











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por email
 Permalink
Permalink
INTRODUCTION
The educational environment (EE) allows students to learn with the interrelationships between classmates, teachers and members of the health team, while encouraging self-confidence. Students’ perceptions about the quality of the educational environment disclose information that is directly related to the teaching-learning process1.
The concept of educational environment (EE) is linked to any context in which teaching and learning take place. Synonyms that are also used for educational environment include “educational atmosphere” and “educational climate”. The EE has an impact on and influence the teaching-learning process, as well as on the quality of work to be developed by undergraduate students and graduates2),(3. The concept of “educational climate” reflects the way in which the student perceives the environment, that is, it informs about their behavior when facing different challenges of educational activities. The same environment can be friendly to one student and/or threatening to another2.
Several factors influence the teaching-learning process, such as facilities, physical and material structure, interpersonal relationships, teaching methodology, ethical and social dimensions, academic services, social assistance programs, institutional assessment policy, teacher qualification, technical-administrative qualification, teacher/student relationship, among others. These influences integrate constitutive elements, favoring the formation of critical and reflective professionals, recognizing the student as an active subject3),(4.
It is necessary to encourage the student to create a reflective thinking, sensitive to current issues, based on and grounded in their life in the society in which they live, in their own social practice, corelating theory with practice5. Teachers, aware of their role in the educational environment, adapt the planning of academic activities to the students’ conditions, seeking to improve their teaching work and mediate the construction of knowledge by the students6.
The educational climate, in the students’ perception, has an impact on the quality of learning. The readjustment of the environment can be an effective strategy to achieve organizational goals, as it contemplates both the needs of the educational institution and the students’ personal expectations and ideas, eliminating the negative effects of dissatisfaction with the training environment and the course4. It is up to the teachers to update their knowledge, be prepared and confident in transmitting their experience, aiming to guide the students in their performance, in the quality of their actions, articulating theory and practice, as a dynamic, interactive process. Clinical teaching aims to develop competencies, facilitating meaningful learning interrelated to the educational teaching environment7)-(9.
Learning in clinical settings and with an early inclusion can direct the medical curricula to the social context of practice, help students transition to the clinical environment, motivate them, make them more confident in dealing with patients and increase self-awareness and the awareness of others10.
In a study to compare the perception of social support and assessment of the educational environment between two groups of medical students, of which one had mentoring support, the Social Support Satisfaction Scale (ESSS, Escala de Satisfação com o Suporte Social) was used to assess the perception of social support and the Dundee Ready Education Environment Measure (DREEM) was used for the assessment of the educational environment. A more critical profile was observed in relation to the perception of social support and the academic environment among students. Mentoring can positively help the students’ trajectory, whether by making them more critical in relation to teaching and their way of learning, or by providing academic support tools11.
When exploring the literature, it was observed that there are instruments that were developed to assess the learning environment, most of them international tools and few aimed at evaluating this environment from the students’ perception in a clinical learning environment.
Clinical Learning Environments (CLE) are considered as encompassing a variety of elements such as learning opportunities, role definitions and attitudes towards teaching and patients, all of which can influence the students’ learning, well-being and satisfaction. The students’ perceptions of CLE also affect the ability to achieve the competencies required to progress in their training and affect how they practice after the training is finished12.
Among the available psychometric instruments, is the “Undergraduate Clinical Education Environment Measure (UCEEM)” created by Strand et al. (2013). The instrument evaluates the students’ perception of the significant aspects of the learning climate in the clinical teaching environment, in addition to providing feedback to the places of educational activity and institutions, on how students perceive the social, emotional and cognitive dimensions of the learning environment13. The UCEEM can be used as a baseline measure and later for the monitoring and evaluation of the effectiveness of interventions to improve the clinical learning environment12.
