











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por email
 Permalink
Permalink
INTRODUCTION
The Impostor Syndrome (IS) has been described in women with professional and academic success who feel they are deceiving others regarding their level of intelligence, doubting their own intellectual capacity and feeling like impostors in their achievements1.
The characteristics of this syndrome have been described as (1) the feeling of having deceived others to overestimate their ability, (2) the attribution of success to something other than intelligence or ability, and (3) the fear of being exposed as a fraud2.
Some authors have identified an IS prevalence of 30% among medical, dental, nursing and pharmacy students. This factor was considered the strongest predictor of psychological distress among students3. Until now, only one study investigated the association between Burnout Syndrome (BS) and IS in undergraduate medical students4.
Additionally, in order to identify the consequences of this condition, other authors have shown that IS-related feelings were associated with increased rates of anxiety, depression and burnout5. Female gender4),(6, low self-esteem7, perfectionism3 and the frequent hierarchy experienced in undergraduate and graduate medical courses8 have been listed as risk factors for IS among medical students. Meanwhile, social support, validation of success, positive affirmation and institutional support have been associated with protection against IS9.
Despite the recent increase in the number of publications on IS10, the scarcity of data in the literature on this condition in undergraduate medical students limits knowledge about the prevalence and impact on mental health7),(11. This study aims at assessing the prevalence of IS in undergraduate medical students in Brazil and its association with Burnout Syndrome and depression.
METHODS
Study design and participants
A descriptive and quantitative cross-sectional study was conducted with undergraduate medical students at a university center in northeastern Brazil. Estimated at 95% reliability and a 5% margin of error, the sample size comprised 247 participants. However, the obtained sample had 425 participants, which allowed for an increase in the study reliability with a 2.93% margin of error. Students who did not give their informed consent were excluded from the study. To calculate the sample size, a prevalence value of 30% was considered as a reference, according to a previous study3. The sample size was calculated using Solvis free sample calculator (available at https://solvis.com.br/calculos-de-amostragem/).
The participants were recruited at the university center, covering all pre-internship semesters of the course, and proportional to the number of students in each school semester. The medical course is divided into four years of pre-clinical and clinical content and two years of internship. The course has a total of 918 students from the 1st to 4th year and 388 students in the internship period. The school uses a hybrid teaching methodology, with traditional lectures and an active student-centered model called Problem-Based Learning (PBL) for 8 hours a week or Team-Based Learning (TBL) in 1 session per semester. Practical activities involve simulation with actors as standardized patients for 4 hours a week, aimed at stimulating and integrating reasoning and activities in clinical settings with real patients and assisted by preceptors.
Measurements
Sociodemographic questionnaire
The questionnaire used to assess the study participants' sociodemographic data was formulated by the authors. It includes questions on age, gender, school semester, marital status, whether they have a paid activity, are income providers, have leisure time and practice any type of physical activity.
Clance Impostor Phenomenon Scale (CIPS)
The Clance Impostor Phenomenon Scale (CIPS) questionnaire, adapted for use in Brazil12, was used to detect IS indicators1. The questionnaire consists of 20 questions that aim at identifying the following: (1) fear of assessment, (2) fear of not being able to repeat success and (3) fear of being less capable than others. The questions were answered using a five-point Likert scale, varying between 1 (not at all true) and 5 (very true), and the result identified the level of IS-related symptoms. The IS symptoms were classified as mild (≤ 40 points), moderate (41-60 points), severe (61-80 points) and very severe (> 80 points).
Maslach Burnout Inventory - Student Survey (MBI-SS)
To assess the students' self-perception of Burnout, we used the MBI-SS (Maslach Burnout Inventory - Student Survey), which was adapted into Brazilian Portuguese13 and the authors paid for the instrument's copyright. The MBI-SS consists of 15 questions subdivided into the following three subscales: Emotional Exhaustion (5 items), Cynicism (4 items), and Professional Efficacy (6 items). All items were assessed by frequency using the following Likert scale (0-6): 0 (never), 1 (once a year or less), 2 (once a month or less), 3 (a few times a month), 4 (once a week), 5 (a few times a week), and 6 (every day). The cut-off points to identify the presence of BS were Emotional Exhaustion ≥ 21, Cynicism ≥ 16 and Professional Efficacy ≤ 18. BS was considered in students with the presence of two (Emotional Exhaustion and Cynicism) or three (Emotional Exhaustion, Cynicism and Professional Efficacy) criteria, as previously described in the literature14.
