










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format
 Send this article by e-mail
Send this article by e-mailShare

 Permalink
PermalinkRevista Brasileira de Educação Médica
Print version ISSN 0100-5502On-line version ISSN 1981-5271
Rev. Bras. Educ. Med. vol.47 no.4 Rio de Janeiro 2023 Epub Oct 18, 2023
https://doi.org/10.1590/1981-5271v47.4-2022-0300
ORIGINAL ARTICLE
Resilience and spirituality of Medicine students during social isolation due to the Covid-19 pandemic
1
, research design, data collection, data analysis, discussion of results, writing of the manuscript http://orcid.org/0000-0002-2135-1120
http://orcid.org/0000-0002-2135-1120
1
, research design, data collection, data analysis, discussion of results, writing of the manuscripthttp://orcid.org/0000-2287-4513
2
, research design, data collection, data analysis, discussion of results, writing of the manuscripthttp://orcid.org/0000-0002-5504-0048
3
, research design, data collection, data analysis, discussion of results, writing of the manuscripthttp://orcid.org/0000-0002-9042-3562
1
, research design, data collection, data analysis, discussion of results, writing of the manuscript, review and approval of the final version of the manuscript, working as advisors of the entire processhttp://orcid.org/0000-0002-2684-0142
1
, review and approval of the final version of the manuscript, working as advisors of the entire processhttp://orcid.org/0000-0002-1884-5680
1 Universidade José do Rosário Vellano, Belo Horizonte, Minas Gerais, Brazil.
2 Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
3 Universidade Federal de Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil.
Introduction:
The COVID-19 pandemic had a negative impact on the mental health of university students. In this period of uncertainty and challenges, the development of resilience, that is, the ability to deal with and recover from adverse situations, was necessary. From the perspective of social isolation, spirituality is shown to be an important resource for resignification, which can have a positive impact on students’ resilience.
Objective:
To identify the degree of resilience of medical students during the social isolation caused by COVID-19 and its relationship with spirituality and personal factors.
Methodology:
A mixed cross-sectional study carried out with medical students from Brazilian private and public institutions. Data were collected from June to September 2020 using a questionnaire containing sociodemographic and opinion questions about positive and negative aspects of social isolation, the Resilience Scale and the Spirituality-Related Attitudes Scale (ARES). For the analysis of the open responses to the questionnaire, a content analysis was performed with categorization of responses by topic.
Result:
308 students participated in the study. The average scores found showed that the students showed moderate resilience and high spirituality. A weak positive correlation was observed between the degree of spirituality and resilience. The variables that positively impacted both resilience and spirituality were high level of satisfaction in studying to become a doctor, high level of happiness with life in recent months, better quality of life during isolation, having a religion and high importance attributed to the fact of having a religion. Female students aged over 25 years old showed greater spirituality. The most often cited positive points were related to social relationships, leisure and personal development. The most frequent negative points and difficulties were mental-physical-social health and remote teaching/adaptation to a new routine.
Conclusion:
The study suggests that students with greater spirituality are more resilient, being better able to deal with stressors; to adapt and have a positive view of adverse situations. These results can contribute to a reflection on educational strategies that aim to help students in coping with stressful situations, such as those experienced as a result of social isolation.
Keywords: Spirituality; Psychological resilience; Medical students; Pandemic; Medical education
Introdução:
A pandemia da Covid-19 repercutiu de forma negativa na saúde mental dos estudantes universitários. Nesse período de incertezas e desafios, o desenvolvimento de resiliência, isto é, a capacidade de lidar com situações adversas e se recuperar, fez-se necessário. Sob a ótica do isolamento social, a espiritualidade se mostra como um recurso importante de ressignificação, podendo exercer impacto positivo na resiliência dos estudantes.
Objetivo:
Este estudo teve como objetivo identificar o grau de resiliência dos estudantes de Medicina durante o isolamento social causado pela Covid-19 e sua relação com a espiritualidade e fatores pessoais.
Método:
Trata-se de um estudo transversal misto realizado com estudantes de Medicina de instituições privadas e públicas brasileiras. Os dados foram coletados no período de junho a setembro de 2020 utilizando um questionário com perguntas sobre aspectos sociodemográficos e referentes à opinião acerca de pontos positivos e negativos do isolamento social, a Escala de Resiliência e a Escala de Atitudes Relacionadas à Espiritualidade (ARES). Para exame das respostas abertas do questionário, fez-se uma análise de conteúdo com categorização delas por temas.
Resultado:
Participaram do estudo 308 estudantes. Os escores médios encontrados demonstraram que os estudantes apresentaram moderada resiliência e alta espiritualidade. Observou-se correlação positiva fraca entre grau de espiritualidade e resiliência. As variáveis que impactaram positivamente tanto a resiliência quanto a espiritualidade foram alto nível de satisfação em estudar para ser médico, alto nível de felicidade com a vida nos últimos meses, maior qualidade de vida durante o isolamento, possuir religião e alta importância atribuída ao fato de ter uma religião. Estudantes do sexo feminino e na faixa etária acima de 25 anos apresentaram maior espiritualidade. Os pontos positivos mais citados estavam relacionados com relações sociais, lazer e desenvolvimento pessoal. Os pontos negativos e as dificuldades mais frequentes foram saúde mental-física-social e ensino remoto/adaptação a uma nova rotina.
Conclusão:
O estudo sugere que estudantes que apresentam maior espiritualidade são mais resilientes, sendo mais capazes de lidar com fatores estressores, adaptar-se e ter uma visão positiva em relação a situações adversas. Esses resultados podem contribuir para uma reflexão sobre estratégias educacionais que visem auxiliar os estudantes no enfrentamento de situações estressoras, como a vivenciada em decorrência do isolamento social.
Palavras-chave: Espiritualidade; Resiliência Psicológica; Estudantes de Medicina; Pandemia; Educação Médica
INTRODUCTION
The COVID-19 pandemic, declared by the World Health Organization in March 2020, had consequences throughout the world, having a dramatic impact on health, with countless deaths and hospitalizations; on the economic sphere, with isolation measures and on the social sphere with emotional and behavioral disorders1. In Brazil, studies show the impacts of COVID-19 on the mental health of the general population, with increased anxiety, insomnia, hyperactivity, depression, among other health problems generated by fear, financial difficulties and social isolation2.
In the academic scenario, across the world, the pandemic resulted in the widespread closing of educational institutions, such as schools, colleges and universities3. In Brazil, the Ministry of Health authorized the replacement of face-to-face classes by digital ones (except traineeships, laboratory practices and, for medical courses, internships)4.
Factors such as delays in continuing the course, the interruption of practical classes and curricular internships as well as, in some Universities, the carrying out of remote activities, resulted in concerns about Internet access and difficulties in adapting to the new learning method, with a negative impact on the mental health of university students. Moreover, aspects such as the disruption in academic routines, separation from friends and concerns about course delays also contributed to the worsening of the mental health of undergraduate students during this pandemic period5. Another factor of concern is related to the loss of learning and skills resulting from this moment, which could have an impact on the acquisition of skills expected in the medical profession.