Considering these facts and due to the absence of validated instruments that address this topic in the Portuguese language, the aim of this study was to adapt cross-culturally the “Undergraduate Clinical Education Environment Measure - UCEEM” instrument into Brazilian Portuguese and validate the translated and adapted version with nursing and medical students who experience clinical teaching during their training.
METHOD
This is a methodological study, which discusses the methods of obtaining, organizing and analyzing data; dealing with the cross-cultural adaptation, creation, validation and evaluation of the instrument, ensuring that the obtained results reveal the differences or similarities between the involved cultures14),(15. The author authorized the translation, adaptation and validation of the instrument and its use in Brazil.
About the instrument
The UCEEM Instrument was created to capture the perception of student satisfaction in the educational environment during clinical teaching. This instrument can be used to recognize the qualities of the learning environment or to identify the actions that should be taken, favoring learning by offering a quality environment, opportunities for academic growth, adequate structure and equipment. The UCCEM allows the evaluation according to the perception of students, how they feel in the clinical teaching environment, how they are welcomed by the team, and whether the structure allows putting the theoretical knowledge into practice13. It has 26 items divided into two dimensions and four subscales or factors: Dimension 1 - ‘Learning Experience’, with F1 Opportunities to learn in and through practice and quality of supervision; F2 Preparation for student admission. In Dimension 2, ‘Social Participation’, we have: F3 Patterns of interaction in the practice scenario; F4 Equal treatment.
The F1 factor refers to the students’ perceptions about the opportunities to learn in and through practical experience and about the process of constructing the meaning of these experiences, together with supervisors and peers (questions 3, 4, 5, 6, 13, 14, 15, 16, 17, 18, 26). F2 reflects the students’ perceptions of the practice setting preparation (educational environment) for student admission and how supervisors/preceptors should make their personal learning experiences based on significant and curriculum-relevant practices (questions 1, 2, 9, 10, 11, 12). The third and fourth factors (F3 and F4) contain variables mapping several aspects related to social participation and equity (F3 questions: 7, 8,19, 20, 21, 22; F4 questions: 23, 24 and 25). To use the instrument in Brazil, it went through the following steps, as shown in Figure 1.
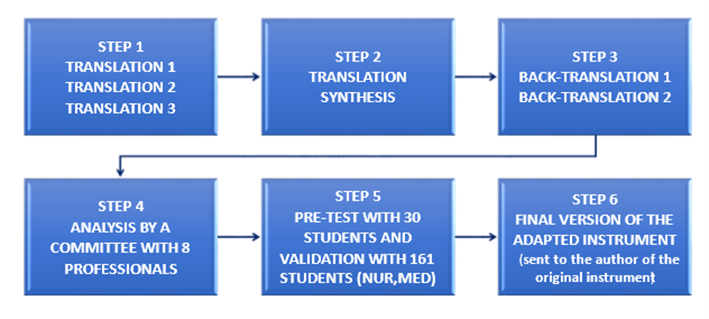
Source: Created by the researcher, adapted from Beaton (2000)16.
Figure 1 Representation of the steps of translation, cross-cultural adaptation and validation of UCEEM.
Translation and cross-cultural adaptation step
For the translation and cross-cultural adaptation of the instrument “Undergraduate Clinical Education Environment Measure (UCEEM)”, the methodological steps of translation, synthesis of translations, back-translation, review by experts, pre-test and validation were followed16.
The translation into Portuguese was performed by three bilingual translators, who were aware of the proposed research objectives and the involved concepts. Two bilingual translators participated in the back-translation, who were not aware of the objectives and involved concepts. The evaluation of the semantic, idiomatic, cultural and conceptual equivalences of the UCEEM items was carried out by a committee of eight expert professionals, five physicians, two nurses and one biomedical science professional, who work as teachers and have a master’s and/or doctoral degree. The Free and Informed Consent Form was sent through e-mail to the experts to be signed together with an Excel spreadsheet containing the items from the original version of the instrument, consensus of the translators and researchers (steps 1 and 2) and consensus of the back-translators and researchers (step 3), with a blank column to describe their considerations about each item of the instrument and the consensus, disclosing their opinion, with the suggested alterations, for better understanding by the target audience.
