











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por email
 Permalink
Permalink
INTRODUCTION
The teaching of pediatrics in Brazilian medical schools started in the middle of the 19th century, as part of the content of obstetrics1. Since the 20th century, pediatrics gained its own space as “Children’s Internal Medicine and Surgical Care”, and has progressively consolidated itself as an area of knowledge essential to the training of general practitioners1),(2.
Between 1999 and 2000, the Pan American Health Organization (Paho), in partnership with the Latin American Pediatric Association (Alape), analyzed the teaching of pediatrics, using a questionnaire sent to medical schools from the database of the Pan American Federation of Medical Colleges and Schools (Fepafem)3. One hundred and ninety-four medical schools from 19 countries in Latin America joined the survey (approximately 50% of the total). The median course load (CL) on pediatrics in the curriculum was 20 weeks (with 1 week being equivalent to 20 hours) among the schools that provided this information in a detailed and consistent manner, and the duration of teaching ranged from 5 to 40 weeks; however, responses below or above this range were excluded. Most of the practical teaching of pediatrics occurred during the clerkship and predominantly at the hospital. Based on these and other findings, several recommendations were made by the authors for the teaching of pediatrics. One of them was the increase in practices outside the hospital and in the hours of practice, which should be started in primary health care in the first years of the course, to that students would have contact with the community and learn the health care process in an integrated way, with activities aimed at health promotion and the prevention of diseases3.
The National Curriculum Guidelines for Undergraduate Medical Courses (DCN)4 establish that the course has a minimum CL of 7,200 hours but does not specify CL range for each area of knowledge. Only the the clerkship CL is specified, which must represent 35% of medical course CL (at least 2,520 hours) and last for two years, with 30% of its activities in the area of General Family Health and Community Medicine in Primary Care and emergency services of the Unified Health System and 70% in the areas of Internal Medicine and Surgical Care, Gynecology and Obstetrics, Pediatrics, Public Health and Mental Health.
The undergraduate curriculum CL in pediatrics is only specified in the premises and guidelines for the teaching of pediatrics at the Brazilian Society of Pediatrics (SBP)5, launched in 2017, based on several documents, including the study by Paho-Alape3, the matrix of curricular correspondence for the purpose of revalidating medical diplomas obtained abroad, competency matrices6 and the clerkship competencies defined by the Brazilian Association of Medical Education7. The SBP recommends that the pediatrics CL correspond to 10% of the total medical course load and that its teaching begin in the first years of the medical course, preferably longitudinally and with increasing complexity5.
The following research question was then raised:
As the authors found no scientific evidence to answer this question, this study was carried out to fill this gap, with the aim of analyzing the total and the pediatric course loads of the Brazilian medical schools’ curricula.
METHOD
This study had a cross-sectional and descriptive design. As the studied data are public and available on the internet, it was not necessary to submit the research project to the Ethics Committee.
We analyzed the existing Medical Schools in Brazil in October 2017, totaling 294 according to data from the Ministry of Education (MEC)8.
The criteria for inclusion of schools were: having a curriculum matrix/grid or political-pedagogical project (PPP) available online and containing sufficient and accurate data regarding the number of hours of pediatrics teaching per year of course.
Data collection was carried out by searching the official internet page of each medical school at the website “Medical Schools”9. The curriculum matrices/grids or PPP of each medical school, in their most recent versions, were accessed, and the variables studied were the geographic region and the school administrative category, type of curriculum, total CL of the medical course, total CL of clerkship, CL of pediatrics (per year), CL of pediatrics at the clerkship and pediatrics’ theoretical and practical CL per year.
The data were entered into a database using Microsoft Excel 2013 software. As the course loads were presented in a heterogeneous way (hours/class and clock hours or actual hours), the course load presented as hours/class were proportionally converted to effective hours (actual hours or “clock hours”). Before the conversion, some schools showed 1 hour/class corresponding to 60, 50 or 45 actual minutes.
Data analysis was performed using descriptive statistics, calculating absolute and relative frequencies for categorical variables and measures of central tendency for continuous variables. The normality of continuous variables was assessed by the Kolmogorov-Smirnov test (K-S), with the distribution was considered normal when p >.05. Continuous variables with normal distribution should be analyzed with mean and standard deviation (SD) and those with non-normal distribution with median and the 25th and 75th percentiles (P25-75). However, both measures are shown in the results, to allow comparison with data from the literature.