Despite the difficulties experienced by students caused by the COVID-19 pandemic, studies on student adversities in other scenarios demonstrate that some students, even seriously disadvantaged ones, are capable of overcoming the challenges and achieving results at levels considered to be superior6. It is observed, therefore, that some individuals respond differently to traumatic situations, being able to recover from a destabilizing event, resisting initially, and then overcoming it, projecting themselves into the future7.
This is the phenomenon of resilience, which is the human capacity to face, overcome and be strengthened or transformed by adverse experiences8. The topic of resilience in student environments has aroused the interest of researchers, as it is related to good academic performance. Three types of resilience are described: emotional, academic and social. The emotional type is related to feelings that favor the ability to adapt; while academic resilience refers to the school environment as a facilitator of learning to solve problems and social resilience deals with relationships and social models that also provide support for facing and overcoming problems9.
Three characteristics are considered essential for a person to be resilient: the ability to accept reality, the ability to improvise and the ability to find meaning in some aspect of life10. Resilience results from the interaction between risk-promoting factors and personal resources, with the latter comprising two motivational processes: the need to defend oneself against danger, and the need to achieve positive objectives11. The protective factors that contribute to overcoming adversity, also called pillars of resilience, are: self-esteem, personal skills and competencies, sense of humor and spirituality7.
Spirituality favors adaptation in the face of life’s inevitable difficulties, functioning as a protective factor, as it alleviates the individual’s stress and vulnerability10. Studies have also demonstrated that, when under stressful situations, spiritualized individuals have more resilience and consequently, deal better with the difficulties imposed on them12)-(14.
According to Cunha, Rossato and Scorsolini-Comin15, the growing interest in investigating the influence of spirituality and religion on health brings about the need to better conceptualize the terms religion, religiosity and spirituality, which are used in national and international research. Religion is the organized system of beliefs, practices, rituals and symbols designed to facilitate access to the sacred (God, the greater force, the supreme truth). Religiosity refers to how much an individual believes, follows and practices a particular religion. Spirituality can be defined as that which brings meaning and purpose to people’s lives16),(17.
According to Saad and Medeiros18, Garfield, Isacco and Sahker19 and Gnanaprakash20, spiritual involvement improves the psychological state, by stimulating hope, forgiveness, altruism and love, which have a positive impact on coping with stressful situations, leading to a better state of well-being and of mental health.
It is in this sense that spirituality represents the soul of resilience, as a human disposition capable of awakening the feeling of unity with others, with the world and with nature, permeating the interrelationships of deeper affections, promoting more effective bonds, capable of developing competencies that are necessary for more resilient results. Faith, the conviction of belonging to the universe, of being part of a supreme purpose, brings responsibilities, sense and meaning to one’s existence and is capable of providing the individual with fundamental devices to deal with adversity21.
The positive effect of spirituality in alleviating psychological suffering has already been demonstrated in the general population6 and in medical students18. Wachholtz and Rogoff22 suggested that spirituality can be considered a protective factor when facing adversity. According to Lucchetti G et al.23 studies have demonstrated an association between greater spirituality and improvements in mental health, clinical outcomes, general well-being, quality of life and greater survival.
The context experienced by people when faced with the COVID-19 pandemic, considering social isolation and the deprivation of interaction in the school environment, required coping strategies from students that could promote a (re)construction of the meaning of life. From this perspective, spirituality has been shown to be an important resource for resignification, facilitating the capacity for strength in the face of adversity24.
Thus, in this unique scenario experienced by all humankind when facing the COVID-19 pandemic, knowledge about the factors that influence the resilience capacity of medical students, especially spirituality, is necessary and opportune to support curricular strategies aimed at promoting the resilience of medical students, as a measure to face adversities experienced throughout the course.
METHODOLOGY
A cross-sectional, mixed study was carried out, conducted using a self-answered questionnaire to assess resilience and spirituality in medical students.
A total of 309 medical students from 44 Brazilian public and private educational institutions participated in the study. The inclusion criteria were being regularly enrolled in a Brazilian medical teaching institution and being over 18 years old. For recruitment, the “snowball” technique was employed, which uses reference networks and is appropriate for sampling in groups that are difficult to access and when there is no precision regarding the number of assessed subjects25. Medical students (regardless of the year or period they were attending) were invited to participate in the study through WhatsApp or email, which contained a link to access the questionnaire, of which header contained the information necessary to participate in the study, including the Free and Informed Consent form, which had to be digitally signed before filling out the questionnaire. Participants were assured of the confidentiality of the collected data, which would be analyzed together, and the identification of any student was not disclosed. This study was approved by the Research Ethics Committee of José do Rosário Vellano University (CAAE: 32131020.3.0000.514 and Opinion number 4.248.876)
From June to August 2020, a questionnaire was administered that contained closed questions addressing sociodemographic aspects; the Resilience scale developed by Wagnild and Young26; the scale of Attitudes Related to Spirituality, developed by Braguetta27 and three open questions in which students were asked to cite the positive, negative points and difficulties experienced during social isolation.
The following tools were used:
Sociodemographic questionnaire consisting of 12 closed questions regarding the variables: gender, age, course period, marital status, family income, desired specialty, degree of happiness in recent months; degree of satisfaction with studying medicine; assessment of one’s quality of life; concept of spirituality and three open questions about their opinion regarding the positive, negative points and difficulties when facing social isolation, with the aim of identifying possible risk-promoting factors (negative points and difficulties) and protective factors (positive points) related with student resilience.
Resilience scale: developed by Wagnild and Young26 to measure levels of positive psychosocial adaptation in the face of important life events. It has 25 items described in a positive way with a Likert-type response format, ranging from 1 (totally disagree) to 7 (totally agree). The scale scores range from 25 to 175 points, with score values up to 120 indicating reduced resilience; scores from 121 to 145 indicating moderate resilience and scores above 145 indicating moderately high or high resilience, indicting high degree of resilience. Studies have shown good reliability and validity of this instrument26, which has been adapted to the Portuguese language27.
Attitudes Related to Spirituality Scale (ARES): scale developed by Braguetta28 based on the understanding of spirituality in the Brazilian context and on theoretical bases. It presented appropriate psychometric analyses and was validated with medical students. It contains 11 items, with a Likert-type response format ranging from 1 (strongly disagree) to 5 (strongly agree). Scale scores range from 11 to 55. Score values up to 38 indicate low spirituality; between 39 and 45, moderate spirituality and above 45, high spirituality.
Quantitative data were analyzed using the SPSS v.17.0 program. In this study, the descriptive measures Minimum, Maximum, Median, Mean values and standard deviation (SD) were presented, in addition to percentages as measures to describe the results of the studied variables. The Chi-square test was used for categorical variables; the Mann-Whitney test for ordinal variables, Pearson’s correlation for scalar variables and the Kruskal-Wallis test for comparison between independent groups in relation to the variable of interest. All results were considered significant for a significance probability of less than 5% (p < 0.05).