The results of steps 1, 2 and 3 depicted in Table 1 show the original version, translations T1, T2 and T3 and consensus up to question 1, as well as Back-translations B1 and B2 of the original version of the UCEEM instrument, to illustrate the process.
The translation, back-translation, and expert assessment (step 4) steps were analyzed by the researcher, considering the suggestions of each specialist. Feedback was carried out, with the exchange of messages with the translators involved in the process, until a consensus was reached. After the back-translation performed by the two translators, each one sent their respective versions by e-mail; the researcher grouped the pre-final version of the instrument in Portuguese and the two back-translations in an Excel spreadsheet; the spreadsheet was sent back to the translators, so they could analyze the other back-translation and describe their considerations, analyzing each item; they chose what the best translation would be and what the considerations, adjustments they thought it was necessary to make, aiming to make the instrument as similar as possible to the original version, without changing the meaning of each sentence.
The considerations of professional expert 2 (EX2) were related to item 1, in which they described that “the back-translation does not translate the initially used term, nor does it convey the same message. ‘Reinforcement’ is perhaps not the most appropriate term. The term ‘reinforcement’ chosen by the researchers should perhaps be replaced by ‘initial guidelines’. Thus, item 1 will look like this: ‘I received a useful information/ introduction to this placement / Eu recebi orientações iniciais adequadas’. As for EX8, they also questioned item 1, but regarding the word ‘placement’, which for them, describes that “refers to the internship”.
Validation steps
The validation (step 5) was performed at two different moments; the semantic, idiomatic, cultural and conceptual equivalences (pre-test) with 30 students, 15 from the nursing and 15 from the medical courses, experiencing clinical teaching, attending the second to the twelfth periods, in September and October 2019. The second moment consisted of the validation with 161 students from the same courses, from December 2019 to February 2020. Data collection for validation was carried out with students attending a philanthropic Higher Education Institution (HEI) located in Curitiba, state of Parana, Brazil. The study was approved by the Ethics Committee for Research with Human Beings, under Opinion n. 2.866.282 and CAAE registration n. 96760118.2.0000.5580.
In the pre-test, the instrument was applied in person to students, aiming to monitor the moment when the instrument was filled out. The Free and Informed Consent Form (FICF) was handed out to be read and signed, indicating acceptance to participate in the study, to all students in the selected periods and disciplines. One discipline/curricular unit was chosen for each period of the nursing and medical courses, with authorization from the course coordinator and teacher in charge. Only the students who met the inclusion criteria and agreed to participate in the study signed the FICF. The mean time required to fill out the instrument was approximately twenty minutes. The students described, in the instrument itself, the difficulties or suggestions regarding clarity.
In the validation (step 5), the instrument was applied online, with feedback from 161 students, using the GoogleForms tool. The students who agreed to participate in the study gave their consent through the FICF that was made available and were then directed to the instrument.
To obtain the sample at this step, the researcher, after receiving authorization from the course coordinators, spent two days in all classes of the nursing and medical courses that met the inclusion criteria, to explain about the research, its objectives, the instrument that was being validated and the importance of participation. Among the inclusion criteria, the students had to be enrolled in a nursing or medical course, between the 2nd and 12th semesters, be experiencing clinical education and be over 18 years of age. Students who were not present on the day of the instrument application (in-person phase) and those on a leave of absence or enrolled in the first semester were excluded.