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 consists of nine questions that assess the presence of each of the symptoms for the episode of major depression15. The nine symptoms consist of depressed mood, anhedonia (loss of interest or pleasure in doing things), sleep problems, tiredness or lack of energy, change in appetite or weight, feelings of guilt or worthlessness, concentration problems, feeling either slow or restless and suicidal thoughts. The frequency of each symptom in the last two weeks is assessed on a Likert scale from 0 to 3, corresponding to the “never”, “several days”, “more than half of the days” and “almost every day” answers, respectively. The questionnaire also includes a tenth question assessing the interference of these symptoms in the performance of daily activities, such as working and studying. The interpretation of the scale depends on the sum of points from Questions 1 to 9, being classified as follows: 0-4: Minimal depression; 5-9: Mild depression; 10-14: Moderate depression; 15-19: Moderate to severe depression; 20-27: Severe depression. The PHQ-9 was previously used in the Brazilian population16.
Ethics approval and consent to participate
The study was approved by the institution's Research Ethics Committee, CAAE: 10294519.4.0000.5049, in compliance with Resolution 466/12 of the National Health Council and the Declaration of Helsinki. The research subjects participated voluntarily, after signing the Free and Informed Consent Form, and were not identified, so as to ensure confidentiality of the answers.
Analysis
The data were analyzed using the Statistical Package for Social Sciences (SPSS, Chicago, IL), version 20. They were summarized using descriptive statistics such as proportion, frequency and mean values. Pearson's chi-square test was used to explore associations and relationships between variables. The relationship between IS, severity of depression symptoms and the Burnout components was analyzed using Spearman's correlation coefficient. A p-value ≤ 0.05 was considered statistically significant.
RESULTS
The study included 425 students with a mean age of 23.03 ± 5.0 years, which represents 62.1% of the total of pre-internship undergraduate medical students from the university center. In this sample, 47 (11.06%), 151 (35.53%), 163 (38.35%) and 64 (15.06%) participants had mild, moderate, severe and very severe IS symptoms.
There were no statistical differences regarding age, gender, current school semester, performance of paid activity or time devoted to leisure activities or hobbies among the individuals with the four levels of IS symptoms (Table 1).
Table 1 Undergraduate medical students’ demographic data and Impostor Syndrome evaluation (n = 425).
| Clance Impostor Phenomenon Scale (score) | |||||
|---|---|---|---|---|---|
| <40 | 41-60 | 61-80 | >80 | p | |
| Age (years) | |||||
| ≤ 21 | 18 (38.3%) | 70 (46.4%) | 80 (49.1%) | 35 (54.7%) | .369 |
| 22 or more | 29 (61.7%) | 81 (53.6%) | 83 (50.9%) | 29 (45.3%) | |