All discursive responses were placed in a table for analysis and the participants’ anonymity was ensured by adopting numbers in the identification. Each student was identified with the letter “S” followed by a number, according to the sequence of respondents to the questionnaire (S1, S2, and so forth). The propositions of the thematic content analysis technique proposed by Bardin29) were used as a reference for the analysis, in relation to the stages: floating reading and categorization. The “floating reading” was carried out with the aim of familiarizing oneself with the material. Then, the students’ responses to each question were analyzed, defining the main ideas or feelings demonstrated that gave rise to the categories. Immediately after defining the categories, all responses were analyzed individually by three researchers who had to select the category to which each one belonged. Thereafter, a consensus analysis of the questions was carried out. Those for which there was no agreement between the researchers were evaluated again until a consensus was reached.
Sample characterization
A total of 308 medical students participated in the study, 80.4% from institutions located in the Southeast region (n=248); 10% in the Midwest region (n=31); 4.3% in the Northeast region (n=13); 4.3% in the South region (n=13) and 1% in the North region of the country (n=3). Of these, 72.1% were female (n=222); 78.6% aged between 18 and 24 years old (n=242); 93% were single (n=287); 53.4% declared a family income greater than ten thousand reais (n=163) and 84.1% of the students (n=259) reported living with their family (father and mother). Regarding the course period, 72.4% (n=222) were attending the first half of the course (1st, 2nd or 3rd year) and 27.6% (n=85) the second half of the course (4th, 5th or 6th year). Among the participants, 43.5% (n=134) declared they wanted to pursue a clinical and surgical specialty, 39.9% (n=123) wanted a clinical specialty and 16.6% (n=51) a surgical specialty. Regarding one’s level of satisfaction with studying medicine, 48.4% (n=149) reported being very satisfied, 35.7% (n=110) were moderately satisfied and 15.9% (n=49) reported being little satisfied or very dissatisfied.
Among the students, 12.3% (n=38) considered themselves very happy with life in the last few months, while 53.2% (n=164) considered themselves happy, 32.1% (n=99) not very happy and 2.3% (n=7) were unhappy. Regarding quality of life, 27.9% (n=86) classified it as very good, 42.5% (n=131) as good, 22.7% (n=70) as reasonable and 6.8% (n=21) as bad or very bad.
Regarding religion, 73.7% (n=227) declared having a religion; 26.3% (n=81) declared that they did not have any religion; 72% (n=222) considered having a religion to be important or very important and 28% (n=86) considered having a religion to be of little importance or not at all important. Regarding the concept of spirituality, 59.7% (n=184) of the students indicated it as the search for the sense and meaning of human life; 55.5% (n=171) as the belief in something that transcends matter; 50.3% (n=155) reported their belief in and relationship with God/religiosity; 40.9% (n=126) indicated an ethical and humanistic attitude and 32.8% (n=101) a belief in the existence of the soul and life after death (Table 1).
Table 1 Characterization of medical students according to personal data.
| Variable | Frequency N (%) |
|---|---|
| Sex | |
| Female | 222 (72.1%) |
| Male | 86 (27.9%) |
| Total | 308 (100.0%) |
| Age range | |
| 18 to 24 years | 242 (78.6%) |
| 25 to 30 years | 44 (14.3%) |
| > 30 years | 22 (7.1%) |
| Total | 308 (100.0%) |
| Marital status | |
| Single | 287 (93.2%) |
| Married | 10 (3.3%) |
| Common-law marriage | 9 (2.9%) |
| Divorced | 1 (0.3%) |
| Widowed | 1 (0.3%) |
| Total | 308 (100.0%) |
| Family income | |
| Up to R$10,000.00 (ten thousand reais) | 142 (46.6%) |
| > R$10,000.00 (ten thousand reais) | 163 (53.4%) |
| Total | 305 (100.0%) |
| 3 cases without information | |
| With whom do you live | |
| Family (father and mother) | 259 (84.1%) |
| Alone | 26 (8.5%) |
| Relative | 18 (5.8%) |
| Total | 308 (100.0%) |
| Year of the course | |
| 1st year | 97 (31.6%) |
| 2nd year | 66 (21.5%) |
| 3rd year | 59 (19.3%) |
| 4th year | 35 (11.4%) |
| 5th year | 25 (8.1%) |
| 6th year | 25 (8.1%) |
| Total | 307 (100.0%) |
| 1 case without information | |
| Specialty you intend to follow | |
| Surgical | 51 (16.6%) |
| Clinical | 123 (39.9%) |
| Clinical-Surgical | 134 (43.5%) |
| Total | 308 (100.0%) |
| Satisfaction with studying medicine | |
| Very dissatisfied | 12 (3.9%) |
| A little satisfied | 37 (12.0%) |
| Moderately satisfied | 110 (35.7%) |
| Very satisfied | 149 (48.4%) |
| Total | 308 (100.0%) |
| Degree of happiness with one’s life | |
| Very happy | 38 (12.3%) |
| Happy | 164 (53.2%) |
| Not very happy | 99 (32.1%) |
| Unhappy | 7 (2.3%) |
| Total | 308 (100.0%) |
| Quality of life at that moment | |
| Very good | 86 (27.9%) |
| Good | 131 (42.5%) |
| Regular | 70 (22.7%) |
| Bad | 19 (6.2%) |
| Very bad | 2 (0.6%) |
| Total | 308 (100.0%) |
| Do you have a religion? | |
| Yes | 227 (73.7%) |
| No | 81 (26.3%) |
| Total | 308 (100%) |
| Importance of having a religion | |
| No importance | 18 (5.9%) |
| Little importance | 68 (22.1%) |
| Important | 95 (30.8%) |
| Very important | 127 (41.2%) |
| Total | 308 (100.0%) |
| Concept of spirituality | |
| Search for the sense and meaning of human life | 184 (59.7%) |
| Belief in something that transcends matter | 171 (55.5%) |
| Belief in and relationship with God/religiosity | 155 (50.3%) |
| Ethical and humanistic attitude | 126 (40.9%) |
| Belief in the existence of the soul and life after death | 101 (32.8%) |
| Total | 308 (100.0%) |
Source: study data.
Resilience of medical students
The average score achieved by students during the social isolation imposed by the COVID-19 pandemic was 135.9 ± 17.8, demonstrating moderate resilience, with 29.9% (n=92) showing moderately high to high resilience, 51.9% (n=160) moderate resilience and 18.2% (n=56) reduced resilience.
Greater resilience was influenced by a high level of satisfaction in studying to be a physician, high level of happiness with one’s life in recent months, greater quality of life during isolation, having a religion and high importance attributed to having a religion (Table 2). Higher agreement scores (very and completely) were observed for the statements; “I feel proud of having accomplished things in my life” by 85.7% of students (n=264) and “Maintaining an interest in things is important to me” by 85.3% (n=263). The lowest agreement scores were observed for the statements “I feel like I can handle several things at the same time” by 18.8% (n=58) and “I do things one day at a time” by 9.1% (n=28).
