











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Complementary and Alternative Medicine (CAM) is a set of interventions and unconventional approaches used in health care, which relies on individual integrality, taking into consideration the global dimension without losing sight of the individual’s singularity, to help explain their processes of illness and health, it is also known as holistic or systemic medicine [1; 2; 3]. The demand for unconventional therapies in treatment of various diseases and health problems has been increasing in recent decades and such treatment have been applied in a complementary or integrated manner in relation to the traditional biomedical model. These practices have been introduced into the health system through their incorporation into care programs in several Western nations [4; 5]. This also relates to a World Health Organization (WHO) recommendation, since the declaration of Alma Ata at the International Conference on Primary Health Care in 1978 [6; 7; 8], and more recently with the publication of the Strategies for Traditional and Integrative Medicines, which established implementation targets for its Member States for the period from 2014 to 2023 [ 9 ].
In Brazil, the legitimization and institutionalization of these approaches to health care began in the 1980s, mainly after the creation of the “Sistema Único de Saúde” (SUS, or Unified Health System) . In 2006, the Ministry of Health implemented the National Program of Integrative and Complementary Practices (NPICP). The program advocates incorporation of practices such as Phytotherapy, Acupuncture, Thermalism, and Anthroposophic Medicine in the SUS [1; 11; 12]. This process, which began with the WHO recommendation, emphasized the importance of integrating traditional non-biomedical practices and so-called “alternatives” toward a reformulated and expanded national health service [1; 7].
The great challenge in NPICP implementation is the lack of sufficient professionals to meet this demand and exercise these practices within the SUS. Despite being recognized as medical specialties by Brazilian governmental institutes for over two decades, Homeopathy and Acupuncture are provided by health services but, in accordance with the population’s demand, they are irrelevant and insufficient [ 12 ].
Therefore, there is a demand for training human resources to fill this gap in the public health care network, especially for new medical professionals. In Brazil, CAM teaching is unexplored and not mandatory in most undergraduate medical course syllabi [ 4 ].
The National Curricular Guidelines (NCG) for Medicine courses proposed by the Ministry of Education in 2001 (and revised in 2014) define the principles, fundamentals, conditions and procedures for the training of physicians, established by the Higher Education Chamber of the National Education Council, for nationwide application in the organization, development and evaluation of the pedagogical projects of the Undergraduate Medicine Courses in Brazil. The guidelines are related to the whole health-disease process of the citizen, the family and the community, integrated to the epidemiological and professional reality, providing the integrality of the actions of care in medicine [ 13 ].
In order to be able to follow the NPICP in the SUS and effectively introduce these specialties, it is necessary for medical schools to add this curricular content to their pedagogical projects for undergraduate courses, so that future physicians are aware of their existence and purpose and can apply them in practice.
Thus, the objective of this research is to investigate the teaching of CAM at medical schools in Brazil and to identify the potential for training professionals in this area.
METHODOLOGY
An observational and exploratory study was conducted, with a descriptive and analytical cross-sectional design and a quantitative approach. This study was carried out at every Brazilian medical school from May 2016 to March 2017. The main bases used included data obtained from a research questionnaire applied to management and teachers in the five regions of the country, the curricular syllabus of the courses and data from the Ministry of Education (MEC) and the Instituto Nacional de Estudos e Pesquisas Educacionais Anísio Teixeira (INEP) . All medical schools in the year 2016 were included in the study. This study considered the administrative characteristics of the medical schools, geographical and regional distribution, methodological educational approach and CAM teaching at medical schools. Descriptive and analytical elements were considered to obtain the following variables: total number of schools, number of schools with CAM education, relationship between number of schools and offer in the capital and in the interior, applied methodologies and the offer of the subject and the work regime of teachers in CAM.