| Gender | |||||
| Female | 21 (44.7%) | 53 (35.1%) | 55 (33.7%) | 25 (39.1%) | .533 |
| Male | 26 (55.3%) | 98 (64.9%) | 108 (66.3%) | 39 (60.9%) | |
| Current school semester | |||||
| 1st | 10 (21.3%) | 22 (14.6%) | 26 (16.0%) | 9 (14.1%) | .661 |
| 2nd | 1 (2.1%) | 14 (9.3%) | 20 (12.3%) | 10 (15.6%) | |
| 3rd | 6 (12.8%) | 21 (13.9%) | 18 (11.0%) | 10 (15.6%) | |
| 4th | 8 (17.0%) | 19 (12.6%) | 18 (11.0%) | 8 (12.5%) | |
| 5th | 5 (10.6%) | 26 (17.2%) | 17 (10.4%) | 11 (17.2%) | |
| 6th | 2 (4.3%) | 9 (6.0%) | 13 (8.0%) | 3 (4.7%) | |
| 7th | 5 (10.6%) | 16 (10.6%) | 19 (11.7%) | 2 (3.1%) | |
| 8th | 10 (21.3%) | 24 (15.9%) | 32 (19.6%) | 11 (17.2%) | |
| Married | |||||
| No | 36 (76.6%) | 131 (86.8%) | 154 (94.5%)* | 63 (98.4%)* | < .001 |
| Yes | 11 (23.4%)* | 20 (13.2%)* | 9 (5.5%) | 1 (1.6%) | |
| Paid activity | |||||
| No | 43 (91.5%) | 132 (87.4%) | 151 (92.6%) | 57 (89.1%) | .461 |
| Once a week | 4 (8.5%) | 19 (12.6%) | 12 (7.4%) | 7 (10.9%) | |
| Income provider | |||||
| No | 44 (93.6%) | 134 (88.7%) | 156 (95.7%)* | 63 (98.4%)* | .025 |
| Once a week | 3 (6.4%)* | 17 (11.3%)* | 7 (4.3%) | 1 (1.6%) | |
| Leisure activites or hobbies | |||||
| Less than half an hour | 4 (8.5%) | 30 (19.9%) | 34 (20.9%) | 13 (20.3%) | .559 |
| Between half an hour and 1 hour | 18 (38.3%) | 40 (26.5%) | 57 (35.0%) | 21 (32.8%) | |
| Between 1 and 2 hours | 20 (42.6%) | 63 (41.7%) | 57 (35.0%) | 22 (34.4%) | |
| More than 2 hours | 5 (10.6%) | 18 (11.9%) | 15 (9.2%) | 8 (12.5%) | |
| Physical activity practice | |||||
| No | 10 (21.3%) | 55 (36.4%) | 55 (33.7%) | 29 (45.3%)* | .032 |
| Once a week | 7 (14.9%) | 9 (6.0%) | 16 (9.8%) | 10 (15.6%) | |
| 2 to 3 time a week | 12 (25.5%) | 37 (24.5%) | 51 (31.3%)* | 11 (17.2%) | |
| More than 3 times a week | 18 (38.3%)* | 50 (33.1%)* | 41 (25.2%) | 14 (21.9%) | |
| Anxiety diagnosis | |||||
| No | 42 (89.4%)* | 126 (83.4%)* | 114 (69.9%) | 51 (79.7%) | .006 |
| Yes | 5 (10.6%) | 25 (16.6%) | 49 (30.1%)* | 13 (20.3%)* | |
| Depression diagnosis | |||||
| No | 46 (97.9%)* | 140 (92.7%)* | 152 (93.3%)* | 53 (82.8%) | .019 |
| Yes | 1 (2.1%) | 11 (7.3%) | 11 (6.7%) | 11 (17.2%)* | |
| Panic disorder diagnosis | |||||
| No | 47 (100.0%) | 149 (98.7%) | 159 (97.5%) | 64 (100.0%) | .412 |
| Yes | 0 (0.0%) | 2 (1.3%) | 4 (2.5%) | 0 (0.0%) | |
| Psychological follow-up | |||||
| No | 40 (85.1%)* | 121 (80.1%)* | 119 (73.0%) | 42 (65.6%) | .045 |
| Yes | 7 (14.9%) | 30 (19.9%) | 44 (27.0%)* | 22 (34.4%)* | |
| Psychiatric follow-up | |||||
| No | 44 (93.6%) | 130 (86.1%) | 135 (82.8%) | 51 (79.7%) | .187 |
| Yes | 3 (6.4%) | 21 (13.9%) | 28 (17.2%) | 13 (20.3%) | |
| Antidepressant use | |||||
| No | 47 (100.0%)* | 139 (92.1%) | 141 (86.5%) | 53 (82.8%) | .011 |
| Yes | 0 (0.0%) | 12 (7.9%)* | 22 (13.5%)* | 11 (17.2%)* | |
| Anxiolytic use | |||||
| No | 45 (95.7%) | 139 (92.1%) | 142 (87.1%) | 55 (85.9%) | .179 |
| Yes | 2 (4.3%) | 12 (7.9%) | 21 (12.9%) | 9 (14.1%) | |
Note: Pearson's chi-square test. Source: prepared by the autors.