Table 2 Assessment of the influence of sociodemographic data on the spirituality and resilience score of medical students during social isolation due to the COVID-19 pandemic, 2020.
| Variable | Spirituality | Resilience | ||||
|---|---|---|---|---|---|---|
| P50 (P25 - P75) | Mean ± SD | p | P50 (P25 - P75) | Mean ± SD | p | |
| Gender | ||||||
| Female | 52.0 (44.0; 54.0) | 47.3 ± 9.8 | 0.006 | 137.0 (126.0; 149.0) | 136.4 ± 16.3 | 0.903 |
| Male | 48.0 (35.0; 53.0) | 43.0 ± 12.7 | 138.0 (124.8; 149.0) | 134.5 ± 21.1 | ||
| Age range | ||||||
| 18 to 24 years | 50.0 (41.0; 54.0) | 45.5 ± 11.1 | 0.046 | 137.0 (125.8; 149.0) | 136.0 ± 17.6 | 0.947 |
| 25 years or older | 52.0 (46.5; 55.0) | 48.2 ± 9.6 | 137.0 (125.0; 150.0) | 135.6 ± 18.5 | ||
| Marital status | ||||||
| Single | 50.0 (42.0; 54.0) | 45.9 ± 11.0 | 0.144 | 137.0 (125.0; 149.0) | 135.5 ± 17.9 | 0.223 |
| Other marital status | 52.0 (47.0; 55.0) | 49.6 ± 7.4 | 138.0 (132.0; 155.0) | 141.1 ± 15.0 | ||
| Family income | ||||||
| Above R$10,000.00 | 50.0 (41.0; 53.0) | 45.5 ± 11.2 | 0.253 | 137.0 (126.0; 149.0) | 136.7 ± 17.0 | 0.586 |
| Up to R$10,000.00 | 51.5 (43.0; 54.3) | 46.6 ± 10.5 | 137.0 (124.8; 148.3) | 134.9 ± 18.7 | ||
| With whom do you currently live? | ||||||
| Family (father and mother) | 51.0 (42.0; 54.0) | 46.3 ± 10.7 | 0.652 | 137.0 (125.0; 149.0) | 135.7 ± 17.9 | 0.935 |
| Other people | 50.0 (38.0; 53.5) | 45.1 ± 11.8 | 137.0 (125.0; 149.0) | 136.6 ± 17.4 | ||
| Year at medical school | ||||||
| 1st or 2nd year | 52.0 (41.0; 54.0) | 46.3 ± 10.8 | 0.234 | 138.0 (126.0; 150.0) | 136.6 ± 18.4 | 0.285 |
| 3rd or 4th year | 50.0 (44.0; 540) | 46.9 ± 10.1 | 134.5 (123.5; 146.0) | 133.8 ± 16.8 | ||
| 5th or 6th year | 48.5 (40.0; 53.0) | 44.0 ± 12.2 | 137.0 (126.8; 150.3) | 137.3 ± 17.6 | ||
| Desired medical specialty | ||||||
| Surgical | 51.0 (40.0; 54.0) | 44.4 ± 13.4 | 0.265 | 140.0 (129.0; 152.0) | 139.1 ± 15.2 | 0.286 |
| Clinical | 49.0 (41.0; 54.0) | 45.3 ± 11.1 | 136.0 (120.0; 150.0) | 134.0 ± 19.6 | ||
| Clinical-surgical | 52.0 (44.0; 54.0) | 47.5 ± 9.3 | 137.5 (127.8; 148.0) | 136.3 ± 16.8 | ||
| Satisfaction with studying medicine | ||||||
| Very dissatisfied or little satisfied | 46.0 (35.5; 53.0) | 43.0 ± 11.6 | 0.002 | 129.0 (113.0; 139.5) | 126.8 ± 19.8 | < 0.001 |
| Moderately satisfied | 48.0 (40.0; 54.0) | 44.8 ± 11.4 | 134.0 (123.0; 143.0) | 131.5 ± 18.1 | ||
| Very satisfied | 52.0 (47.0; 54.5) | 48.1 ± 9.8 | 143.0 (132.0; 153.0) | 142.1 ± 14.4 | ||
| Level of happiness with one’s life in the recent months | ||||||
| Very happy / Happy | 52.0 (45.0; 55.0) | 47.4 ± 10.1 | 0.001* | 142.0 (131.8; 152.0) | 140.8 ± 15.2 | < 0.001* |
| Not very happy / Unhappy | 48.0 (38.8; 53.0) | 43.7 ± 11.7 | 129.0 (116.0; 139.0) | 126.6 ± 18.7 | ||
| Quality of life at this moment | ||||||
| Very good | 52.0 (45.0; 55.0) | 47.7 ± 10.0 | 0.064** | 144.0 (132.0; 153.0) | 142.2 ± 14.5 | < 0.001** |
| Good / Regular | 50.0 (42.0; 54.0) | 45.7 ± 11.0 | 135.0 (123.0; 147.0) | 134.4 ± 17.8 | ||
| Bad / Very bad | 47.0 (35.5; 52.5) | 43.0 ± 12.0 | 132.0 (111.5; 138.5) | 124.7 ± 21.4 | ||
| Do you have a religion? | ||||||
| No | 38.0 (25.5; 48.0) | 36.0 ± 13.5 | < 0.001* | 135.0 (125.5; 144.0) | 132.1 ± 16.5 | 0.026* |
| Yes | 52.0 (47.0; 55.0) | 49.7 ± 6.8 | 139.0 (125.0; 151.0) | 137.2 ± 18.1 | ||
| Importance of having a religion | ||||||
| None or little importance | 38.0 (26.0; 48.3) | 36.4 ± 13.4 | < 0.001** | 134.5 (125.8; 144.3) | 133.7 ± 15.5 | 0.016** |
| Important | 47.0 (42.0; 52.0) | 45.8 ± 8.0 | 137.0 (120.0; 147.0) | 133.2 ± 19.9 | ||
| Very important | 54.0 (52.0; 55.0) | 52.9 ± 2.6 | 141.0 (129.0; 153.0) | 139.3 ± 17.1 | ||
Database: study data.
Note: the probability of significance refers to the Mann-Whitney test (*) and the Kruskal-Wallis test (**)
Spirituality among medical students
The average scores found among medical students during the social isolation imposed by the COVID-19 pandemic was 46.1 ± 10.8, demonstrating high spirituality, with 67.9% (n=209) of students having high spirituality, 13 6% (n=42) moderate spirituality and 18.5% (n=57) showing low spirituality. A higher degree of spirituality observed was correlated with female gender, age group over 25 years old, high level of satisfaction in studying to become a physician, high level of happiness with life in recent months, having a religion and high importance attributed to the fact of having a religion (Table 2). Higher agreement scores were observed for the statements “I believe in something sacred, transcendent (God, a superior force)” by 75% (n=231) of the students and “My spirituality encourages me to help other people” by 65.9% (n=203). The lowest agreement scores were observed for the statements: “My beliefs and spiritual values direct my actions on a daily basis” by 42.9% (n=132) and “My faith or spiritual beliefs give meaning to my life” by 48% ( n=148).
