











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Emotional intelligence (EI) is a much-debated topic, not only in medicine and healthcare. It can be defined as the ability to accurately perceive, evaluate and express emotions; the ability to perceive and/or generate feelings when they facilitate thought; the ability to understand emotion and emotional knowledge; and the ability to control emotions to promote emotional and intellectual growth1. It is a social skill and can be taught, trained or improved2.
Several studies have shown the direct effects of EI on medical practice and, more specifically, on establishing and maintaining a good doctor-patient relationship3. Canales and Cleveland discussed the importance of a medical professional’s ability to understand and manage emotions, feelings and behaviors. Their analysis revealed that this skill is developed automatically during ongoing work with and care of patients. Nonetheless, they concluded that curricular changes in medical schools would provide doctors-in-training with greater aptitude in relation to skills involving EI4.
Hernandez-Vargas and Dickinson-Bannack claimed that EI is an essential skill in medical practice5. It assists the doctor-patient relationship, positively affects quality of care and patient satisfaction, improves doctor performance, level of involvement and job satisfaction and facilitates the development of communication skills3), (5.
In a literature review, Johnson established that the ability to evaluate a patient’s emotions improved information collection and diagnostic accuracy. The author highlighted that strategies to train, develop, test and evaluate medical students’ emotional skills must be addressed in a longitudinal and comprehensive way throughout medical school. The goal is not just to establish but also to facilitate the incorporation of these concepts and skills6.
Another recent study that evaluated the effect of EI on medical students’ performance in surgical activities showed that the ability to support and respond well to workplace and occupational stress was linked to students’ or doctors’ EI levels. The results suggested the need of training the cognitive area, which includes these skills, so students could develop better work-related stress coping mechanisms7.
Therefore, improving doctors’ and medical students’ EI can be considered a possible solution for mitigating the deleterious effects caused by the complexity of a doctor’s relationship with the work environment, as well as his/her intrapersonal and interpersonal relationships. This skill can be taught and improved, and the effects of its inclusion in medical school curricula should be systematically evaluated3), (5.
There are few articles on EI and medical education in Brazil. An instrument to evaluate EI levels8 has only recently been validated for Brazilian Portuguese, and our literature review did not identify any studies that have evaluated EI levels in Brazilian medical students. The main objectives of this study were therefore to compare the EI levels of students from different years of medical school and to identify factors that affected these levels.
MATERIALS AND METHODS
Study design and population
This was a cross-sectional study that evaluated students in the 1st, 3rd and 6th years of a private medical school at the Universidade José do Rosário Vellano (UINFENAS), Belo Horizonte Campus, in the years 2017 and 2018. The University has its own admission process. In Brazil, the medical program structure is different from that in the United States and other European countries, as the preclinical and clinical years comprise a single program with a total length of 6 year.
The sample size was calculated as 177 volunteers, 59 from each year, according to StatCalc EpiInfo® (CDC, USA) for cross-sectional studies, based on a total population of 450 medical students (150 students from each year), a 25.0% expected frequency of high EI levels, margin of error of 5% and a 95% confidence interval. Considering possible losses and incomplete questionnaires, the sample size was increased by 10%, up to 195 volunteers, 65 from each year of medical school. Recruitment was done by convenience. All students from each of the three years were invited to participate. In all cases, the researchers oversaw questionnaire completion, but without interfering in the process. All volunteers signed the free and informed consent form prior to inclusion in the study.