Descriptive analysis was performed with the presentation of the variables using frequency distribution and the Pearson correlation coefficient (X2)-Chi-square. The proportions were compared using the Chi-square test or Fisher’s Exact Test. When the expected value of a contingency table was equal to or greater than 5, the Chi-square test was used; in all other situations, Fisher’s Exact Test was used. The difference between proportions was estimated by the Odds ratio (OR), calculated through simple logistic regression, with a 95% confidence interval (95% CI). The study was approved by the Research Ethics Committee of the University of Fortaleza under number 1.540.537 in accordance with the principles of the National Ethics Commission in Research and in respect to resolution number 466/12 of the National Health Council / Ministry of Health. Agreement was given through the informed consent form (ICF).
RESULTS
We evaluated 272 (100%) medical schools distributed throughout five regions of the country. There was a predominance of medical schools located in the Southeast region, corresponding to 41 percent of the total.
There is an even distribution of medical schools, considering the percentage of population by region, but when considering the ratio of the number of available places per inhabitant per region, the total university courses in the Southeast region is the largest in relation to the rest of the country, while the North and Northeast regions have the lowest ratio of available places per inhabitant ( Table 1 ).
TABLE 1 Relationship of the number and annual available places in medical schools by region and inhabitants of Brazil.
| Nr. places /Year | Population | Places/10.000 habitants | |
|---|---|---|---|
| North | 1,847 | 17,707,783 | 1.04 |
| Northeast | 6,966 | 56,915,936 | 1.22 |
| Midwest | 2,100 | 15,660,988 | 1.34 |
| South | 3,936 | 29,439,773 | 1.34 |
| Southeast | 11,756 | 86,356,952 | 1.36 |
| Brazil | 26,650 | 206,081,432 | 1.29 |
Regions ordered by number of available places per 10,000 inhabitants.
Trend Test of Number of Places: p-value = 0.538
Source: Research data 2016 (prepared by the author).
It was found that only 57 of the 272 existing and active medical schools currently address CAM in their curriculum and are distributed throughout the five regions of the country. The number of medical schools with CAM education is proportionally higher in the South and Midwest, corresponding to almost a quarter of the existing courses in each of these regions ( Table 2 ). The Northeast displays significant growth in number of medical schools and also in the teaching of CAM, but the Southeast holds more than a third of the medical schools in the country and the same proportion refers to schools that have a CAM approach. Therefore, no significant difference was found in the distribution of schools with CAM teaching in the five regions of the country. There is a statistically significant difference in the number of schools in the capitals of the Northeast region in relation to smaller cities of this region as regards the teaching of CAM.
TABLE 2 Distribution of all Medical Schools and Schools with CAM teaching by administrative regions in Brazil (2016).
| Regions | Total schools | Teaching of CAM | Odds ratio (OR) | |||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| N | % | P value | OR | Standard error | CI 95% | P value | ||
| North | 22 | 3 | 13.6 | 1 | – | – | – | |
| Northeast | 70 | 16 | 22.9 | 1.9 | 1.3 | 0.49-7.2 | 0.357 | |
| Southeast | 112 | 21 | 18.8 | 0.756 | 1.5 | 0.97 | 0.39-5,4 | 0.569 |
| South | 43 | 11 | 25.6 | 2.2 | 1.6 | 0.54-8.8 | 0.275 | |
| Midwest | 25 | 6 | 24 | 2.0 | 1.6 | 0.44-9.2 | 0.373 | |
| Brazil | 272 | 57 | 21 | – | ||||
Source: Research data 2016 (prepared by the author).
The increase in the total number of medical schools in relation to the number of schools with CAM teaching, especially in the last ten years, has not been significant.
Currently, most medical schools in Brazil have a private administrative regime. Around 46% are public (29% national, 13% state and 5% municipal). However, in relation to the teaching of CAM, there is predominance in the public sector (64.91%). Most of the schools that teach CAM in Brazil are Federal Public Administrations, mainly in the Northeast and South. In the Southeast, the teaching of such practices is found mainly in state or private schools. Of all the regions, the North was the one that had the least growth, both in number of schools and in the teaching of CAM. In the Midwest, Northeast and Southeast regions, the proportion of public schools is higher, and proportion of schools with CAM is higher, while the opposite occurs in the South and North regions. It is observed that the Southeast states have the highest concentration and number of medical schools and of CAM teaching.