Correlation between the degree of resilience and spirituality observed in medical students during social isolation
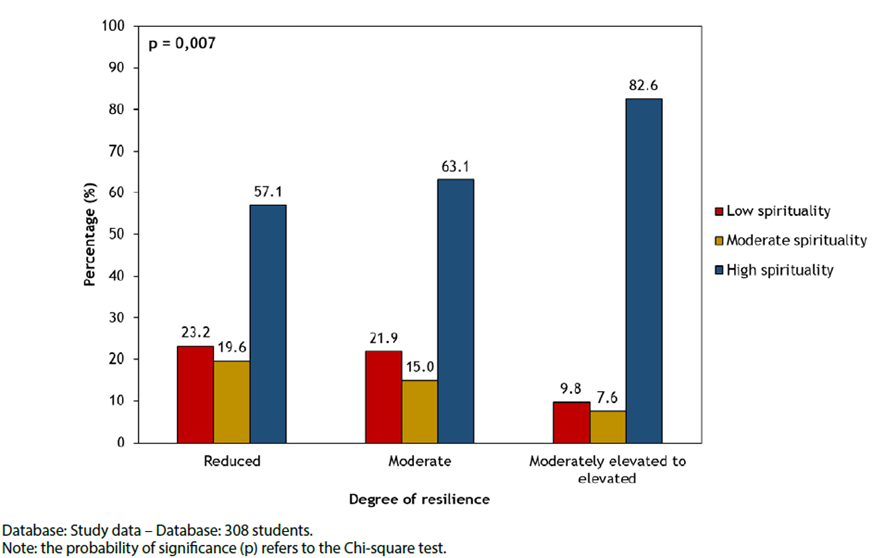
A significant, positive and weak correlation was observed between the degree of spirituality and the degree of resilience (r=0.267, p<0.001 - Pearson’s correlation), with the group that showed greater resilience having the highest percentage of students with high spirituality (Graph 1).
Categorization of medical students’ responses in relation to the positive, negative points and difficulties experienced in social isolation during the pandemic.
Regarding the positive points reported, four categories were obtained: (1) Social relationships; (2) Leisure and personal development; (3) Social concerns; (4) Saving time and money. Regarding the negative points reported, four categories were obtained: (1) Social, economic and political concerns; (2) Coexistence conflicts; (3) Social life, physical and mental health (4) Remote teaching and changes in routine. In relation to the reported difficulties, four categories were obtained: (1) Social life, physical and mental health; (2) Coexistence conflicts; (3) Remote teaching and adaptation to a new routine (4) Adaptation to new individual and collective protection measures. (Chart 1).
Chart 1 Categorization of medical students’ responses in relation to the positive, negative points and difficulties experienced in social isolation during the pandemic.
| CATEGORIES | DESCRIPTION | RESPONSES |
|---|---|---|
| POSITIVE POINTS | ||
| 1. Social relationships | Reports that considered that confinement made it possible to bring social interactions closer together. | “Spending time with my family, which I didn’t have the opportunity to do before.” (S 56) |
| “Being closer to my family.” (S83) | ||
| 2. Leisure and personal development | Reports that considered having more time for leisure and the possibility of personal development, including self-care, self-knowledge and studies as positive points of the confinement. | “Self-knowledge, possibility of improving patience, resilience.” (S4) |
| “My reunion with myself” (S18) | ||
| “More time for individual activities such as studying, reading, weight training and meditation.” (S49) | ||
| “Opportunities to develop spirituality, self-control, and reestablish priorities.”(S84) | ||
| 3. Social concerns | Reports that considered the very objective of confinement as a public health measure to be positive, that is, raising awareness of the population about the current scenario and the need to change habits to reduce contagion and the possibility of more time to prepare health systems. | “Lower incidence of contagion, better preparedness of the health system” (S38) |
| “Reduce the flow of people in large centers and strengthen the understanding of a moment that requires changes in lifestyle” (S93) | ||
| “Greater development from a social perspective, rather than just an individual one.” (S87) | ||
| 4. Saving time and money. | Reports that considered that changing habits during the confinement allowed better optimization of time and saving money. | “Not spending time on transport to go to the University, eating food at home without it being heated in the microwave” (S63) |
| “Having time to do things at home” (S65) | ||
| “Not having to travel to go to work…” (S74) | ||
| “[...] having lunch at home, less traffic/travel time to go to the university” (S86) | ||
| NEGATIVE POINTS | ||
| 1 Social, economic and political concerns | Reports of negative repercussions of the pandemic and confinement in the social, political and economic field, such as unemployment, deaths and increased social inequality. | “Drastic economic and social changes in the country” (S65) |
| “Economic setback” (S111) | ||
| 2. Coexistence conflicts | Reports of conflicts with people one interacts with on a daily basis, either due to increased time spent together and less privacy, such as people who had to return to their parents’ house, or due to conflicts with people who did not follow the measures to fight COVID- 19. | “A lot of interaction with my parents” (S42) |
| “[...] having to fight with people to follow directions [...]” (S65) | ||
| 3. Social life, physical and mental health | Reports that cite as negative points of the quarantine the damage to one’s mental and physical health, as well as a feeling of loneliness. | “Social distancing. It’s hard to be away from the people you love, not being able to hug, talking in person.” (S18) |
| “[...] Difficulty exercising and eating is worse”. (S48) | ||
| “Increase in anxiety attacks.” (S56) | ||
| 4. Remote teaching and changes in routine | Reports that consider that confinement was detrimental to academic life, as well as requiring an adaptation to Emergency Remote Teaching and a new routine without leaving home. | “Studying remotely, missing part of classes due to the internet, less concentration, worse performance, more fatigue, less learning, more work.” (S89) |
| “Modifying my routine, not being able to vary where I study, depending on internet access and quality for classes, interruptions during classes by the family” (S86) | ||
| DIFFICULTIES | ||
| 1. Social life, physical and mental health | Reports that considered that the confinement period brought difficulties in social life, mental health and physical health. | “Being without physical activity and without seeing friends” (S14) |
| “Fear, uncertainty about the future.” (S51) | ||
| “Difficulties regarding not going out with friends to bars/parties; increased anxiety [...]” (S108) | ||
| 2.Coexistence conflicts | Reports that considered that the confinement period brought challenges in adapting to coexistence inside the home. | “[...] adapting to living with my parents again.” (S7) |
| “Being with my parents, since I hadn’t lived with them for a long time.” (S74) | ||
| “[...] Also, living with family, even though it is something positive, becomes a complication when it is necessary to concentrate on classes, tests and I cannot be interrupted.” (S86) | ||
| 3. Remote teaching and adaptation to a new routine | Reports that considered that the confinement period brought difficulties regarding the remote teaching and adapting to a new routine, such as spending more time at home. | ““The same routine for a long time, without a breach in expectations and extra activities” (S16) |
| “Living in front of a computer screen, being confined at home” (S20) | ||
| “The routine became very difficult, especially sleeping, waking up and studying” (S36) | ||
| “Getting used to online classes” (S69). | ||
| 4. Adaptation to new individual and collective protection measures. | Reports that considered adaptation to new individual and collective protection measures, such as hygiene habits and the use of masks, as challenges during the confinement period. | “Getting used to wearing face masks” (S11) |
| “Being very careful with and cleaning supermarket purchases [...]” (S31) | ||
| “The inclusion of new hygiene habits into one’s daily life” (S95) | ||
An analysis of the frequency of student responses was carried out according to the categories in relation to positive, negative points and difficulties during social isolation (Table 3). The results showed that in relation to positive points, students more frequently highlighted leisure and the possibility of personal development (59.3%), followed by social relationships (52.2%). Regarding negative points, mental/social/physical health was the most often cited (72.8%), followed by remote teaching/adaptation to a new routine (51.3%). Among the difficulties faced during isolation, remote teaching and adapting to a new reality continued to stand out (62.7%), followed by mental/social/physical health (38%).