RESULTS
Characteristics of schools
One hundred and fifty-one schools were included in the study (51.4% of the total). Of the 143 which were not included, 43 did not provide their curriculum matrix/ grid or online PPP (n = 43), 29 provided the PPP without information about the programs or CL and 71 provided their PPP without differentiating the specific load aimed at the teaching of pediatrics.
The administrative category was private in 82 schools (54.3%), federal in 49 (32.5%), state in 16 (10.6%) and municipal in 4 (2.6%).
The curriculum was traditional in 132 schools (87.4%), unspecified in 9 (6%), modular in 5 (3.3%) and had problem-based learning in 5 (3.3%).
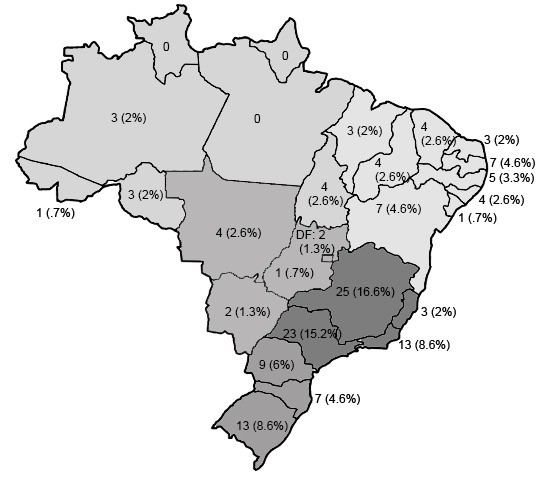
The geographic region of 29 schools was the South (60.4% of the total medical schools in this region), 64 schools in the Southeast (52% of the total schools in this region), 38 in the Northeast (52.8% of the total schools in this region), 11 in the North region (44% of the total schools in this region) and 9 in the Midwest (34.6% of the total schools in this region).
The distribution of 151 Brazilian medical schools by state is shown in Figure 1.
Course load and course load in pediatrics in medical schools.
The schools’ total and the pediatrics course load is shown in Table 1.
Table 1 Total and pediatrics course load in 151 of the 294 existing Brazilian medical schools in October 2017.
| Course load | Mean (DP) | Median (P25-75) | Minimum | Maximum | p* |
|---|---|---|---|---|---|
| Total CL | 8,053.8 (656.9) | 7,975 (7440-8550) | 7,200 | 9,885 | .01 |
| Total CL before the clerkship | 4,665.7 (593.8) | 4,640 (4,260-5,045) | 3,225 | 6,262 | .2 |
| ClerkshipCL | 3,388.1 (430.3) | 3,430 (3,072-3,710) | 2,520 | 4,425 | .2 |
| Total pediatrics CL | 778.2 (181.6) | 780 (630-900) | 396 | 1,300 | .2 |
| Pediatrics CL before the clerkship | 238.9 (108.5) | 220 (160-300) | 46 | 740 | <.01 |
| Pediatrics practical CL before clerkship† | 139.8 (71.5) | 123 (90-180) | 27 | 345 | .003 |
| CL of pediatrics clerkship | 538.6 (161.6) | 514 (405-640) | 180 | 1075 | <.01 |
Abbreviations: SD: Standard Deviation; P25-75: 25th and 75th percentiles. * P-value in the Kolmogorov-Smirnov test (normality if p >.05). †A total of 72 schools differentiated the theoretical from the practical CL in pediatrics, of which 2 did not offer practical CL before the clerkship.
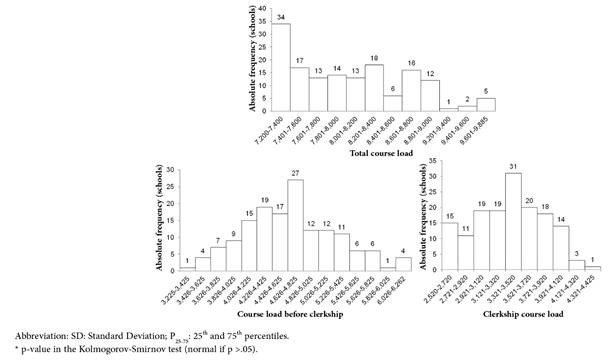
Figure 2 illustrates the distribution of schools by CL of the medical course.
Fifty-two schools had a pediatrics CL of less than 700 hours (27.3%). Of these, 9 have a CL between 396 and 500 hours and 43 CL between 501 and 699. Eight schools had a CL between 700 and 720 hours (4.2%) and 29 between 721 and 800 hours (15.3%). The remainder had a CL for over 800 hours. Figure 3 illustrates the distribution of schools by total CL of pediatrics.
