











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por email
 Permalink
Permalink
INTRODUCTION
Nonverbal communication is an important part of medical interviewing1, corresponding to nearly 60% of doctor-patient interactions2)-(5. Nonverbal communication has been widely researched outside the medical field6), (7. In the medical literature, studies have suggested that nonverbal communication plays an important role in the physician-patient relationship8, being associated with patient satisfaction9)-(11, emotional distress12, symptom resolution13, and malpractice claims14.
Despite such evidence, nonverbal skills are still underestimated in medical education. Few interventions designed to improve medical students’ nonverbal behavior are reported in the medical education research field. Uncertainties on whether nonverbal behavior may be developed through educational interventions might explain this paucity of evidence10),(15)-(17. Some authors believe nonverbal behavior is innate18, while others admit that this behavior is culture-specific and can be learned19. We assume that nonverbal communication skills are determined by a fusion of these extremes5.
Considering nonverbal communication - posture, gesture, eye contact, tone of voice, and proximity, that is, aspects of an actor’s demeanor that frame the message content - as a trainable skill8),(20),(21, the existence of appropriate instruments for teaching and assessing the nonverbal behavior of physicians and medical students is mandatory. The Relational Communication Scale for Observational measurement of doctor-patient interactions (RCS-O) is an instrument specifically developed to measure the relational communication aspects of the doctor-patient interaction. It is practical to administer and can be used in formative assessments of medical students and physicians22. Since the RCS-O has been originally developed in the United States, its use in other countries must be preceded by the adequate processes of translation, cultural and linguistic adaptation23. Such processes are particularly important as nonverbal skills vary between different situations and cultures24)-(26.
The RCS-O is used for the direct observation of the doctor-patient relationship, with good psychometric properties for the majority of its items and domains. To the best of our knowledge, the RCS-O is the only validated instrument that was specifically developed to measure the relational aspects of non-verbal behavior during the interaction between doctor and patient (22.
This research reinforces the importance of nonverbal communication as a powerful medical skill and aims to translate and culturally adapt the RCS-O to Brazilian Portuguese. The scale will be used to assist medical educators in designing and evaluating educational interventions tailored to improve students’ nonverbal communication with patients.
METHODS
This is a cross-cultural adaptation study, which was approved by the local research ethics committee, carried out after permission by Judee Burgoon, the instrument’s author.
Instrument
The RCS-O is a validated version for third-party observers of doctor-patient interactions of the Burgoon and Hales’ relational communication scale (RCS)22),(27)-(30. The scale was specifically developed to produce a global measure of the relational component of doctor-patient interactions, handled primarily through nonverbal channels22. It comprises 34 items arranged in six dimensions.
The six dimensions are divided as follows: (1) intimacy - IA immediacy/affection - the degree to which closeness or distance is expressed, (2) intimacy (SD - similarity/depth) - the degree to which the interactants feel alike or different, (3) intimacy (RT - receptivity/trust) - the degree to which interest and concern or lack of interest and disregard are expressed, (4) composure (C) - the degree to which one is calm or anxious, (5) formality (F) - the degree to which the interaction is formal or relaxed and (6) dominance (D) - the degree to which power is shared or unequal22.
The instrument can be used in formative assessment of physicians and medical students22. Answers are rated on a seven-point Likert scale ranging from ‘’strongly disagree’’ to ‘’strongly agree’’. Scores range from 34 to 228, with higher scores indicating the ability to put the patient at ease and develop an equal partnership with the patient. Doctors with higher scores demonstrate openness by revealing a professional demeanor that is friendly, approachable, and relaxed. The RCS-O is a psychometrically sound instrument used to measure relational communication skills not only in patient-centered, but also in doctor-centered approaches22),(27),(28),(30.
Translation and cultural adaptation
The translation and cultural adaptation of the instrument were performed according to international guidelines31),(32 (Figure 1). In the first stage - forward translation - two bilingual translators native of Brazilian Portuguese produced two independent translations of the instrument from English into Brazilian Portuguese. In the second stage, a bilingual healthcare professional native of Brazilian Portuguese performed the reconciliation of the previous translations. In the third stage (back translation), an American translator fluent in Portuguese translated the reconciled version back into the original language. In the fourth stage, the author of the instrument made comments on the back-translated version.