Table 3 Frequency of student responses according to categories in relation to positive, negative points and difficulties during social isolation.
| CATEGORIES | N (%) |
|---|---|
| Positive points | |
| Social relationships | 160 (52.5%) |
| Leisure and personal development | 181 (59.3%) |
| General / social reflections on the current context | 36 (11.8%) |
| Saving of time and money | 28 (9.2%) |
| Negative points | |
| Social/economic/political concerns | 53 (17.5%) |
| Coexistence conflicts | 15 (5%) |
| Mental/social/physical health | 220 (72.8%) |
| Remote teaching / adapting to a new routine | 155 (51.3%) |
| Faced difficulties | |
| Mental/social/physical health | 114 (38%) |
| Coexistence conflicts | 27 (9%) |
| Remote teaching / adapting to a new routine | 188 (62.7%) |
| Adapting to new individual and collective protection measures | 30 (10%) |
Source: study data.
DISCUSSION
This study aimed to evaluate the degree of resilience of medical students during the period of social isolation caused by COVID-19 and its relationship with spirituality and personal factors. Since resilience results from the interaction between risk-promoting factors (adverse situations) and protective factors capable of promoting positive developments in terms of psychosocial well-being11),(21),(30, we also sought to understand the possible risk-promoting factors (negative points and reported difficulties), as well as protective factors (reported positive points), from the students’ perspective.
Our data demonstrate that during the social isolation caused by the COVID-19 pandemic, the most frequently reported negative factors and faced difficulties, and therefore risk promoters, were the changes in mental, social and physical health as well as adapting to a new routine and remote teaching, which can be observed in the sentences:
“Anxiety/lots of bad news and many people going through difficulties/uncertainties about the future/not being able to maintain a routine” (S59)
“Isolation from other people, closing of gyms, unemployment, closing of businesses” (S60)
“Uncertainties and lack of answers about the academic future, loneliness, missing my family, uncertainty as to whether I will be able to return home or whether I should stay in BH. Difficulty exercising and eating is worse. “Feeling useless and without perspective, feeling like crying almost every day” (S48)
“Modifying my routine, not being able to vary where I study, depending on internet access and quality for classes, interruptions during classes by the family” (S86)
Regarding stressors among medical students during the pandemic, our results are consistent with the literature. In a multicenter study carried out in nine countries, addressing changes in lifestyle among medical students (n=2776) during the COVID-19 pandemic, negative changes were observed in all assessed countries, due to changes in the style of classes (they became online), which resulted in an average of 8.7 hours a day in front of a computer screen, with the worsening in study, sleeping and eating habits, leading to symptoms such as back pain, asthenopia, irritability and emotional instability31. Remote teaching and assessments can increase the level of uncertainty and stress, as it is a modality that is still little known in medical education, a fact that may have compromised supervision, communication and monitoring of activities by teachers, in addition to making it difficult to establish socio-affective relationships, which are so relevant to the learning environment32. In addition, the uncertain nature and unpredictable course of the disease, together with intolerance, uncertainty and perceived risk of acquiring the infection were considered risk factors for negative psychological responses, including behavioral changes, emotional distress and avoidance reactions among common people. Previous outbreaks reported that the psychological impact of quarantine can range from immediate effects such as irritability, fear of contracting and spreading the infection to family members, anger, confusion, frustration, loneliness, denial, anxiety, depression, insomnia, despair, and even extreme consequences, such as suicide33.
In this study, carried out during the COVID-19 pandemic, it was observed that medical students presented, on average, moderate resilience and a high degree of spirituality, which showed a significant positive and weak correlation. These do not corroborate what was observed by Salles et al.34 in a study carried out at a University in Rio de Janeiro, in which 54% of students showed low resilience in the pandemic, although they are similar to the findings of another study carried out with medical students, in a period before the pandemic, which found moderate resilience in 53% of students, influenced by religious faith, spirituality, social support and optimism35. A systematic review study demonstrated a moderate positive correlation between resilience and spirituality/religiosity36.
Despite the social isolation promoted by the pandemic, the most cited positive factors were social relationships and the possibility of personal development and leisure. In this context, the students’ resilience and spirituality were positively influenced by their satisfaction in studying to become a doctor; by the level of happiness with life in recent months; for the greater quality of life during isolation; for having a religion and the importance attributed to the fact of having a religion. High spirituality was also influenced by the female gender and age over 25 years. The correlation between the degree of spirituality and resilience observed in this study is relevant, since in addition to the important role of spirituality in resilience, it is also related to improvement in mental health18, quality of life37 and coping with adversity38.
In line with our data, a study carried out by Tempski24 with medical students found that students with high resilience had a better perception of quality of life. The research also showed an association between higher resilience scores and better perception of the educational environment and lower rates of anxiety and depression. Concordant results were also observed by Neufeld39, who demonstrated an association between resilience and psychological well-being, reinforcing that higher resilience scores are related to essential factors to improve well-being and minimize psychological stress.
In the present study, the statements “I feel proud of having accomplished things in my life” and “Maintaining an interest in things is important to me” obtained higher scores and percentage of agreement on the resilience scale, suggesting that personal competence and motivation are important factors for the development of resilience. In the literature, results indicate that satisfaction with competence (“Can I really do this?”) has a positive and statistically relevant association with resilience39. According to Pestana40, students who demonstrate characteristics of resilience perceives themselves as capable of facing the difficulties encountered in the social and academic fields, which reflects positively on academic results, with the school having an important role in promoting resilience, by encouraging students to overcome adversities within the scope of school tasks and other achievements.
Knowing the aspects related to the development of a greater degree of resilience in students is fundamental, since, according to Pestana40, resilience can be developed, and the implementation of specific programs in universities can boost this construct. Studies have demonstrated that among the several factors that comprise the resilient process, spirituality stands out as a mediator capable of providing the individual with resources to overcome adversities18)-(20),(23.
According to Saad, Masiero and Battistella18, the health of individuals is determined by the interaction of physical, mental, social and spiritual factors. Thus, these authors report that there is a possible causal association between spirituality and health. The possible effects of spirituality on health may be related to simple physiological effects, such as the reduction in muscle tension, heart rate and blood pressure, as well as more complex reactions, such as the ability to control pain, suffering, stress, increasing the ability to adapt to challenging situations and expand social ties41.
For the students, spirituality was conceptualized mainly as the “search for the sense and meaning of human life”, followed by “belief in something that transcends the matter”. Half of the students understand spirituality as “belief in and relationship with God/religiosity”, which comes closest to the definition of religiosity42. This suggests a likely overlap between these two dimensions in the student’s perception. Regarding the religious involvement by the students, in the present study, 73.7% declared a religious affiliation. These data differ from the estimate of the Brazilian population, which indicates that 95% have a religion43, but it is close to the results obtained in a multicenter study involving 12 Brazilian medical schools, where religious involvement was found in 66.1% of participating students44. In this study, the relevant role of religion in coping with adversity was observed, since having a religion and giving high importance to having a religion was correlated with higher spirituality and resilience scores. Collier et al.45 reported that religious beliefs and spirituality are part of the individual’s identity and, therefore, are individual components that must be considered when developing strategies to cope with the adversities triggered by the pandemic.