Procedures
The main study outcome was the EI level, and secondary outcomes were EI levels within different domains. Outcomes were measured using the version of the Schutte Self-Report EI Test (SSEIT) that has been validated to be used in Brazil8), (9. The SSEIT is a self-administered questionnaire with 33 items, divided into four domains: Perception of Emotions, Managing Own Emotions, Managing Others’ Emotions, and Utilization of Emotions. The items use a Likert scale with five response options: (1) strongly disagree, (2) partially disagree, (3) neither disagree, nor agree, (4) partially agree and (5) strongly agree. When calculating the final score, the response values of items 5, 28 and 33 must be inverted before summing up all response values. The score for each of the four domains is calculated by adding the corresponding items: Perception of Emotion (items 5, 9, 15, 18, 19, 22, 25, 29, 32, 33), Managing Own Emotions (items 2, 3, 10, 12, 14, 21, 23, 28, 31), Managing Others’ Emotions (items 1, 4, 11, 13, 16, 24, 26, 30) and Utilization of Emotions (items 6, 7, 8, 17, 20, 27). The total score ranges from 33-165. Higher scores indicate higher levels of EI 8,9. The main exposure variable was the medical school year, divided into three groups: 1st, 3rd and 6th years. The following variables were also collected: gender, age, marital status, children (yes/no), religion, previous undergraduate course, participation in extracurricular activities and self-reported previous mental disorder diagnosis. Mental disorder was evaluated through two questions. A yes or no question: “Have you ever had a confirmed diagnosis of depression or other mental disorders (except epilepsy)”, and an open one: “What was the diagnosis?”. The second question was considered only when the answer to the first one was “yes”.
Statistical analysis
In the descriptive analysis, the mean and standard deviation were used for continuous variables, and frequency distribution was used for categorical variables. ANOVA was used to compare EI scores among school years, and Student’s t-test was used to compare EI and gender, marital status (single or not), religion, previous undergraduate course, participation in extracurricular activities and previous mental disorder diagnosis. The two-tailed Fisher’s exact test was used to compare gender and previous mental disorder diagnosis. Pearson’s correlation test was used to evaluate the association between age and EI score. Multiple regression analysis was performed for the total EI score and its domains in relation to the variables with p values <0.10. A significance level of 0.05 was adopted. IBM® SPSS® Statistics software v. 19 (IBM, USA) was used for the statistical analysis.
Ethical aspects
This study was approved by Institutional Ethics Committee (Opinion N. 2.048.558) and is in accordance with the current version of the Declaration of Helsinki and Resolution 466/2012 of CONEP and its updates. All volunteers received clarification on the study objectives and signed the free and informed consent form before inclusion.
RESULTS
Between October 2017 and April 2018, 225 volunteers were recruited. Of these, 16 (7.1%) were excluded due to incomplete questionnaires. The final sample comprised 209 participants, 71 from the 1st year, 69 from the 3rd year and 69 from the 6th year of medical school.
Table 1 shows the demographic and personal characteristics of the 209 volunteers according to the course year. A predominance of females (138 - 66.0%) and single individuals (199 - 95.2%) was observed. Only four volunteers (1.9%) had children, and 19 (9.1%) declared having no religion. Twenty-one (10.0%) had previous degrees, and 128 (61.2%) reported participating in extracurricular activities. The frequency of previous depression or another mental disorder diagnosis was 16.3% (34 volunteers). The mean overall age was 23.2 (± 3.9) years.
Table 1 Personal and demographic characteristics of the 209 volunteers according to the medical course year
| Variable | 1st year | 3rd year | 6th year | Total | |||||
| N | % | n | % | n | % | n | % | ||
| Gender | Female | 46 | 64.8 | 45 | 65.2 | 47 | 68.1 | 138 | 66.0 |
| Male | 25 | 35.2 | 24 | 34.8 | 22 | 31.9 | 71 | 34.0 | |
| Marital status | Single | 67 | 94.4 | 66 | 95.7 | 66 | 95.7 | 199 | 95.2 |
| Married | 4 | 5.6 | 2 | 2.9 | 2 | 2.9 | 8 | 3.8 | |
| Other | 0 | 0.0 | 1 | 1.4 | 1 | 1.4 | 2 | 1.0 | |
| Children | Yes | 1 | 1.4 | 2 | 2.9 | 1 | 1.4 | 4 | 1.9 |
| No | 69 | 98.6 | 67 | 97.1 | 68 | 98.6 | 204 | 98.1 | |
| Religion | Yes | 64 | 90.1 | 62 | 89.9 | 64 | 92.8 | 190 | 90.9 |
| No | 7 | 9.9 | 7 | 10.1 | 5 | 7.2 | 19 | 9.1 | |
| Previous degree | Yes | 6 | 8.5 | 6 | 8.7 | 9 | 13.0 | 21 | 10.0 |
| No | 65 | 91.5 | 63 | 91.3 | 60 | 87.0 | 188 | 90.0 | |
| Extracurricular activities | Yes | 17 | 23.9 | 62 | 89.9 | 49 | 71.0 | 128 | 61.2 |
| No | 54 | 76.1 | 7 | 10.1 | 20 | 29.0 | 81 | 38.8 | |
| Previous mental disorder | Yes | 13 | 18.3 | 8 | 11.6 | 13 | 18.8 | 34 | 16.3 |
| No | 58 | 81.7 | 61 | 88.4 | 56 | 81.2 | 175 | 83.7 | |
| Age | Mean (SD) | 21.0 (3.76) | 23.0 (3.21) | 25.8 (3.11) | 23.2 (3.90) | ||||
SD - standard deviation Source: prepared by the authors
Of the 21 participants with a previous degree, 17 (85.0%) had graduated in the health area, with the most frequent degree being nursing (7 - 35.0%), followed by physiotherapy and pharmacy, both with three participants (15.0%) each. Some of the 34 volunteers with previous mental disorders reported more than one diagnosis, totaling 41 diagnoses. The most frequent ones were depression (21 - 51.2%) and anxiety-related disorders (18 - 44.0%).
