improve understanding of the spatial relationship, characteristic of anatomical structures, especially the most complex ones. 5 Therefore, 3D resources can favor the understanding of anatomical structures from their global perspective, as well as contribute to a better assimilation of knowledge already acquired in classes and from atlases. 1 Nicholson et al. found that medical students who studied the inner ear using a tutorial accompanied by a 3D anatomical model scored 18 points higher than students who studied by the tutorial alone. 9
Several 3D systems have been developed for the teaching of anatomy. One of the most advanced anatomy visualization systems is the 3D anatomical table. It is a digital visualization platform that has real-size male and female virtual corpses. This characteristic has provided the inclusion of a powerful image editing tool, with features derived from a software approved by the U.S. Food and Drug Administration (FDA) for surgical planning. 11 This tool merges customizable 3D models derived from real patient images, which enables full-size simulations. 11
From an academic point of view, the anatomical table can be useful as a complementary resource for cadaveric studies. Once the axial sections are properly recorded and segmented in traditional dissection, they are used on the table to create final images of any anatomical system or structure on all three axes of the body. 12 The possibility of functioning as an imaging workstation is a particularly relevant characteristic of this resource, especially when one wants to study anatomy applied to a pathological example or simply to analyze exams. 11 For instance, computed tomography (CT) and magnetic resonance imaging (MRI) of the liver can be viewed interactively in 3D. 11
Complex structures, such as the liver and gallbladder, can be well displayed by the table. 3D visualization of the liver facilitates the visibility of its contents and allows the use of visual perception methods such as immersion, navigation, and interaction. 3 The liver is one of the major organs vulnerable to tumors, and greater knowledge about its 3D image can improve the physician’s expertise in clinical situations. For instance, liver damage close to crucial structures could be more easily assessed through 3D imaging, especially by students. 3 , 12 Moreover, in eventual surgical cases, 3D liver imaging evaluations could lead to more accurate resections, without concomitant removal of healthy liver tissue and impairment of adjacent structures. 12
Although CT and MRI sections provide data on the lesion, sometimes their precise location in relation to large blood vessels is not evidently satisfactory (e.g., the hepatic portal vein or biliary tract). 13 Not only that, these images can be difficult to understand and interpret for an inexperienced team and, especially for medical students. 3 The combination of these factors led us to believe that the traditional method of teaching hepatobiliary anatomy in medical schools might not be sufficient to guarantee the necessary skills for good clinical practice. Thus, it is necessary to evaluate whether the 3D anatomical table is an effective resource to support the teaching of applied hepatobiliary anatomy to undergraduate medical students.
METHODS
This study was approved by the PUC-Rio Internal Ethics Committee (n. 2015-55) and also by the UNIFESO Research Ethics Committee (REC) (CAAE: 54519415.0.0000.5247). The Free and Informed Consent Form (ICF) was obtained from all participants prior to study enrollment. There were no conflicts of interest related to this research.