However, it is interesting to note that although the majority reported having a religion, only 32.8% of students associated spirituality to the belief in the existence of the soul and life after death. These data are close to the findings of the study by Lucchetti et al.44, in which this relationship was mentioned by 20.3%. This view of spirituality is close to the broader concept given by Puchalski46, which involves personal aspects that correlate the approach to transcendence through the relationship with others, with the environment, with art and reason.
According to Scorsolini-Comin et al.38, given the scenario of uncertainty and problems experienced during the pandemic, the approach to spirituality can be a strategy that, when providing comfort by offering a dimension of welcoming and addressing reflections, has a humanizing potential, by connecting people, contexts and processes that help develop student resilience.
However, despite the importance of the spirituality dimension in quality of life, resilience and the doctor-patient relationship, few Brazilian medical schools have courses that specifically deal with spirituality/health. A study carried out by Lucchetti et al.47 with 86 medical schools in the country, identified that only 10.4% of the medical teaching institutions offered a specific course on spirituality and 30.1% reported addressing the subject separately at some point during the course, whereas only 2% indicated their intention to implement a specific program on the topic in the curriculum.
The need for new studies on spirituality and resilience among medical students seems to be important to support educational strategies aimed at stimulating student well-being during undergraduate school, reducing their vulnerability to stressful situations, both at the individual level of students and teachers. as well as in teaching conditions.
Considering that the practice of Medicine provides great proximity to life, pain, human suffering, dying and death, in addition to awakening other stressful triggers, the introduction of educational strategies in the curriculum, aiming to approach spirituality and resilience, not only in clinical practice, but also in their personal lives is necessary. To discuss the concepts of spirituality and resilience, and the factors involved, can help promote behavioral changes that will make students stronger in the face of adversity and obstacles, thus training professionals who are better able to deal with the difficulties that will be encountered both in professional practice, as in personal life. However, it is important that these educational strategies be included in the curriculum in a longitudinal way, with approaches in different learning contexts.
This study had as limitations the sample size, which may not have been sufficient to represent the entire population of medical students in Brazil, the realistic context of the responses, since self-answered questionnaires are totally dependent on the interviewees’ sincerity, as well as the cross-sectional characteristic of the study, considering that resilience is a dynamic process of self-reconstruction and adaptation.
FINAL CONSIDERATIONS
During social isolation, the medical students showed moderate resilience and high spirituality, with a positive but weak, correlation between them. The variables that positively influenced resilience and spirituality were satisfaction with studying to become a doctor, high level of happiness with one’s life in recent months and higher quality of life during isolation, having a religion and high importance attributed to the fact of having a religion. High spirituality was also influenced by the female gender and the age group over 25 years old. In this study, it was also possible to identify that during the social isolation caused by the COVID-19 pandemic, the factors that most negatively impacted medical students were mental/social/physical health and adaptation to a new routine and remote teaching. Therefore, the data obtained in this study suggest that students who had greater spirituality were probably more resilient and able to deal with the stressors related to physical/mental/social health and the remote teaching routine imposed by social isolation, in addition to adapting and maintaining a positive attitude regarding the experienced problems. These results can support the reflection of educational strategies aimed at helping to face problems arising as a result of social isolation, in addition to other adversities commonly found in the medical course.
REFERENCES
1. Ribeiro CO. Alteridade, espiritualidade e pandemia. CDR. 2020;8(13):231-48. [ Links ]
2. Raony I, Figueiredo CS, Pandolfo P, Giestal-de-Araujo E, Oliveira-Silva BP, Savino W. Psycho-neuroendocrine-immune interactions in Covid-19: potential impacts on mental health. Front Immunol. 2020;27(11): 1170. [ Links ]
3. United Nations Educational, Scientific and Cultural Organisation. Covid19: educational disruption and response. Paris: Unesco, 30 July 2020 [acesso em 22 maio 2020]. Disponível em: Disponível em: http://www.iiep.unesco.org/en/covid-19-educational-disruption-and-response-13363 . [ Links ]
4. Brasil. Portaria nº 343, de 17 de março de 2020. Dispõe sobre a substituição de aulas presenciais por aulas em meios digitais enquanto durar a situação de pandemia do Novo Coronavírus - COVID-19. Diário Oficial da União, 18 mar 2020. Seção 1, p. 39 [acesso em 6 maio 2020]. Disponível em: Disponível em: http://www.in.gov.br/en/web/dou/-/portaria-n-343-de-17-de-marco-de-2020-248564376 . [ Links ]
5. Gundim VA, Encarnação JP da, Santos FC, Santos JE, Vasconcellos EA, Souza RC. Saúde mental de estudantes universitários durante a pandemia de Covid-19. Rev Baiana Enferm. 2020;35:1-14 [ Links ]
6. Oliveira FN, Bianchini LGB, Reis LA dos. Significações do professor e indicadores de resiliência em estudantes com dificuldades de aprendizagem em matemática. ETD. 2019;21(2):416-34. [ Links ]
7. Rocca L, Susana M. Resiliência: um novo paradigma que desafia a reflexão e a prática pastoral. Atual Teol. 2208;ano XII(28):248-264. [ Links ]
8. Grotberg EH. Nuevas tendencias en resiliencia. In: Melillo A, Ojeda ENS, organizadores. Resiliencia: descobriendo las propias fortalezas. Buenos Aires: Paidós; 2002. p. 19-30. [ Links ]
9. Angst R. Psicologia e resiliência: uma revisão de literatura. Psicol Argum. 2009;27(58):253-60. [ Links ]
10. Rogge JFN, Lourenço ML. A resiliência humana no ambiente acadêmico de cursos stricto sensu. Rev Adm IMED. 2015;5(3):291-301. [ Links ]
11. Tomás C, Instituto Superior Manuel Teixeira Gomes. Resiliência e espiritualidade. Quando a fé se torna amparo. OMNIA Rev Interdiscip Ciênc Artes. 2018;8(2):29-36. [ Links ]
12. Chequini MCM. A relevância da espiritualidade no processo de resiliência. Psicol Rev. 2007;16(1/2):93-117. [ Links ]