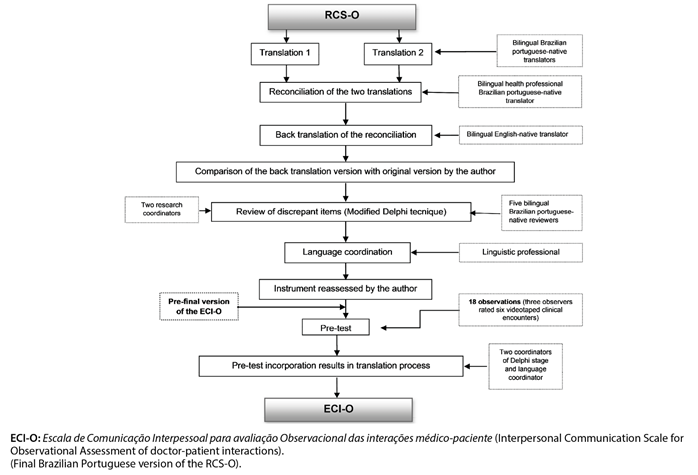
In the fifth stage, items, behavior categories, expressions, sentences or words identified as lacking semantic, idiomatic, experimental or conceptual equivalences at any stage of the translation process were sent to be reviewed. Five bilingual reviewers native of Brazilian Portuguese (two professional translators and three physicians experienced in the process of translation of outcome measures) assessed all previous stages to choose the best translation option for the instrument. The modified Delphi technique33),(34, was used to reach a consensus among reviewers in interactive electronic rounds organized by two research coordinators in semi-structured questionnaires on the Delphi Decision Aid website35.
After each round, independent reviewers received feedback on the statistical analysis of responses. They also received suggestions made by other reviewers in each round. The questionnaires answered by the independent reviewers comprised the entire translation process and were available to the reviewers during the whole process, which totaled three rounds. The process was completed after meeting at least 80% of consensus among the participants36),(37. The instrument was then sent for evaluation by a language coordinator and for a new analysis by the author (stage six), to produce the pre-final version.
Pre-test
Three interns, three medical residents, and six patients provided informed consent for the recording of their clinical outpatient encounters held at the university hospital of our institution.
Three observers from the faculty of our institution used the pre-final Brazilian version of RCS-O (stage seven) to assess four videotaped clinical encounters between real patients and medical students and residents. This video approach is useful and reliable for analyzing physician-patient nonverbal communication interactions in medical settings38.
The observers obtained instructions during a two-hour meeting, when observers and research coordinators discussed about the scale nature, conception, and use. A relational communication analysis was also part of the topics covered during the meeting. Each observer received a flash drive with the pre-final version of the scale, instructions for rating the instrument, a manual, and a video lesson containing information about the scale and about nonverbal communication skills.
The observers underwent a retrospective and cognitive interview in order to check understanding and applicability of the items and domains37. Research and language coordinators analyzed suggestions given by the observers and incorporated them, when relevant, into the final Brazilian version of the RCS-O (supplementary material). The final items were named after the domain and number in the original scale (e.g., Item 3 - domain Intimacy I - immediacy/affection = IA3). The items were randomly arranged before instrument administration.
The number of videotaped clinical encounters (4) and observers (3) (totaling twelve observations) was enough to conclude the cultural adaptation of the instrument, although it was insufficient to perform any statistical analysis for validation purposes. Sample sizes of five to 12 participants in the pre-test phase have been used in several cultural adaptation studies39)-(43.
RESULTS
The RCS-O title and items “The physician did not want a deeper relationship with the patient” (IA2), “The physician communicated coldness rather than warmth” (IA5), and “The physician seemed to desire further communication with the patient” (SP13) were reviewed after the back translation and the author’s comments. These items were then analyzed through the modified Delphi technique rounds. The item IA5 reached consensus (100% agreement) only after four rounds (Table 1).