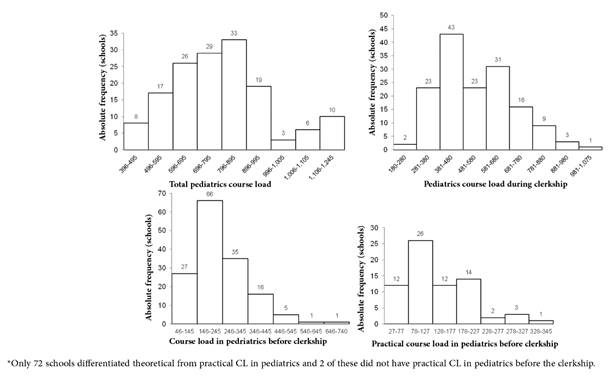
Figure 3 Course load in pediatrics in 151 of the 294 existing Brazilian medical schools in October 2017*
Two schools started teaching pediatrics in the first year of the course (1.3%), 19 in the second (12.6%) year, 63 in the third (41.7%) and 67 in the fourth year (44.4%).
The theoretical CL of the 2 schools that started teaching in the first year was 40 and 55 hours.
Of the 72 schools that had differentiated data between the theoretical and practical CL of pediatrics, 2 had no practical pediatrics CL before the clerkship. The practical CL in pediatrics started in the 2nd year in 6 schools, in the 3rd year in 28 and in the 4th year in 36. Regarding the distribution in the curriculum, 2 had a practical CL only in the 2nd year, 3 had practical CL from the 2nd to the 4th year, 6 only in the 3rd year, 22 from the 3rd to the 4th years, 36 only in the 4th year, and 1 in the 2nd and 4th years. Therefore, 6 schools had practical CL in the 2nd year, 31 in the 3rd and 61 in the 4th year.
The medians of theoretical and practical CL were, respectively: in the 2nd year, 114 (P25-75 = 48.7-160) and 87.8 (P25-75 = 18.7-135.5); in the 3rd year, 100 (P25-75 = 60-152) and 60 (P25-75 = 45-120); and, in the 4th year, 120 (P25-75 = 67-165) and 102 (P25-75 = 74-134).
The mean of the proportion between the total CL and the CL in pediatrics was 9.7% (SD = 2.2), ranging from 5% to 15%, and the median was 9.5%, P25-75 = 8.1-11.4 (p = .04 in the K-S test). The mean proportion between the clerkship CL in pediatrics and the total CL was 15.9% (SD = 4.2), ranging from 6% to 26%, and the median, 16%, P25-75 = 12.5-18.9 (p = .02 in the K-S test). The mean proportion between the CL before the clerkship in pediatrics and the CL was 5.1% (SD = 2.2), ranging from 1% to 13%,and the median was 4.7%, P25-75 = 3.6-6.5 (p = .01 in the K-S test).
DISCUSSION
In this study, the median CL of the curriculum of the studied schools was 7,975 hours; however, due to its wide variation, the 25th and 75th percentiles were 7,440 and 8,550, respectively.
Although all schools comply with the norm established by the National Curriculum Guidelines (DNC) of a CL equal to a minimum of 7,200 hours4, the majority greatly exceeds this value. Only three showed the minimum CL, at least half had a CL over 7,975 hours (10% over the minimum stipulated by the DCN), and at least seven exceeded 2,224 hours of this recommendation (30.9%), reaching a maximum limit of 9,885 hours.
It is clear that, as there is no maximum limit for the CL, the definition of this load is at the discretion of each institution, which creates the risk of CL that go far beyond the minimum recommendation by DCN. This “extra” period of 2,224 hours observed in some medical schools represents 60.1% to 74% of the minimum time required for training in some undergraduate courses in other areas, such as law, computer science and public administration10. And, even in relation to other courses in the health field, the minimum CL for medical courses is quite high10.
The median CL of clerkship in the 151 schools was 3,430 (P25-75 = 3,072-3,710), ranging from 2,520 to 4,425 hours. All of them also comply with the minimum CL stipulated by the DCN of 2,520 hours for the clerkship, and the majority goes well beyond this limit. As the duration of the clerkship is two years, the increase in CL results into a direct increase in the weekly CL, with a consequent decrease in free areas and days of vacation for students.