Not being married, having a low level of physical activity and not contributing to the family income were associated with severe or very severe IS symptoms. Previous medical diagnosis of depression, anxiety and the use of antidepressants were also associated with severe or very severe IS symptoms. This association was not observed with panic disorder or use of anxiolytics (Table 1).
The students with severe or very severe IS symptoms were more often followed by a psychologist, but this was not observed in relation to the assistance provided by a psychiatrist (Table 1).
There was an association between severe and very severe IS level and a PHQ-9 scale score that indicated moderate, moderate-high and high depressive disorder (Figure 1).
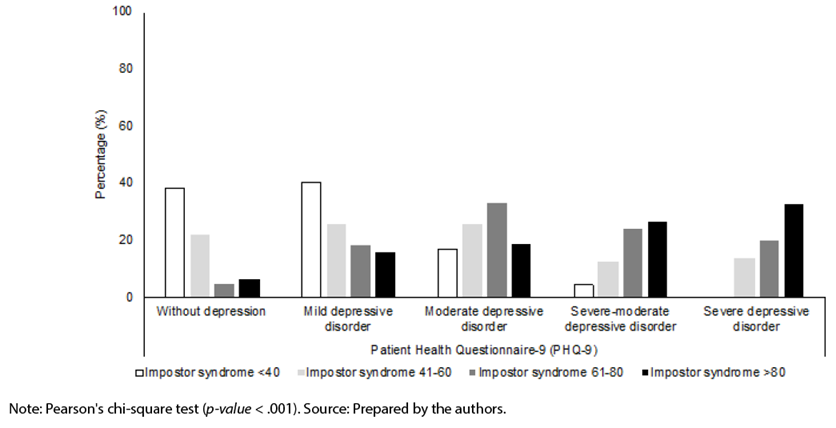
Figure 1 Association between depression and Impostor Syndrome in undergraduate medical students (n = 425).
A positive correlation was identified between IS and the severity of depression symptoms (ρ = .459, p < .001).
A significant association was also identified between severe and very severe IS levels and high levels of the Emotional Exhaustion and Cynicism components identified through the Burnout Syndrome scale. There was an association between severe and very severe IS level and the perception of high Professional Efficacy by the Burnout Syndrome scale (Figure 2).
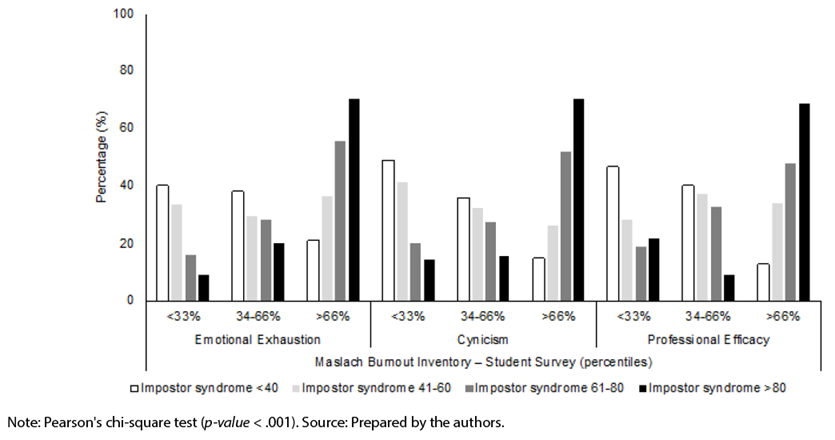
Figure 2 Association between Burnout and Impostor Syndrome in undergraduate medical students (n = 425).