Table 1 Process to solve discrepant item translations using the modified Delphi technique.
| Original Item | Translations | Number of rounds to reach consensus | Percentage of consensus | |
|---|---|---|---|---|
| Title Relational communication scale for observational measurement of doctor-patient interactions (RCS-O) | T1 | Escala de comunicação relacional para a medição de observação das interações médico-paciente (RCS-O) | 2 | 80% |
| T2 | Escala de comunicação relacional para a medição de observação das interações médico-paciente (RCS-O) | |||
| REC | Escala de comunicação relacional para medida observacional das interações médico-paciente (ECR-O) | |||
| RT | Communicational relations scale for measuring observations of the interaction between physician and patient (CRS-O) | |||
| Pre-final | Escala de comunicação interpessoal para medida observacional das interações médico-paciente (ECI-O) | |||
| IA2 item The physician did not want a deeper relationship with the patient b | T1 | O médico não quis uma relação mais profunda com o paciente b | 2 | 80% |
| T2 | O médico não quis uma relação mais aprofundada com o paciente b | |||
| REC | O médico não quis uma relação mais aprofundada com o paciente b | |||
| RT | The physician did not want a more intimate relation with the patient b | |||
| Pre-final | O(a) médico(a) não quis uma relação mais próxima com o(a) paciente b | |||
| IA5 item The physician communicated coldness rather than warmth b | T1 | O médico comunicou-se de forma fria ao invés de cordial b | 4 | 100% |
| T2 | O médico comunicou-se com frieza ao invés de cordialidade b | |||
| REC | O médico comunicou-se friamente ao invés de calorosamente b | |||
| RT | The physician communicated in a cold way, rather than warmly b | |||
| Pre-final | O(A) médico(a) transmitiu frieza ao invés de cordialidade b | |||
| SP13 item The physician seemed to desire further communication with the patient | T1 | O médico pareceu desejar mais comunicação com o paciente | 2 | 80% |
| T2 | O médico pareceu desejar uma maior comunicação com o paciente | |||
| REC | O médico pareceu desejar manter a comunicação com o paciente | |||
| RT | The physician seemed to want to maintain communication with the patient | |||
| Pre-final | O(A) médico(a) pareceu desejar continuar a comunicação com o paciente | |||
T1 - Forward Translation 1; T2 - Forward Translation 2; REC - Reconciliation; RT - Back translation; b - items must be reverse-coded before analyzing the data.
At the end of the translation process, the language coordinator adjusted nine (26.4%) items. The adjustments were grouped into five categories: Conventionality pragmatic level, conventionality syntactic level, ambiguity/polysemy, literal translation and comprehension (Table 2). Items that required modification generally belonged to the intimacy domains I and II. Items IA2, IA5, and SP13 required more than one change. In the item IA2, both changes were in the combinality category. Five items were adjusted due to ambiguity/polysemy (Table 2).
Table 2 Main adjustments due to inconsistencies in the translation process of the Brazilian RCS-O items.