The medical schools with CAM adopt mostly active methodologies (AM) of teaching learning, with a predominance of Problem-Based Learning (PBL), while one-third of the schools adopt a traditional methodology. Other methodologies used in accordance with the pedagogical political projects, besides PBL, are: General Practitioner, Humanistic, Non-Traditional, and Community Education. ( Figure 1 ).
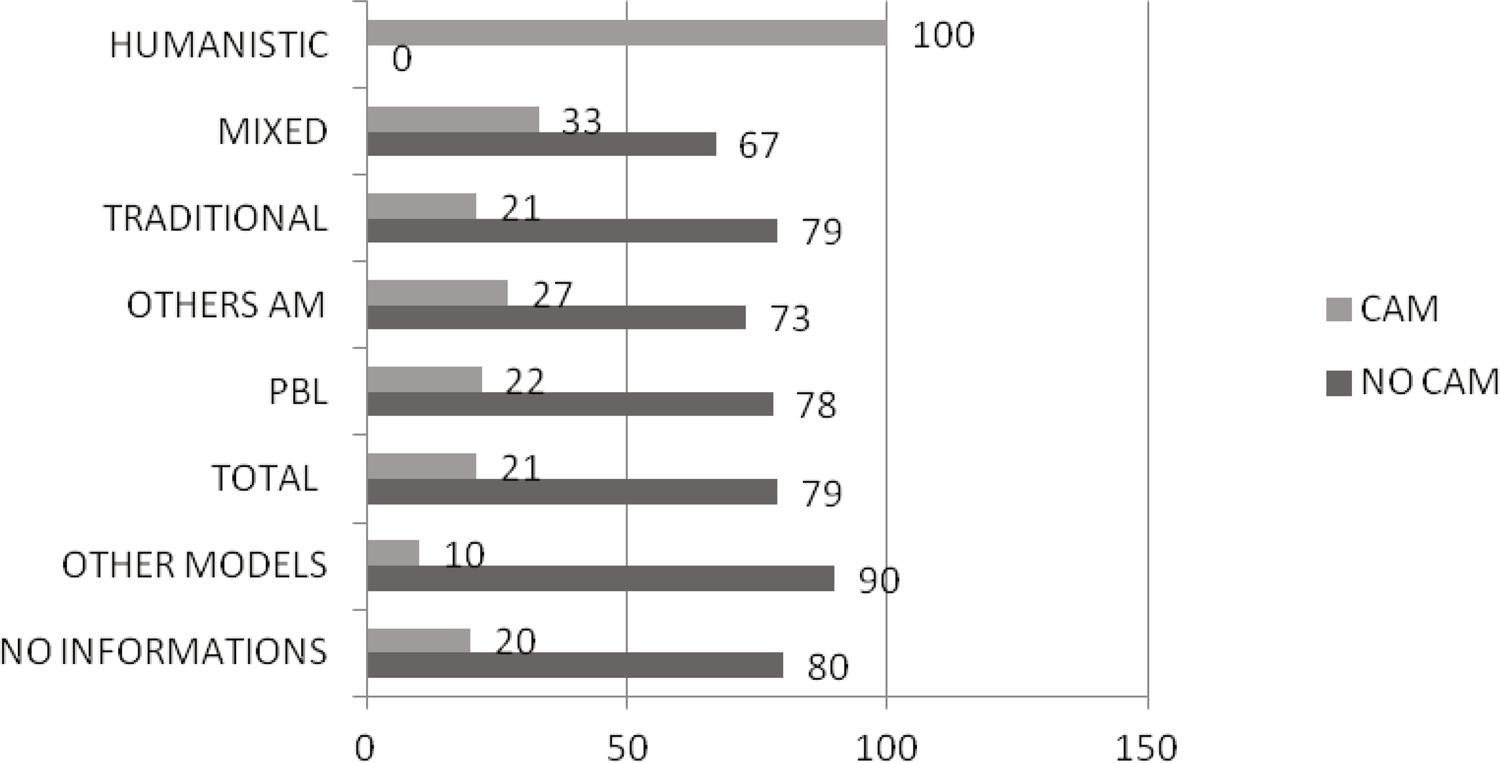
PBL: Problem Based Learning; AM: Active Methodologies; CAM: Complementary and Alternative Medicine.