Analysis of the instrument data validated by experts
The instrument that had already been validated by experts (translation and back-translation, as shown in Table 1) was applied to students in two steps, with the aim of testing it in practice. The results were analyzed by Confirmatory Factor Analysis (CFA), through the IBM SPSS AMOS 26.0.0 program, and also by Item Response Theory (IRT), through the eIRT complement (version 1.2.0; http://libirt.sf.net) for Microsoft Excel Software (Microsoft 365®), with analysis through Samejima’s Graded Response Model17. This analysis allows obtaining the instrument’s reliability index, determined by Cronbach’s alpha, as well as the discrimination index, which verifies the association between the global scores of a respondent and the response in each individual item18. The Likert scale is based on questions that were transformed into numbers for the analysis. After the calculation, each question is transformed into a scale that indicates the evaluators’ rate of agreement.
Table 1 Segment of translations T1, T2 and T3, and Back-translations B1 and B2 of the original version of UCEEM instrument.
| Original version | T1 | T2 | T3 | Researcher | Consensus T1, T2, T3 and researcher |
|---|---|---|---|---|---|
| Title: Undergraduate Clinical Education Environment Measure | Title: Medida do ambiente de educação clínica de graduação | Title: Medição Ambiental na Graduação em Educação Clínica | Title: Medida do ambiente de educação clínica de graduação” | Title: Medida do ambiente de ensino clínico de graduação | Title: Medida do ambiente de ensino clínico na graduação |
| 1. I received useful induction to this placement. | 1. Eu recebi indução útil para esta colocação. | 1. Recebi indução útil para este posicionamento | 1. Recebi indução útil para esta colocação. | 1. Recebi reforço útil para esta colocação | 1 Recebi reforço útil para esta colocação |
| Pre-final version of the UCEEM instrument T1, T2, T3 and researcher, back-translation B1 and B2, consensus of the back-translators and researcher. | |||||
| Pre-final version, T1, T2, T3 and researcher | B1 | B2 | Researcher | Consensus B1, B2 and researcher | |
| Title: Medida do ambiente de ensino clínico na graduação | Title: Undergraduate Clinical Education Environment Measurement | Title: Measurement of the clinical graduate education environment | Title: Undergraduate Clinical Education Environment Measurement | Title: Undergraduate Clinical Teaching Environment Measurement | |
| 1 Recebi reforço útil para esta colocação | 1. I received useful reinforcement in this placement | 1. I received helpful reinforcement for this placement. | 1. I received useful reinforcement in this placement | ||
Source: Research data.
Samejima’s model allows obtaining the Operating Characteristic Curve (OCC) of each item. Qualitatively, the conical shape of the curve allows predicting the evaluation power of the question, indicating whether or not it is a good question to assess what is proposed. The sum of the curves for each item indicates whether the instrument itself is adequate to assess the proposed latent trait, which consists in the students’ satisfaction with the educational environment of clinical teaching.
RESULTS
Semantic, idiomatic, cultural and conceptual analyses were the focus of the experts’ validation. These analyses involved qualitative answers provided by each specialist. An example of this type of contribution is: 1) It would be best to hide the subject “I” in the instrument. 2) In fact, the original word “useful” could be replaced by “helpful”. 3) The word “encouraged” could be used to replace the word “stimulated”, adapting to the meaning of the statement.
Based on these contributions, the authors analyzed all the answers and consensually chose the prevailing answers; thus, the questionnaire gradually acquired the characteristics of the final version. Due to its qualitative characteristic, statistical analyses were not performed, as they depend on numerical agreement values.
The analysis of the UCEEM respondents reveals the internal consistency of the instrument translated into Brazilian Portuguese. In the two steps of instrument application, both in the pre-test and in the validation step, the students reported that the instrument was clear, used simple language, with objective, easy-to-understand and self-explanatory questions, directly related to the clinical teaching environment that the students experienced and, thus, it was not necessary to change the instrument.
For the CFA, the 4-factor model originally proposed by the author was adopted, whose result showed a good fit to the model. The values of the fit indices for the questionnaire are shown in Table 2, as well as in the graphical representation of the CFA in Figure 2.