| Adjustment category | Items | Examples | |
| Reconciliation | Final version | ||
| *Conventionality Pragmatic level | Title, C21, C23 | Title - Escala de Comunicação Relacional para medida Observacional das interações médico-paciente (ECR-O) C21 - O médico sentiu-se muito tenso ao conversar com o paciente b C23 - O médico sentiu-se muito relaxado ao conversar com o paciente | Title - Escala de Comunicação Interpessoal para avaliação Observacional das interações médico-paciente (ECI-O) C21 - O(A) médico(a) pareceu muito tenso(a) ao conversar com o(a) paciente ᵇ C23 - O(A) médico(a) pareceu muito tranquilo(a) ao conversar com o(a) paciente |
| * Conventionality Syntactic level (Combinality) | IA2, IA5, IA6, D34 | IA2 - O médico não quis uma relação mais aprofundada com o paciente b D34 - O médico dominou a conversação | IA2 - O(A) médico(a) não quis estabelecer uma relação mais próxima com o(a) paciente b D34 - O(A) médico(a) teve controle sob a conversa |
| *Ambiguity/polysemy | IA2, IA4, IA5, SP13, C23 | IA4 - O médico achou a conversa estimulante IA5 - O médico comunicou-se friamente ao invés de calorosamente b SP13 - O médico pareceu desejar manter a comunicação com o paciente C23 - O médico sentiu-se muito relaxado ao conversar com o paciente | IA4 - O(A) médico(a) achou a conversa empolgante IA5 - O(A) médico(a) transmitiu frieza ao invés de cordialidade b SP13 - O(A) médico(a) pareceu querer continuar a conversa com o(a) paciente C23 - O médico pareceu muito tranquilo (a) ao conversar com o paciente |
| *Literal translation | SP11 | SP11 - O médico tentou direcionar a conversa a um nível mais aprofundado | SP11 - O(A) médico(a) tentou direcionar a conversa para aprofundar no assunto |
| *Comprehension | SP13, F27, D31 | SP13 - O médico pareceu desejar manter a comunicação com o paciente F27 - O médico quis que a discussão fosse casual D31 - O médico tentou controlar a interação | SP13 - O(A) médico(a) pareceu querer continuar a conversa com o(a) paciente F27 - O(A) médico quis que a discussão fosse descontraída D31 - O(A) médico(a) tentou controlar a interação com o paciente |
Domain encoding [IA - immediacy/affection (I), SP - similarity/depth (II), C - composure (IV) e D - dominance (VI)], followed by item encoding (1 to 34); words and expressions in bold - adjustments.
All pre-test observers considered the instrument comprehensible and easy to apply. One of them, aiming to ensure familiarity in identifying clues related to certain nonverbal behaviors, strengthened the importance of previous training with the scale. Another observer suggested that the instrument should be used for teaching and assessing not only physicians and medical students, but also other health professionals.
After the pre-test, research and language coordinators replaced the words “casual” (item F27) and “relaxado(a)” (item C23) by the words “descontraída” and “tranquilo(a)”, respectively, as suggested by observers (Table 3).
Table 3 Pre-final, pre-test suggestions and final version of Brazilian RCS-O.
| Pre-final item | Pre-test suggestion | Final item |
|---|---|---|
| IA1 - O(A) médico(a) estava intensamente envolvido(a) na conversa com o(a) paciente | IA1 - O(A) médico(a) estava bastante envolvido(a) na conversa com o(a) paciente | IA1 - O(A) médico(a) estava intensamente envolvido(a) na conversa com o(a) paciente |
| SP13 - O(A) médico(a) pareceu querer continuar a comunicação com o(a) paciente | SP13 - O(A) médico(a) pareceu querer continuar a conversa com o(a) paciente | SP13 - O(A) médico(a) pareceu querer continuar a comunicação com o(a) paciente |
| C23 - O(A) médico(a) pareceu muito relaxado(a) ao conversar com o(a) paciente | C23 - O(A) médico(a) pareceu muito tranquilo(a) ao conversar com o(a) paciente | C23 - O(A) médico(a) pareceu muito tranquilo(a) ao conversar com o(a) paciente |
| F27 - O(A) médico(a) quis que a discussão fosse casual b | F27 - O(A) médico(a) quis que a discussão fosse descontraída b | F27 - O(A) médico(a) quis que a discussão fosse descontraída b |
Domain encoding [IA - immediacy/affection (I), SP - similarity/depth (II), C - composure (IV) e F - formality (V)], followed by item encoding (1 to 34); words and expressions in bold - proposed adjustments.
DISCUSSION
Although nonverbal communication is present in every social interaction, it is still underestimated in scientific studies8. To our knowledge, this is the first Brazilian translation and cultural adaptation study of an instrument for teaching and assessing nonverbal medical students’ and physicians’ skills in relational communication in the clinical encounter.
During the translation process, words were changed in order to remove the sexual connotation that could arise from overintimacy in the physician-patient relationship. The words “stimulating”, “warmth”, “desire”, “relaxed”, “conversation to a deeper level”, “deeper relationship”, “casual”, and “intensely” were changed in the consensus stage by independent reviewers, the language coordinator, or during the pre-test. Those changes were particularly important considering this instrument will be used to teach/assess nonverbal communication skills.