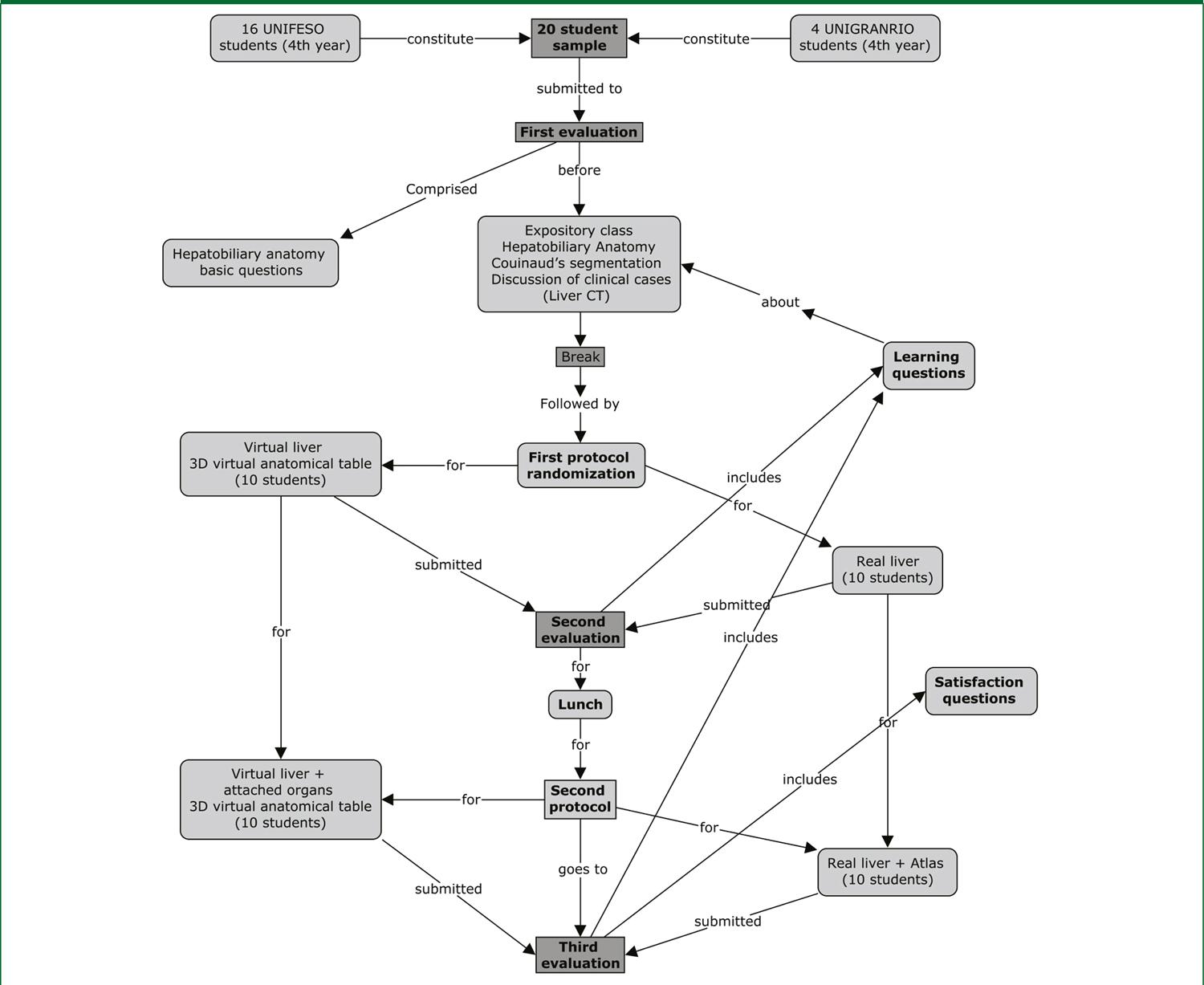
For this study, volunteer undergraduate students from the 4 th year of medical school were recruited exclusively. Students from other periods of medical school, as well as students from other undergraduate courses at participating institutions, were not included. Among the participants, those who failed to perform any research steps were excluded. The research protocol was fully applied at the Pontifícia Universidade Católica do Rio de Janeiro (PUC-Rio), in the city of Rio de Janeiro (RJ), which owns the 3D anatomical table. The medical students came from Serra dos Órgãos University Center (UNIFESO), located in the municipality of Teresópolis (RJ); and from Universidade do Grande Rio (UNIGRANRIO), located in the municipality of Caxias (RJ). After recruitment, the participants were randomized and allocated into two groups.