A positive correlation was identified between IS and the Emotional Exhaustion (ρ = .384, p < .001), Cynicism (ρ = .384, p < .001) and Professional Efficacy (ρ = .302, p < .001) components. BS evaluated by the presence of the three criteria was not associated with IS (p = .088); however, the use of a two-dimensional evaluation (Emotional Exhaustion and Cynicism) showed an association between BS and IS (p < .001).
DISCUSSION
This study showed a high prevalence of IS in medical students, regardless of the attended semester during the pre-internship period. The facts of not being married, not contributing to family income and not practicing any type of physical activity were associated with IS. Moreover, there was a significant association with the diagnoses of depression, anxiety and antidepressant use. As for the Burnout components, there was a positive association of Emotional Exhaustion and Cynicism with IS. Higher scores for IS were associated with higher scores for Professional Efficacy, identified by linear correlation analyses. This finding suggests that, despite the perception of efficacy in academic tasks, there must be skepticism about one’s personal capacity to achieve this efficacy.
Although most studies about IS have been conducted in the USA and Canada, twenty-one studies evaluated populations in other countries, including five in Austria, five in Australia/New Zealand, four in Germany, three in Iran, two in the UK, two in Pakistan and one in Belgium, Korea and Malaysia each10. Eight studies evaluated medical students5.
A similar study with Malaysian graduate medical students also identified a high prevalence of IS, characterized by a score of 62 as the cut-off value (48% of men and 44% of women). In this study, carried out in an underdeveloped/developing country such as Brazil, the authors also identified a positive correlation between IS and depression and anxiety. In addition, IS was associated with the feeling that they were unable to cope with challenges during internship17.
A study conducted with 189 medical students in Pakistan found 59.25% of IS, according to the Clance impostor phenomenon scoring18, with severe or very severe IS rates, even higher than our findings. In another cross-sectional study, conducted in a private medical college of Lahore, Pakistan, with 143 final-year medical students, the prevalence of IS according to the Young Impostor scale was 47.5%6. In the USA, a study with 169 first-year medical students at Saint Louis University identified 31.9% of “high” or “intense” impostor phenomenon scores19.
In a study conducted with a sample of 59% of undergraduate medical students at the University of Kansas Medical School, which had a traditional 4-year pre-internship program, 41% reported moderate impostor feelings (score 40-60), 38% frequent impostor feelings (score 60-80) and 13% intense impostor feelings (score > 80)20.
The prevalence values for IS in developed or in underdeveloped/developing countries were similar to those identified in the current study with undergraduate medical students in Brazil. The association of female or male gender with IS was not identified in this study and is still controversial in the literature. Some studies showed a statistically significant difference in IS rates between male and female medical students3)-(4),(6),(20, whereas others found no difference7),(11),(16),(21)-(22. The Impostor phenomenon was assumed initially to be predominant in high-achieving women. However, further studies showed that this phenomenon is also quite frequent among male individuals. Some researchers found the gender variable to be nonsignificant regarding the prevalence and severity of the Impostor phenomenon20.
Medical education is demanding and the transition into the clinical practice can be a particularly challenging phase of training. The earlier training years seem to be associated with greater psychological distress3. According to Maqsood et al. (2018)18, third-year students were found to have a high prevalence and degree of IS severity. The current study found high prevalence of IS regardless of the semester attended during the pre-internship period. Other authors stated that progress into senior classes or senior training years does not exert any effect on the Impostor phenomenon; therefore, if a student suffers from it, they will continue suffering from this phenomenon despite any advancement in their schooling levels6),(18.
Unfortunately, there is not much data on the influences of gender, race, income or physical activity on the development of IS and it is important to better understand these populations if we hope to reduce the effects of IS among health professionals. Being married, for example, may act as a buffer against psychological distress during professional training.
Association of the Impostor Syndrome with depression
According to some authors, depression and anxiety were particularly important characteristics of those with impostor feelings, as well as those with low self-discipline and perceived competence23. This study not only identified an association between IS and the established medical diagnoses of anxiety and depression, but also showed a relationship between IS and greater severity of depressive symptoms in medical students.