The word “desire” (item SP13) may illustrate problems related to polysemy in the teaching/assessment of nonverbal communication skills. This verb holds an ambiguous characteristic, both in English and in Brazilian Portuguese: it means (1) to want something, to wish for something, and (2) to be sexually attracted to somebody44. This explains our choice to use the verb “to want” instead of using “to desire” in the final Brazilian version of the RCS-O.
Likewise, on account of polysemic meanings in Brazilian Portuguese, we decided to change the words “relaxed” (item C23) and “casual” (item F27). In English, “relaxed” is an adjective that represents concepts of being calm, not anxious38 and it does not have the pejorative connotation of carelessness or displeasure on the part of the doctor towards the patient, as it may be case in Brazilian Portuguese45. “Casual”, on the contrary, is also a polysemic word in English, and we chose the adjective “descontraída” to convey the non-formal connotation intended by the scale. “Relaxed” and “casual” could also sound as lack of professionalism in the physician-patient relationship.
Those interpretations and assessments in the translation process called our attention. The examples above bring to discussion the type of intimacy established between physician and patient. Intimacy (physical intimacy/contact and emotional intimacy/feelings) is part of the physician-patient relationship and it is necessary in the therapeutic process. However, it makes patients vulnerable to damages when the limits of this intimacy are crossed46.
Establishing the limits of appropriate and inappropriate intimacy indicates efficiency, reliability, and, as a consequence, good health practice. The ideal limit can be developed and strengthened by the teaching of basic skills, including behavioral ones. The physician’s attention and sensibility to their own nonverbal behavior46 is crucial to good communication and high-quality clinical encounters47.
Although some studies have claimed that nonverbal behavior is mandatory for good medical care, there still is a limited comprehension of the meaning of nonverbal clues, especially concerning the physician-patient interaction46. Assessing this behavior requires caution (Mast, 2007), since many factors may change the “reading” of the nonverbal behavior. Nonverbal behavior expressing intimacy and interest can be understood either as affection or as threat when expressed by strangers8. Similarly, persistent and direct eye contact can be understood as an invasive or a thoughtful behavior46.
Interpreting this communication may vary according to different factors. Cultural47, ecological and historical factors experienced by a particular society (such as wars and agricultural systems)48, personality and connection/intimacy between people8 may play an important role in nonverbal communication. The hierarchical relation in the physician-patient interaction49 is also an important influencing issue in clinical communication.
Despite those influencing factors and the possibility of different interpretations of nonverbal communication, we should not underestimate the importance of teaching and evaluating this skill. The main medical education guidelines50)-(52 state that physicians should constantly watch nonverbal communication in professional health care.
Physicians that are able to cross intercultural borders inherent to any clinical encounter by having adequate behavioral skills are also able to simplify patient-centered health care47 and establish a more effective vertical communication49.
In this context, research on medical education requires teaching and assessment instruments concerning nonverbal communication skills. The use of rigorous translation and adaptation techniques with the participation of a panel of qualified experts and language coordinators in our study resulted in a sound instrument to be used in the Brazilian medical education.
Our study has some limitations. We used video recordings for pretesting the instrument. This approach may have influenced our results. Although video recordings have been used in the original scale validation studies²², this approach may have posed difficulties in assessing students’ and physicians’ nonverbal behavior. Nevertheless, the video approach is used to assess reliability of other nonverbal communication instruments in medical settings38. Also, our sample size did not allow the use of factor analysis of the RCS-O for validation analysis. Therefore, we encourage future validation studies to test the structural validity of the instrument.
CONCLUSION
The process of translation and cultural adaptation of the RCS-O to Brazilian Portuguese resulted in a suitable instrument to be introduced as a tool for teaching and assessing interpersonal communication skills in medical education. Validation studies are needed to elucidate the psychometric parameters of the items and domains of the Brazilian version, especially those adjusted for cultural issues related to intimacy in the doctor-patient relationship. We hope this study may encourage health educators to invest in the teaching and assessment of nonverbal communication skills in other countries.