13. Khosravi M, Nikmanesh Z. Relationship of spiritual intelligence with resilience and perceived stress. Iran J Psychiatry Behav Sci. 2014;8(4):52-6. [ Links ]
14. Sant’ana G, Silva CD, Vasconcelos MBA. Espiritualidade e a pandemia da Covid-19: um estudo bibliográfico. CCS. 2020;31(03):71-7. [ Links ]
15. Cunha VF da, Rossato L, Scorsolini-Comin F. Religião, religiosidade, espiritualidade, ancestralidade: tensões e potencialidades no campo da saúde. Rev Relegens Thréskeia. 2021;10(1):143-70. [ Links ]
16. Koenig HG, King DE, Carson VB. Handbook of religion and health. Oxford: Oxford University Press; 2012. [ Links ]
17. Puchalski C, Ferrell B, Virani R, Otis-Green S, Baird P, Bull J, et al. Improving the quality of spiritual care as a dimension of palliative care: the report of the Consensus Conference. J Palliat Med. 2009 Oct;12(10):885-904. [ Links ]
18. Saad M, Masiero D, Battistella LR. Espiritualidade baseada em evidências. Acta Fisiátrica. 2001;8(3):107-12. [ Links ]
19. Garfield CF, Isacco A, Sahker E. Religion and spirituality as important components of men’s health and wellness. Am J Lifestyle Med. 2013 Jan;7(1):27-37. [ Links ]
20. Gnanaprakash C. Spirituality and resilience among post-graduate university students. J Health Manag. 2013 Sept 1º;15(3):383-96. [ Links ]
21. Werner E, Smith RS. Vulnerable but invincible: a longitudinal study of resilient children and youth. New York: McGraw-Hill; 1982. [ Links ]
22. Wachholtz A, Rogoff M. The relationship between spirituality and burnout among medical students. J Contemp Med Educ. 2013;1(2):83-91. [ Links ]
23. Lucchetti G, Lucchetti AG, Badan-Neto AM, Peres PT, Peres MFP, Moreira-Almeida A, et al. Religiousness affects mental health, pain and quality of life in older people in an outpatient rehabilitation setting. J Rehabil Med. 2011 Mar;43(4):316-22. [ Links ]
24. Tempski P, Santos IS, Mayer FB, Enns SC, Perotta B, Paro HBMS, et al. Relationship among Medical student resilience, educational environment and quality of life. PLoS One. 2015 June 29;10(6):e0131535. [ Links ]
25. Vinuto J. A amostragem em bola de neve na pesquisa qualitativa. Temat. 2014;22(44):203-20. [ Links ]
26. Wagnild GM, Young HM. Development and psychometric evaluation of the Resilience Scale. J Nurs Meas. 1993;1(2):165-78. [ Links ]
27. Pesce RP, Assis SG, Avanci JQ, Santos NC, Malaquias JV, Carvalhaes R. Adaptação transcultural, confiabilidade e validade da escala de resiliência. Cad Saude Publica. 2005;21(2):436-48. [ Links ]
28. Braghetta CC. Desenvolvimento e validação de um instrumento para avaliar espiritualidade: Escala de Atitudes Relacionadas à Espiritualidade (ARES). São Paulo: Universidade de São Paulo; 2017 [acesso em 26 set 2022]. Disponível em: Disponível em: https://www.teses.usp.br/teses/disponiveis/5/5142/tde-05102017-112819/?gathStatIcon=true . [ Links ]
29. Bardin L. Análise de conteúdo: edição revista e ampliada. São Paulo: Edições; 2016. [ Links ]
30. Sisto A, Vicinanza F, Campanozzi LL, Ricci G, Tartaglini D, Tambone V. Towards a transversal definition of psychological resilience: a literature review. Medicina. 2019;55(11):745. [ Links ]
31. Perez-Dominguez F, Polanco-Ilabaca F, Pinto-Toledo F, Michaeli D, Achiardi J, Santana V, et al. Lifestyle changes among medical students during Covid-19 pandemic: a multicenter study across nine countries. Health Educ Behav. 2021 Aug;48(4):446-54. [ Links ]
32. Cao W, Fang Z, Hou G, Han M, Xu X, Dong J, et al. The psychological impact of the Covid-19 epidemic on college students in China. Psychiatry Res. 2020; May;287:112934. [ Links ]
33. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. O impacto psicológico da quarentena e como reduzi-lo: revisão rápida das evidências. Lancet. 2020;395(10227):912-20. [ Links ]
34. Salles GEB de, Gandra DM, Nogueira HP, Silva LCP, Cruz MC, Corrêa MG, et al. Mudanças comportamentais e resiliência dos estudantes de Medicina em meio à pandemia da Covid-19. Braz J Hea Rev. 2021 Apr;15;4(2):8451-63. [ Links ]
35. Martinez JE, Assis Pereira D de, Santos Barril E dos, Matos SF de, Santos RM dos. Resiliência em estudantes de medicina ao longo do curso de graduação. Rev Fac Cienc Med Sorocaba. 2016;18(1):15-8. [ Links ]
36. Schwalm FD, Zandavalli RB, Castro Filho ED de, Lucchetti G. Is there a relationship between spirituality/religiosity and resilience? A systematic review and meta-analysis of observational studies. J Health Psychol. 2022 Apr;27(5):1218-32. [ Links ]
37. Freitas Melo C de, Sampaio IS, Abreu Souza DL de, Santos Pinto N dos. Correlação entre religiosidade, espiritualidade e qualidade de vida: uma revisão de literatura. Estud Pesq Psicol. 2015;15(2):447-64. [ Links ]
38. Scorsolini-Comin F, Rossato L, Cunha VF da, Correia-Zanini MRG, Pillon SC. A religiosidade/espiritualidade como recurso no enfrentamento da Covid-19. Rev Enferm Cent-Oeste Min. 2020;10(1):1-12 [acesso em 26 set 2022]. Disponível em: Disponível em: http://www.seer.ufsj.edu.br/index.php/recom/article/view/3723 . [ Links ]
39. Neufeld A, Malin G. Exploring the relationship between medical student basic psychological need satisfaction, resilience, and well-being: a quantitative study. BMC Med Educ. 2019 Nov 5;19(1):1-8. [ Links ]
40. Pestana DF de J. Resiliência em contexto ou contexto da resiliência: resolução de problemas em estudantes universitários [tese]. Lisboa: Universidade de Lisboa; 2018 [acesso em 26 set 2022]. Disponível em: Disponível em: https://repositorio.ul.pt/handle/10451/37625 . [ Links ]
41. Dantas Filho VP, Sá FC de. Ensino médico e espiritualidade. Mundo Saúde. 2007;31(2):273-80. [ Links ]
42. Koenig HG. Religion, spirituality, and health: the research and clinical implications. ISRN Psychiatry. 2012 Dec;16(2012):373-381. [ Links ]
43. Moreira-Almeida A, Lucchetti G. Panorama das pesquisas em ciência, saúde e espiritualidade. Cien Cult. 2016;68(1):54-7. [ Links ]
44. Lucchetti G, Bassi RM, Lucchetti ALG. Taking spiritual history in clinical practice: a systematic review of instruments. Explore. 2013 May;9(3):159-70. [ Links ]
45. Collier KM, James CA, Saint S, Howell J. The role of spirituality and religion in physician and trainee wellness. J Gen Intern Med. 2021 Oct;36(10):3199-201. [ Links ]
46. Puchalski C. Task force report: spirituality, cultural issues, and end of life care. Assoc of Am Med Colleg, Contemporary issues in medicine, communication in medicine, medical school objectives Project. 1999:25-6. [ Links ]
47. Lucchetti G, Lucchetti ALG, Espinha DCM, Oliveira LR de, Leite JR, Koenig HG. Spirituality and health in the curricula of medical schools in Brazil. BMC Med Educ . 2012;12(1):1-8. [ Links ]
Received: November 16, 2022; Accepted: September 11, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