In the study with 256 medical students from Malaysia, positive correlations were found between IS and depression (ρ = .42) and anxiety (ρ = .41)17. However, there is a scarcity of data on medical students that evaluated this association. In a study conducted with 255 Family Medicine residents in Wisconsin, 41% of the women scored as impostors, when compared to 24% of the men (p = .02). The impostor scores were also correlated with depressive symptoms (r2 = .45, p < .0001), as well as with trait anxiety (r2 = .65, p < .0001) and state of anxiety (r2 = .39, p < .0001)24.
Association between the Impostor Syndrome and Burnout
Some studies have identified that IS was also correlated with increased levels of the Burnout components of Emotional Exhaustion and Cynicism, as well as with decreased job satisfaction rates25)-(26. At this time, only one study has investigated the association between IS and Burnout in undergraduate medical students. One hundred and thirty-eight medical students from Jefferson Medical College, USA, participated in the study and IS was significantly associated with the Burnout components of Emotional Exhaustion (χ2 = 8.0, p = .018) and Depersonalization (χ2 = 10.3, p = .006)4.
Even studies carried out with medical residents found this association. A study carried out with general surgeons and general surgery residents in the city of Minneapolis showed an association of Burnout with clinical IS symptoms (OR 3.95, p = .017)22. In another study with 200 Dermatology residents, 89% of the respondents (n=108) had IS, with moderate to intense impostor tendencies. The odds of Burnout for those with IS was 19.61 (p < .005). IS showed a moderate positive correlation with Emotional Exhaustion and Depersonalization (r = .4100, p < .001; r = .3126, p = .0005, respectively), and a moderate negative correlation with Professional Efficacy (r = -.3355, p = .0002)27.
The current study also identified an association between Burnout and IS and can contribute to a better understanding of the relationship between these conditions. The identification of this association in undergraduate medical students may positively impact our capacity to prevent Burnout among medical professionals.
Limitations
There are limitations to this study, namely: non-inclusion of medical internship students, who are likely to suffer from greater mental and physical demands, and the cross-sectional design of the study, which does not allow determining the cause-and-effect relationships between IS and Burnout, depression or anxiety. The cross-sectional, quantitative and descriptive nature of the study did not allow performing the qualitative analysis of this phenomenon regarding its possible origins, the students' self-knowledge in relation to the feeling that leads to it, the influence of the individuals' intrinsic factors, such as gender or skin color and the influence of extrinsic factors, such as pressure from teachers. In addition, generalization of the findings should be performed with caution, as the study was conducted in a single University Center.
Implications
Despite these limitations, this study was important because it showed a relevant association between IS and Burnout, depression and anxiety in undergraduate medical students. Moreover, there is a current lack of data in the literature on this condition in undergraduate students, which limits knowledge about the prevalence and impact on mental health. The development of IS among medical students can have long-term effects, given its association with symptoms of anxiety, depression, emotional exhaustion and cynicism.
Identifying IS symptoms in medical students in the pre-clinical stages can predict those at risk of facing difficulties in the future in their professional practice and life and can help prevent Burnout. This predictive value has recently brought “IS” among pre-internship students as the focus of research. One reason can be its strong association with the “Burnout phenomenon” and, thus, the increasing number of dropouts and suicides among the students.
The subjects of the current research were not identified. The results were reported to the institution's Pedagogical Support Center to promote awareness and prevention actions on Burnout and IS.
Other studies are necessary to guide interventions and institutional strategies against IS. Many institutions programs to treat impostor syndrome are part of their orientation activities. These programs help students find whether they have the tendency or not and, if they do, to encourage them to join such programs. The students may be trained to understand perfectionism and how to set expectations for themselves that are more reasonable and achievable. Meanwhile, similar programs should be developed for the faculty, staff and administration. They should be trained to identify those students in need of support and provide them with help to cope with the problem and improve their well-being.