Table 2 shows EI total score and its domains according to the medical course year. None of these differences were statistically significant. All scores could be considered high, as they reach at least 75.0% of the maximum score.
Table 2 Total emotional intelligence score and its domains scores for 209 volunteers according to the medical course year
| Variable | 1st year | 3rd year | 6th year | Total | p* | ||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Total score | 127.9 | 13.7 | 127.6 | 13.1 | 131.2 | 12.4 | 128.9 | 13.1 | 0.208 |
| Perception of emotion | 36.5 | 5.3 | 36.3 | 5.3 | 38.0 | 5.4 | 36.9 | 5.4 | 0.115 |
| Managing Own Emotions | 36.3 | 5.3 | 36.7 | 4.0 | 37.6 | 4.1 | 36.9 | 4.6 | 0.212 |
| Managing Others’ Emotions | 30.5 | 4.1 | 30.7 | 4.3 | 31.6 | 4.0 | 30.9 | 4.1 | 0.223 |
| Utilization of emotions | 24.6 | 3.6 | 23.9 | 3.9 | 23.9 | 3.5 | 24.6 | 3.7 | 0.412 |
SD - standard deviation; *ANOVA Source: prepared by the authors
Table 3 shows the variables with a statistically significant difference regarding total EI score and its domains, except for age. There were no significant differences between EI score and having a religion or participating in extracurricular activities. Men had a statistically higher score than women for the Managing Own Emotions domain, 38.0 ± 4.3 versus 36.3 ± 4.6 (p = 0.013), respectively. Students with a previous degree also showed higher scores in the Perception of Emotion domain, 39.5 ± 4.7 versus 36.7 ± 5.4 (p = 0.021), respectively. Volunteers who reported a previous mental disorder had a lower total EI score (124.6 ± 13.2 versus 129.7 ± 13.0, p = 0.036) and a lower score in the Managing Own Emotions domain (33.7 ± 4.1 versus 37.5 ± 5.5, p < 0.001).