Source: Data prepared by the author.
Figure 1 Percentage of CAM and theaching-leargin methodologies in Brazilian medicine schools (2016)
As for the teaching of CAM in its various forms of practice and rationalities, most schools adopt a single model of practice and there is a prevalence of homeopathy and acupuncture teaching, followed by integrative medicine and phytotherapy ( Figure 2 ).
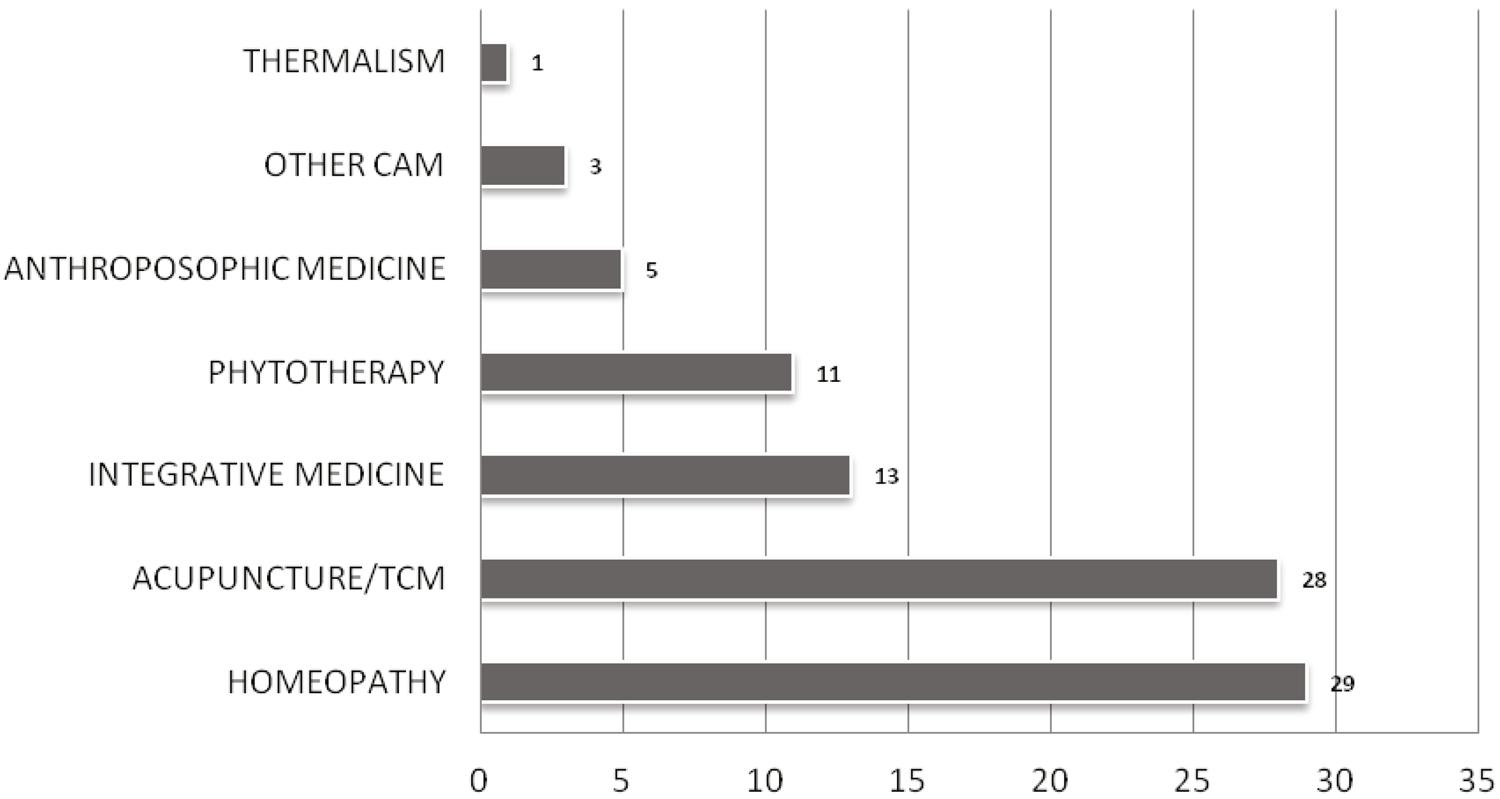
TCM: Traditional Chinese Medicine
CAM: Complementary and Alternative Medicine
Source: Census survey 2016 (data prepared by the author).