The participants were assessed regarding two outcomes: 1) Learning – which refers, in this study, to the assimilation of information given during the classes, i.e., technical questions about the anatomy and clinical cases about the hepatobiliary structure. It also refers to the dimensions of representation about learning (referential and procedural), which was evaluated quantitatively; and 2) Self-perception – the students’ own perception of the satisfaction of their learning in relation to the resources used. Learning was assessed through 3 multiple-choice questionnaires (alternatives A to D), totaling 30 questions. The first questionnaire (“pre-test”) included 10 questions on hepatobiliary anatomy and physiology. This assessment was applied before the students received any technical information and was justified by the need to verify their previous knowledge about the subject, in order to evaluate whether possible differences in this phase could affect the final results of the research. Shortly thereafter, all participants received expository content during a 90-minute (one-and-a-half hour) class, which focused on hepatobiliary anatomy and Couinaud’s segmentation, as well as the presentation of actual clinical cases on hepatobiliary structures (consisting of expository class and use of imaging exams). The liver was chosen as the study organ because it has some characteristics that favor a more reliable evaluation of the three-dimensional visualization. Firstly, it is an organ of which anatomical nomenclature is addressed early in the medical undergraduate course. Therefore, during the clinical cycle of the course, students, already familiar with the anatomical structure, are introduced to Couinaud’s hepatic segmental anatomy. This model was proposed by Couinaud in the 1960s and is widely accepted in clinical practice and especially in liver surgery. 3 Moreover, anatomically, the liver is a globular organ. This facilitates comparison with 3D models for tumor-specific location and better planning of liver resection margins (typical requirements for liver surgery are locating the tumor and determining its associations with intrahepatic vascular and biliary systems). 3
The image data were entirely generated by the 3D virtual anatomical table, which belongs to the medical department of PUC-Rio. The internal visualization of the virtual liver was performed through a transparency control and sections in all of its axes (sagittal, coronal and transversal). Two real, formalin-preserved livers were transferred from UNIFESO to PUC-Rio two days prior to the application of the study protocol with specific authorization for this purpose. The livers (one with and the other without attached structures) were stored in thermal boxes, remaining under storage until the research instruction phase.
Randomization
After the expository class, the students were randomized and allocated to: 1) Experimental group – hepatobiliary anatomy + Couinaud’s segmentation (explored exclusively on the 3D anatomical table (Anatomage / software 3.0)); versus 2) Control group – same content as the experimental group; however, seen in a real liver. This phase was coordinated by the same teachers who taught the classes in the first phase (they received previous instructions about the use of the 3D anatomical table). To avoid introducing a bias regarding the teacher’s teaching method, both teachers were in charge of teaching both groups. To allow this, the interventions were applied at different times.
At the end of this phase, both groups were submitted to the second evaluation, consisting of 10 technical questions about the content. The aim of this evaluation was to verify the comparative effectiveness of the 3D virtual anatomical table with the real formalin-preserved model – and questions about the students’ own perception of satisfaction with the resources used to teach anatomy.
Finally, after the second assessment, the students were submitted to the last step related to instruction. Maintaining the same allocation, the students from each group returned, respectively, to the 3D anatomical table and the real liver. In this phase, participants were instructed about the liver and the attached structures and organs. For that purpose, resources from the virtual table that insert and / or remove attached organs were used. As for the real liver, two fresh organs were used in the study: a simple one (only liver and the gallbladder) and one with attached structures. At this phase, once again, the instructions were provided at different times by the same teachers to avoid the introduction of a bias related to the teaching method. After this phase, the third and last evaluation of the study, with a total duration of 30 minutes, was applied. In this test, in addition the 10 technical questions, 12 questions regarding the perception of self-satisfaction about the teaching resources were also applied. A flowchart representing the entire research protocol is shown in figure 1 .
Analyses
Student performance (learning) was assessed regarding the overall assessment score, being measured by two outcomes: incorrect response rate; and failure rate. The student who gave at least 11 incorrect questions was considered as having failed. The answers were only considered as correct or incorrect. All results (correct / incorrect) and the time required to answer each assessment were automatically recorded. The number of correct answers in each evaluation was tested in relation to their normality, from the values of asymmetry and kurtosis, being considered normal. Therefore, the number of correct answers in each evaluation (evaluations 1 to 3) and in each group (G1 – Anatomical Table and G2 – Real anatomical piece) was synthesized as mean followed by the respective standard deviation. The absolute difference between two means was presented. The comparison between the mean number of correct answers between two evaluations was tested by paired Student’s t test. On the other hand, the comparison between the mean number of correct answers between the two interventions was performed by Student’s t test for independent samples. The significance level was set at 5% (p <0.05).