Table 2 Fit index to the model proposed by the CFA.
| Index | Value |
|---|---|
| RMSEA | 0.088 |
| NFI | 0.704 |
| IFI | 0.811 |
| TLI | 0.766 |
| CFI | 0.805 |
Legend: RMSEA - Root Mean Square Error of Approximation; NFI - Bentler and Bonnet´s Normed Fit Index; IFI - Bollen´s Incremental Fit Index; TLI - Tucker-Lewis Index; CFI - Bentler´s Comparative Fit Index.
Source: Research data.
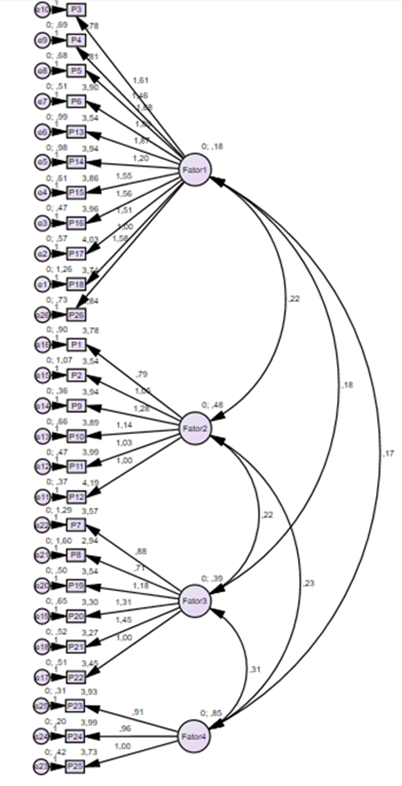
Source: Research data.
Figure 2 Confirmatory Factor Analysis (CFA) for the Brazilian version of the UCEEM instrument.
The indices have values that range from 0 to 1, and the lower the RMSEA index, the better the fit of the model. The other indices indicate that, the higher the values, the better the fit of the model.
The IRT analysis, performed individually for each factor (n=161), showed the following values (F1= 0.858; F2=0.827; F3=0.816; F4=0.882). The author of the original instrument proposed a multidimensional model for “Measure of the Clinical Teaching Environment in Undergraduate Studies”. The values indicate that the model now translated can also be considered multidimensional with four factors, as proposed by the original instrument. In Spearman’s correlation analysis, the data showed that there is a positive correlation between the questions (p<0.05), which contributed to the high alpha value calculated for each factor of the instrument.
The analysis of the instrument’s total curve allowed us to observe that the students, despite developing academic activities in the same school environment, their perception varied from very low to very high. This was reflected in the different skill levels observed in the applied instrument. For each score point (latent trait that varied in the instrument from 55 to 126), there is a function of the amount of information that can be obtained by the instrument. Thus, it is observed that, in all possible scores that can be presented by the instrument, the values are high. This interpretation is shown in Graph 1, which shows the result of the total curve of the items.
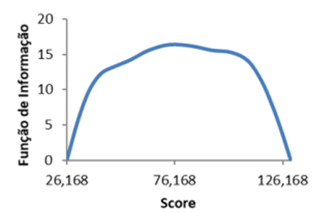
From the individual scores of each participant, it was possible to establish that the observed latent trait (satisfaction with the clinical teaching environment) can be observed and analyzed with this instrument. The minimum and maximum values analyzed varied from -2.290 to 2.601, which is equivalent to the instrument score from 55 to 126, considering that if a student answered 5 in all the alternatives, the score would be 130. It is possible to say that the instrument assesses satisfaction with the educational environment of clinical teaching in a positive way. The score generated by the instrument reliably estimates a multiplicity of results. On the opposite side, if the participant answered 1 in all the alternatives, the value would be exactly 26 points, equivalent to the number of questions. Thus, it is also possible to state that the instrument allows evaluating students who are dissatisfied with the educational clinical teaching environment.
Another item analyzed is the discrimination index, a value that varies from 0 to 1 and indicates the level of clarity of each item. Table 3 shows the mean values of each question and their respective standard deviations, shown in ascending order according to their discrimination index.