Figure 2 Types of CAM in medical schools in Brazil (2016)
There is a predominance of teaching in CAM in non-compulsory modules or curricular subjects. Non-compulsory curricular activities developed are optional modules and/or optional disciplines, study groups and extension projects are among the most cited.
DISCUSSION
This study showed that medical schools are not homogeneously distributed in the five regions of Brazil. There has been growth in recent years, especially in the Northeast region, where the number of schools has tripled, but this has not been enough to overcome the inequality. This disproportion is even greater when considering the relation between the number of available places in schools with population of each region. The North and Northeast regions have the lowest number of places per inhabitant. On the other hand, the South and Midwest have fewer inhabitants per medical school and, therefore, a higher percentage of schools in relation to the percentage of the national population. The number of available places is also disproportionate and poorly distributed throughout the regions of the country. When observing some cities in the Midwest, such as the Federal District, a greater ratio of doctors per inhabitant was found, whereas in innerstate cities in the North and Northeast there is a lack of doctors [ 14 ]. It was also found that there has been a growth of medical schools since 2012, which includes the process of internalization, in keeping with previous research [ 15 ], which may in the future result in a greater balance in the proportion of doctors per capita.
The study also showed that there are currently 272 medical schools in Brazil and, of those, 57 (21%) which include teaching of CAM. In 2006, there were only 155 medical schools in the country and 36 (23.2%) which included CAM teaching, which differs from a previous study [ 16 ] and data obtained according to the year the school was founded. There has been a noteworthy growth in the number of medical schools since introduction of the National Curricular Guidelines (37% until 2006). Since 2006, this growth has been more evident (reaching 75%). There is, however, a gap between the increase in medical schools and the teaching of CAM, since the growth was only 2.7 schools/year for schools teaching CAM, while the growth of medical schools in general was 11.7 schools/year over the last ten years [16; 17]. This means that, although the number of medical schools has tripled, ICP teaching has not kept up with the educational landscape, with reduced content in relation to the number of schools in the 1970s ( Figure 2 ).
Teaching in CAM has not shown significant growth even in the Northeast since the implementation of the NPICP. In the 1960s, 39 new medical schools were founded according to data from the National Institute of Education and Research (NIER) [ 14 ], of which nine schools (23%) had CAM in the curriculum. As of 2006, 23 new medical schools adopted teaching of CAM corresponding to 40% of the current total. However, 60% of schools with CAM already existed, showing that the implementation of the NPICP in 2006 did not have an impact on the teaching of CAM at undergraduate level; it equally had no impact on the SUS, as previous studies have shown [ 18 ]. In a 2014 study, Salles, Homo and Silva showed that public schools were more numerous in the Northeast and were considering the WHO orientation to prioritize the teaching of TM/CAM in the poorest regions of its member countries. Confirming Scheffer’s studies [14; 15], most medical schools in Brazil are currently managed privately (approximately 46% are public). However, in relation to CAM education, public schools remain prevalent.