To investigate the effect of the interventions on the students’ perceptions of their learning, a Likert scale was used, a 12-topic questionnaire using an inductive approach, where responses were grouped into 5 subcategories that can be quantified (I fully agree; I agree more than disagree; I cannot give an opinion; I disagree more than agree; I fully disagree). The first six questions are affirmative; the last six constitute a repetition of the first six; however, in the negative form. The purpose of this model is to verify the logical agreement between two contrary answers concerning the same question.
RESULTS
A total of 20 undergraduate students (65% women) participated in this study. Sixteen students came from UNIFESO and four from UNIGRANRIO. All participants remained in the research protocol until the end of the study. Gender distribution was similar between the two groups (Chart 1). There was no statistically significant difference regarding the students’ previous knowledge of hepatobiliary anatomy (p = 0.290), and there was no difference between the groups regarding the other evaluations (2 nd assessment: p = 0.572; and 3 rd assessment: p = 0.414).
CHART 1 Distribution of participants by gender and randomization
| N (%) | Female gender | |
|---|---|---|
| G1 Anatomical table | 10 (50%) | 6 (60%) |
| G2 Real liver | 10 (50%) | 7 (70%) |
| Total | 20 (100%) | 13 (65%) |
Overall, the resources that were evaluated improved the participants’ learning. In the longitudinal comparison between the pretest and the two subsequent evaluations, the increase in knowledge about hepatobiliary anatomy and Couinaud’s segmentation was significant in both, being higher in the 2 nd evaluation – applied after the expository class and randomization to the anatomical table or real liver (p = 0.001), when compared to the 3 rd assessment – after the inclusion of attached organs in the anatomical table or real liver (p = 0.012) ( Chart 2 ). In the longitudinal comparison of the performance between the groups, the group that used the real liver was significantly better than the group that used the anatomical table in the 2 nd evaluation (p = 0.002). On the other hand, when the longitudinal comparison was between the pre-test and the 3 rd evaluation, the group that used the anatomical table performed significantly better (p = 0.040).
CHART 2 Analysis of the learning results
| Group | 1 st evaluation Mean ± SD | 2 nd evaluation Mean ± SD | Difference between the 1 st and 2 nd evaluations | 3 rd evaluation Mean ± SD | Difference between the 1 st and 3 rd evaluations | ||
|---|---|---|---|---|---|---|---|
| (A) | (B) | (B-A) | p -value | (C) | (C-A) | p- value | |
| Comparison between 2 evaluations | |||||||
| All | 6.50 (1.64) | 7.95 (1.15) | +1.45 | 0.001 | 7.70 (1.59) | +1.20 | 0.012 |
| Anatomical table (G1) | 6.90 (1.20) | 7.80 (1.14) | +0.90 | 0.121 | 8.00 (1.49) | +1.10 | 0.040 |
| Real liver (G2) | 6.10 (1.97) | 8.10 (1.20) | 2.00 | 0.002 | 7.40 (1.71) | +1.30 | 0.122 |
| Comparison between the two interventions (G1 x G2) | |||||||
| Difference | 0.80 | 0.30 | – | – | 0.60 | – | – |
| p -value | 0.290 | 0.572 | – | – | 0.414 | – | – |
As explained, the second evaluation prioritized questions that addressed the three-dimensional visualization of the organ. On the other hand, the component statements of the third evaluation prioritized the liver’s connections with other body structures. Unlike the real liver, the 3D liver allowed visualization of the internal structures of the organ, such as hepatic veins and arteries. This technique occurred in two ways: through transparency control or through the use of the virtual scalpel, which “cut” the organ in several axes.
The results of the self-satisfaction assessment are shown in table 3, expressed as percentage of discordants. This criterion was adopted because it was based on the premise that most participants consider at least adequate the resources used for learning (especially the real liver, which is a reference standard for teaching anatomy). Secondly, a better visualization of the effect of resources was expected when comparing the groups. Overall, the students’ perception of satisfaction with the resources that were used in the study for the learning of hepatobiliary anatomy was considered very good, with a minimum overall satisfaction rate of 80%. When the survey specifically referred to the easily assimilated knowledge when using these learning resources, the percentage of agreement was total (100%). In the comparative mode between the groups, 20% of the students allocated to the real liver group were not satisfied with this type of resource, compared to 0% of this result in the table group. On the other hand, 30% of participants allocated to the anatomical table did not feel stimulated to learn hepatobiliary anatomy using the 3D feature, compared to 10% of the real liver group.