Table 3 Mean, deviation and discrimination index values by question, in ascending order of the discrimination index.
| Item | Mean | Deviation | Discrimination |
|---|---|---|---|
| 18. I have the opportunity to learn together with other students in this placement. | 3,744 | 1,200 | 0,337 |
| 8. There is sufficient physical space for the number of students on placement here. | 2,944 | 1,338 | 0,354 |
| 23. Everyone is treated equally here, regardless of cultural background. | 3,925 | 1,007 | 0,437 |
| 14. I feel able to ask my supervisors any question I wish. | 3,944 | 1,108 | 0,447 |
| 25. Everyone is treated with the same respect and dignity, regardless of professional background. | 3,731 | 1,128 | 0,454 |
| 7. I have adequate access to computers. | 3,569 | 1,258 | 0,455 |
| 1. I received useful induction to this placement. | 3,781 | 1,099 | 0,465 |
| 4. I am sufficiently occupied with meaningful (work) tasks. | 3,775 | 1,030 | 0,468 |
| 5. My tasks are suitably challenging for my level of knowledge and skills. | 3,806 | 1,081 | 0,495 |
| 2. My supervisors were expecting me when I arrived. | 3,538 | 1,264 | 0,511 |
| 24. Everyone is treated equally here, regardless of gender. | 3,988 | 0,994 | 0,511 |
| 22.Communication between those working here is good. | 3,453 | 0,950 | 0,531 |
| 11.The supervisors are well prepared for supervising. | 3,994 | 0,994 | 0,546 |
| 21. I feel welcome in the staff room/lunchroom here. | 3,270 | 1,153 | 0,552 |
| 20. I feel included in the team of people who work here. | 3,308 | 1,143 | 0,555 |
| 10. I have sufficient access to supervision. | 3,888 | 1,135 | 0,555 |
| 19. As a student, I am received in a positive way by the staff here. | 3,544 | 1,018 | 0,563 |
| 17. I have the opportunity to put my theoretical knowledge into practice in this placement. | 4,025 | 0,987 | 0,583 |
| 15. I get the opportunity to provide a rationale for my actions during supervision sessions. | 3,856 | 1,018 | 0,590 |
| 13. I receive useful feedback from my supervisors. | 3,535 | 1,268 | 0,593 |
| 9. I have a supervisor to whom I know I can turn. | 3,944 | 1,074 | 0,615 |
| 6. I am encouraged to participate actively in the work here. | 3,900 | 1,068 | 0,621 |
| 26. I feel I have influence over my learning in this placement. | 3,844 | 1,081 | 0,630 |
| 3. My (work) tasks are relevant to the learning objectives. | 4,150 | 0,963 | 0,630 |
| 12. It is clear that my supervisors are familiar with the learning objectives. | 4,194 | 0,925 | 0,642 |
| 16. My problem-solving skills are developing well in this placement. | 3,963 | 0,948 | 0,644 |
Source: Research data.
This index shows the level of certainty that the participant has when differentiating one item from another. The higher the value, the better the level of discrimination. Thus, it is observed that question 16 is the one that best allows to differentiate the participant regarding totally disagree (1) and fully agree (5).
DISCUSSION
The validation of the UCEEM instrument called, after the translation, “Measure of the Clinical Teaching Environment in Undergraduate Studies” (Appendix 1) allowed quantifying and analyzing the subjective characteristics of those involved in the research. The use of validated instruments in the health area allows the verification of the need for intervention in some process or method. Instrument validation and adaptation to the target population’s culture provides reliable validated instruments to be used in different contexts and areas.
The statistical analysis showed that the translated and cross-culturally adapted instrument has good internal consistency, with a positive correlation between the questions. This indicates that the higher the value for each item individually, the higher the result score for the instrument as a whole. This is the desirable standard with this type of instrument, because with it, a scale for measuring the students’ satisfaction with the educational environment for clinical teaching is obtained, which varies from the student with less satisfaction to the one who is completely satisfied.