Since 2001, medical teaching has undergone modifications regarding the teaching-learning methodologies used and has been progressively adapting to the National Curricular Guidelines (NCG), implemented in 2001 and revised in 2014, which explains the predominance of active methodologies. However, the teaching of CAM does not seem to depend on the methodology, although the growth of schools with PBL/AM has increased proportionally in relation to the growth of schools with other methodologies. In relation to the new approaches and teaching methodologies that have been advocated, there are twice as many schools with PBL teaching in the Northeast than traditional schools or schools with mixed methodologies. This is probably due to the expansion of medical teaching centers since the NCG, prioritizing this region in the country. However, the number of schools with CAM is similar in both models. Most approaches to CAM in the Northeast are traditional medicines and practices such as Acupuncture and Homeopathy, then Integrative Medicine and Phytotherapy. In the Southeast, the teaching of Homeopathy predominates, followed by Integrative Medicine and then Acupuncture. It is difficult to find Phytotherapy training in this region, perhaps because of the historical colonial influence that brought over French Medicine in the early nineteenth century, with a focus on Homeopathy [19; 20] and only after the immigration of the Eastern populations [ 21 ] (SMBA, 2015). Anthroposophic Medicine became part of the group of medical rationalities adopted in 2006, and is increasing offered in the health care system [ 22 ]. There has been a growth of around 240% in the number of medical schools in the country if the 2006 and 2016 data is considered [ 16 ], and there is still a need for professionals. We have an index of 2.1 doctors per 1000 inhabitants, which is considered low according to CFM data [ 14 ]. This profile can be modified if there is a better distribution of available places in the capital and the interior of the states. There was an increase in the medical population between 2013 and 2015, and this was probably due to the new schools that already had their first graduate medics.
The growing emergence of medical schools and the lack of growth in CAM teaching demonstrated in this research confirms the fact that, while the number of medical schools has almost tripled in Brazil since 2006, even with the official implementation of CAM in the SUS through the NPICP, growth has become less pronounced. Moreover, the motivation to learn presumes involvement of mental processes that are not directly observable. It is often necessary to involve interactions between an individual and a social context [ 23 ], so it is not an individual phenomenon. Introducing CAM into the medical school curriculum requires a dedicated team to cause a significant change [ 24 ]. For the medical student interest in CAM depends on its inclusion in the curriculum learning context. This context needs to be modified, by encouraging this curricular content in pedagogical projects, contributing to the process of humanization in health [13; 23; 24; 25] and following the principles of the National Curricular Guidelines, with respect to receptive listening; development of therapeutic connection; integration of the human being with the environment and society; an expanded view of the health-disease process; global promotion of human care and self-care; and the necessary opening for new knowledge or there will be no growth or worse, there will be a stagnation of teaching of Integrative Practices in Brazilian Medical Schools [1;11;12;25]. The implementation of National Curricular Guidelines in 2001, should have contributed to the growth of schools and the teaching of CAM, however this failed to materialize.
CONCLUSION
The conclusion can be drawn that the number of medical schools almost tripled after 1970, but there was no increase in CAM teaching in these schools, in fact there was a reduction in their implementation in the national scenario. The NPICP failed to impact on the growth of teaching CAM, which was also the case in relation to the SUS. In the two decades previous to the National Curricular Guidelines being implemented, there was a greater increase in CAM in medical education than in the following period, which is contrary to what the WHO advocated, recommending the preparation of new professionals qualified to work with CAM mainly in Primary Health Care (PHC). Ten years after the creation of the NPICP and after more than two decades of the formalization of Homeopathy and Acupuncture as medical specialties there is still no teaching systematization of CAM in Brazilian medical schools. There is a need to conform to the new National Guidelines for Medical Education and the WHO recommendations to train new human resources to support an integrated and humanized medical practice. This should be the role of CAM in education and health, provided that strategies for effective implementation and syllabus standardization are considered and adopted by the administrators of medical schools in Brazil, in partnership with the Ministries of Education and Health.