The self-satisfaction survey had as its target the learning resources that were used. Nevertheless, the instructors were also included in the assessment, because they consider that the way they explore pedagogical resources may interfere with students’ perceptions of satisfaction. Based on this assumption, it was observed that 10% of the participants allocated to the anatomical table considered that the teachers did not take full advantage of the teaching capacity of this resource. The discordance on this topic in the real liver group was total. When the question addressed the students’ capacity to reproduce the knowledge they obtained from their classes, 10% of each group stated that they did not feel able to perform this task. This proportion was the same as when the participants were asked about their motivation to utilize once again the resource that was used in the activity.
DISCUSSION
This study demonstrated that a high-resolution 3D digital platform with a full-size, virtual liver and gallbladder is an appropriate resource for teaching anatomy in Medicine. This statement – supported by other studies in the literature 14 , 15 – is supported by the fact that the virtual anatomical table was able to provide the information to the medical student as well as a formalin-preserved real liver. This finding is demonstrated because both groups increased their knowledge from the baseline. That is, the acquisition of longitudinal knowledge (comparison between the pretest and the 3 rd assessment) was recorded in both arms of the study, being significantly higher by those who were in front of the anatomical table ( p = 0.040). However, cross-sectionally there was no statistically significant difference between the two interventions in the two evaluations that took place after the instruction phase of the study.
These results may be justified by the fact that the anatomical table reproduced structural features of the real organ, facilitating the learning of visuo-spatial relationships to a level of detail that may not be attainable for visualization by any other means (especially the internal liver segments), including the real organ. 10 For instance, the group allocated to the real liver did not visualize portal vein branches in loco (they were not displayed separately from the liver parenchyma). Through the transparency control feature, the group allocated to the table could see, in the same image (preserved liver silhouette), not only the entire course of the intrahepatic vessels, but also their spatial correlation with each other or with other structures, 15 such as a Couinaud’s segment.
In addition to the learning outcome, a relevant finding of this study was the level of satisfaction with the anatomical table found among students. At least in theory, it is possible that more attractive resources will make students more interested and spend more time studying anatomy. On the other hand, this additional time spent on anatomical study and review could introduce an interference in the use of time dedicated to studying, as students may fail to prioritize other important areas of the medical course. This paradox should be considered when indicating the usefulness of the anatomical table. Nevertheless, similar findings have been previously reported 16 , 17 and may represent a more convincing argument for the development of interactive 3D teaching tools.
In a research similar to this protocol, Venis et al. 18 carried out a comparative study evaluating the effectiveness of the 3D virtual anatomical table (Anatomage/software 3.0) versus anatomical models aimed to learning knee anatomy in 12 medical students. Similarly, the researchers applied three tests (one pretest (before instruction), one post-test (with technical questions, as well as self-satisfaction questions), and one last test 2 weeks after the end of the protocol to assess information retention. The participants allocated to the anatomical table group showed significantly better results in the two regular post-instructional assessments ( p -0.020; and p -0.047). The perception of satisfaction was also higher among the students who used the anatomical table (score in the Likert scale of 4.6 versus 3.2 points). 18
In a broader context, the results that express effectiveness and satisfaction regarding the use of 3D resources bring in parallel an important counterpoint to the paradigm of the need for the use of cadavers and structures in situ in the teaching of anatomy. First, there is no doubt that actual anatomical structures represent the standard of reference for understanding the three-dimensional component of the human body through observation and discovery. 19 Second, this helps the formation of the spatial reasoning necessary for the understanding and interpretation of the information provided by the image. However, preserved real anatomical structures do not always provide an accurate impression of the living body and are a source of emotional unrest for some students. 19 From another perspective, the time set aside by educational institutions for the traditional learning of gross anatomy through visual and tactile experience of the actual structure has been reduced by incorporating active learning methods (such as problem-based learning), 19 a fact that has forced experts to rethink how to teach anatomy.