For more than 20 years, the need to reduce the excessive theoretical content of the medical curriculum has been recommended, and there have been recommendations to create a core curriculum with mandatory subjects that are essential for medical training and approximately 30% of subjects that the students can choose, according to their preferences and affinities. Moreover, it is recommended to guarantee the existence of green areas, also called pro-student, from the first to the fourth year of the course, which represents free time for the student11),(12.
Although the curriculum design and the course load definition represent delicate situations between the areas of knowledge7, it is essential that a proposal for a curriculum without excesses is attained.
The information overload, caused by the volume of biomedical and clinical knowledge and the speed in its production, dissemination and renewal, exceeds the capacity of the human mind to organize and retain it. Increasingly, attention has been drawn to the need to focus teaching on capturing and managing knowledge13.
A study by Monteiro et al., carried out in Northern Brazil, demonstrated that students sleep little and consider that fatigue, the amount of content, additional work and the short time available interfere in their study process14.
As DiCarlo states15, many higher education courses have excessive content, inadequate time to think and very little fun. The author affirms that the excess of factual content taught during traditional classes, in which the student takes on a passive posture, makes learning boring. Memorizing this content is only good for the students to take tests, and it is easily forgotten. This process does not encourage students to think more profoundly to provide its understanding and leaves them little time to develop skills to learn throughout life, such as thinking critically, solving problems, communicating and connecting. In their words, “students need to talk” and write about what they learn, “to correlate the new information with their previous experiences and apply it in their daily lives”. For that purpose, they need time to build and consolidate knowledge. The author emphasizes that teachers need to forsake the idea that it is necessary to cover the content so that students are well prepared for the future. He then proposes to reduce the factual content of the curriculum and classes in which the students passively receive information. Instead, he recommends using resources that can inspire and motivate the students’ interest and love of learning and make them active and progressively independent in the construction of their knowledge15.
Even alterations in the traditional curriculum, with a reduction in content and student inclusion since the beginning of the course in primary care settings, together with experience in the community, are associated with increased motivation for learning among the students of the first two years of the course16.
The overload of content has also been pointed out as being among the several factors responsible for the onset of depressive symptoms17, of which prevalence was estimated at 27.7% among medical students in a meta-analysis carried out in 2016 including studies from 43 countries18.
As for the teaching of pediatrics, 68.5% of the schools have a CL in pediatrics of over 720 hours. The proportion between the total CL in pediatrics and the total CL was less than 8% in 58 of the schools and its median was 9.5% (P25-75 = 8.1-11.4).
This is similar to the mean proportion of 10.1% found by Del Ciampo and Del Ciampo in a study with Brazilian medical schools until 200219, and of 9.7% (SD = 2.7) found by Veiga and Batista in medical schools located in Rio de Janeiro20.
The inclusion of pediatrics in the curriculum tends to be a later one, with 44.4% schools starting their teaching in the fourth year and 41.7% in the third year. Few schools offer the teaching of pediatrics throughout the course and only 3 offer theoretical teaching combined with the practical teaching from the second to the fourth year.
The practical classes follow the same trend, starting before the third year in only 8.6% of schools and few schools offering it longitudinally during the four years before clerkship.
These findings are in line with the recommendations of Paho-Alape3 and SBP5, which recommend that training in pediatrics be started early in the course, with increasing complexity, and that practical training should be started in the first years of the medical course, ideally in primary care3. Other documents 21), (22 emphasize the undeniable importance of practical activities for medical training.
Therefore, our study demonstrates that it is still necessary to include teaching in pediatrics in earlier stages of the medical course, associating theory with practice, and in a longitudinal way.
Finally, as a reflection on the curriculum, if medical education aims to train professionals capable of caring for people, it is important that managers and everyone involved in medical training consider that an excess content is harmful to students’ learning and health, considering that students often enter medical school in their teens. As a basis for building their future professional identity, it is essential that the students have time and incentive for reflection. Moreover, it is necessary to share resources and encourage them to take care of themselves, to cultivate resilience and develop constructive and caring relationships with everyone involved in their education, including peers, teachers, managers, patients and the community23.
This study had some limitations. One of them was the impossibility of including all schools, due to the online unavailability of their pedagogical projects or curricular matrices/grids on the official websites of the educational institutions or lack of data in these documents about the CL in pediatrics. Also, this study analyzed only the CL of the medical and pediatrics course, without considering the content and methodology of teaching and assessment, not allowing the analysis of the teaching quality. However, the analysis of the CL allows the evaluation of the course content load and the time allocated and importance given by the institution to the teaching of pediatrics, aiming at developing skills to work in pediatric health care.