Considering that satisfaction with the educational environment of clinical teaching is related to the development of clinical competencies, it can be inferred that the instrument is applied to assess students of different academic profiles. This means that the instrument is valid in a wide range of profiles, from different levels of education (periods during undergraduate school). This instrument can be applied to students throughout their undergraduate course, to monitor the satisfaction of the clinical teaching educational environment.
Satisfaction with the performance of academic activities can be considered as commitment, which is perceived in the individual by the energy that is spent, the involvement and the effectiveness when performing a certain activity, since their values are considered whether in the work or in the study environment. Committed students feel connected to their activities and perceive them as a positive challenge, since variables such as social support, self-efficacy, degree of personal satisfaction, and autonomy encouragement help in the performance and achievement of academic goals19.
The stimulating learning environment involves learning objectives, partnering with supervisors, opportunities to interact with patients and allowing students to take responsibility. The good relationship of the supervisor/preceptor with the student and effective guidance is essential in the teaching-learning process20.
The evaluation of the educational environment in the United States of America (USA) is often carried out in schools, aiming at evaluating the educational climate, the perception of students and staff. The research shows, through the employees’ perception, that the educational climate influences the results during the workday21.
The study carried out with nursing students at the Universiti Kebangsaan Malaysia Medical Centre in Malaysia, also reported that the good relationship between the supervisor and the student influences the teaching-learning process, resulting in a better understanding of the content by the student22.
Regarding the clinical teaching in health, the literature indicates the importance of supervisors/preceptors, their training for supervision, and the student’s perception of the supervisors. There is reference to the fact that they are trained and qualified professionals to supervise, since the supervised internship is an opportunity for the student to expand their knowledge and put them into practice. Supervisors, in addition to countless contributions, need to convey security to the student when developing their activities into practice, emphasizing what needs to be improved9),(23.
Students reported in a survey that being actively committed with the learning process, receiving appropriate clinical supervision, and value the staff members to help support patient care were expectations of supervised students in the obstetrics and gynecology internship24),(25.
The supervision carried out by the teacher in clinical teaching aims to prepare the student for their professional practice, provide commitment with the environment they are in and with the work team, develop clinical skills, plan the systematization of care and people management, and contribute to the development of educational actions, among others26.
When the student is committed with the educational environment and feeling like a participant, these are aspects that contribute to their academic performance, personal and professional growth27. A study carried out at the Universiti Kebangsaan Malaysia Medical Centre also states that the educational environment has an influence on student learning, as it allows the student to acquire knowledge and skills that will prepare them for their professional practice22.
In the study carried out in the USA, it was learned that the commitment among employees of educational institutions will provide a collaborative environment, as they will identify common goals and this will allow developing a relationship of trust between managers and employees, helping employees to achieve their work goals with greater motivation21.
CONCLUSION
It was possible to reach and respond to the proposed objectives of this research, aimed at the translation, cross-cultural adaptation and validation of the translated and adapted version into Brazilian Portuguese with nursing and medical students. In these two courses, satisfaction with the educational environment is essential for the development of clinical teaching.
After the validation, the instrument can be applied to several courses in the health area, allowing other researchers and educational institutions to use it in their own contexts.
The Item Response Theory showed to be efficient in measuring latent variables that cannot be directly verified. The validated instrument showed an adequate profile for the assessment of satisfaction with the educational environment in clinical teaching in different student profiles. In this context, learning about student satisfaction with the educational environment in clinical teaching implies adapting the educational environment to the students’ expectations to better favor learning in clinical teaching.
The original instrument has four factors, which were maintained in the version translated into Brazilian Portuguese, showing to be reliable for use in undergraduate courses in the health area for the Measure of the Clinical Teaching Environment in Undergraduate Studies.