Against this perspective, Costa e Lins 20 reported that the use of human corpses, even if only for demonstration of anatomical structures in class, was considered indispensable to the teaching-learning process in the study of human anatomy by 542 students from different health courses, mainly because they considered that the handling of the corpse represented a way to strengthen the humanization of the conduct of future health professionals. 20 Although the anatomical table has been able to provide a level of information similar to the real liver and is a device that has some advantages over the organ in situ (for example, it does not use formaldehyde; it allows for “virtual dissection” as often as necessary, etc.), these findings do not support the hypothesis that the anatomical table can replace the structures in situ in the teaching of anatomy, mainly because this study has important limitations.
The effectiveness of three-dimensional resources in the teaching of hepatobiliary anatomy is demonstrated in several works 3 , 15 with some nuances between them. Unlike this study, Beerman et al. 15 and Jurgaitis et al. 3 did not use a pretest in their research protocols, which brings out the possibility that the difference found in the results of these studies was influenced by a greater prior knowledge of the students allocated to the 3D group. In our study, although the pretest performance was measured (showing no statistically significant difference between groups ( p = 0.290), we did not assess other variables that could interfere with the final research results.
For instance, this is the case with the innate spatial ability. 21 Spatial abilities consist of visualization, orientation and manipulation of structures in space. 22 Spatial abilities have been related to knowledge of three-dimensional anatomy (3D), being applied in practical exams (identification), topographic questions, among others. 25 Based on this information, Hegarty et al. 23 identified a model capable of expressing individual differences regarding the performance in some of these areas, attributed to innate spatial abilities (Hegarty, 2007). It is possible, therefore, that students have different levels of spatial abilities and this may have affected the results of this research. Second, our sample was considerably small, possibly unable to reliably demonstrate differences in estimates of the intervention effect.
In conclusion, the 3D virtual anatomical table improved the knowledge of hepatobiliary anatomy for medical students in relation to their previous knowledge of these structures. In the cross-sectional comparison of post-instructional evaluations, there was no difference between the two interventions. Moreover, the 3D platform had a positive impact on the satisfaction level of the study participants. This study shows that the 3D virtual anatomical table has the potential to improve medical students’ understanding and interest in anatomy. Therefore, it is recommended that future protocols such as this be performed with larger samples and exploring other anatomical structures.
CHART 3 Result of self-satisfaction assessment
| TOPIC / QUESTION | Discordant (%)* | ||
|---|---|---|---|
| G1 Anatomical table | G2 Real liver | Total | |
| 1) I feel satisfied with the pedagogical resource that was used for my learning. | 0.0 | 0.0 | 0.0 |
| 2) I consider that the teacher took full advantage of the learning resource used to teach the subject in question. | 10.0 | 0.0 | 5.0 |
| 3) The resource used in class facilitated my assimilation of knowledge. | 0.0 | 0.0 | 0.0 |
| 4) I feel able to reproduce the knowledge I learned based on the class I had. | 0.0 | 10.0 | 5.0 |
| 5) I was stimulated to learn through the resource used during the activity. | 0.0 | 10.0 | 5.0 |
| 6) I am motivated to reuse the resource that was utilized in the activity. | 0.0 | 0.0 | 0.0 |
| 7) I am not satisfied with the pedagogical resource that was used for my learning. | 100.0 | 80.0 | 90.0 |
| 8) I do not consider that the teacher took full advantage of the learning resource used for teaching the subject in question. | 90.0 | 100.0 | 95.0 |
| 9) The resource used in class did not facilitate my assimilation of knowledge. | 100.0 | 100.0 | 100.0 |
| 10) I do not feel able to reproduce the knowledge I learned based on the class I had. | 90.0 | 90.0 | 90.0 |
| 11) I was not encouraged to learn through the resource used during the activity. | 70.0 | 90.0 | 80.0 |
| 12) I am not motivated to reuse the resource that was utilized in the activity. | 90.0 | 90.0 | 90.0 |