Table 3 Total scores for Emotional Intelligence and its domains among 209 volunteers according to gender, previous degree and self-reported previous mental disorder
| Gender | Female | Male | p* | ||
| Mean | SD | Mean | SD | ||
| Total score | 128.0 | 12.9 | 130.5 | 13.6 | 0.200 |
| Perception of Emotion | 36.7 | 5.2 | 37.3 | 5.8 | 0.451 |
| Managing Own Emotions | 36.3 | 4.6 | 38.0 | 4.3 | 0.013 |
| Managing Others’ Emotions | 31.0 | 4.0 | 30.7 | 4.4 | 0.608 |
| Utilization of Emotions | 24.0 | 3.8 | 24.5 | 3.4 | 0.331 |
| Previous degree | No | Yes | p* | ||
| Mean | SD | Mean | SD | ||
| Total score | 128.4 | 13.3 | 133.1 | 10.5 | 0.120 |
| Perception of Emotion | 36.7 | 5.4 | 39.5 | 4.7 | 0.021 |
| Managing Own Emotions | 36.8 | 4.7 | 37.9 | 3.3 | 0.272 |
| Managing Others’ Emotions | 30.9 | 4.2 | 31.0 | 3.9 | 0.929 |
| Utilization of Emotions | 24.1 | 3.7 | 24.7 | 3.2 | 0.457 |
| Self-report of previous mental disorder | No | Yes | p* | ||
| Mean | SD | Mean | SD | ||
| Total score | 129.7 | 13.0 | 124.6 | 13.2 | 0.036 |
| Perception of Emotion | 36.9 | 5.3 | 37.4 | 5.9 | 0.594 |
| Managing Own Emotions | 37.5 | 4.1 | 33.7 | 5.5 | < 0.001 |
| Managing Others’ Emotions | 31.2 | 4.2 | 29.7 | 3.6 | 0.054 |
| Utilization of Emotions | 24.2 | 3.7 | 23.8 | 3.3 | 0.539 |
SD - standard deviation; * Student’s t-test Source: prepared by the authors
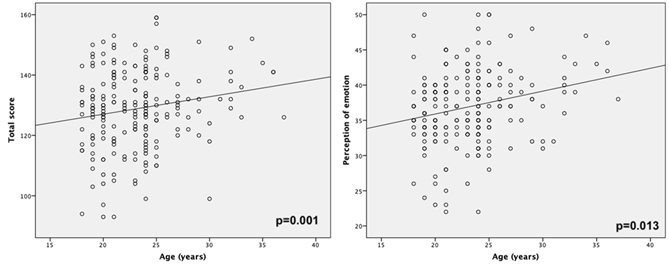
Pearson’s correlation showed a weak but statistically significant positive association between age, total EI score and Perception of Emotion domain (Figure 1). The other domains were not statistically significant.
Considering that the volunteers with a previous degree were older than those without one (30.8 ± 5.1 years versus 22.3 ± 2.8 years; p <0.001) and that the reporting of a previous mental disorder was significantly higher among women than among men (21.1% versus 5.6%; p = 0.003, RR = 1.43 - 95% CI 1.21 - 1.70), it was decided to include these four variables in the multiple regression analysis, regardless of their crude p value. According to Table 4, it was observed that age increase positively affected the total score (padjusted = 0.040), Perception of Emotion (padjusted = 0.013) and Managing Others’ Emotions (padjusted = 0.020). Self-report of a previous mental disorder negatively affected the total EI score (padjusted = 0.033) and the scores for Managing Own Emotions (padjusted = <0.001) and Managing Others’ Emotions (padjusted = 0.025). The multiple regression analysis revealed no association between gender, previous degree and EI levels.
Table 4 Multiple regression of age, gender, previous graduation, and self-reported previous mental disorder and emotional intelligence scores
| Variable | Non-standardized coefficients | pcrude | padjusted | |
| Total score | beta | standard error | ||
| Age | 0.626 | 0.302 | 0.013 | 0.040 |
| Gender | 1.595 | 1.921 | 0.200 | 0.407 |
| Previous degree | -0.069 | 3.912 | 0.120 | 0.986 |
| Previous mental disorder | -5.306 | 2.472 | 0.036 | 0.033 |
| Perception of Emotion | beta | standard error | pcrude | padjusted |
| Age | 0.311 | 0.124 | 0.001 | 0.013 |
| Gender | 0.660 | 0.784 | 0.451 | 0.401 |
| Previous degree | 0.200 | 1.598 | 0.021 | 0.901 |
| Previous mental disorder | 0.411 | 1.009 | 0.594 | 0.684 |
| Managing Own Emotions | beta | standard error | pcrude | padjusted |
| Age | 0.177 | 0.101 | 0.068 | 0.082 |
| Gender | 1.063 | 0.642 | 0.013 | 0.099 |
| Previous degree | 0.029 | 1.308 | 0.272 | 0.983 |
| Previous mental disorder | -3.658 | 0.826 | < 0.001 | <0.001 |
| Managing Others’ Emotions | beta | standard error | pcrude | padjusted |
| Age | 0.225 | 0.096 | 0.092 | 0.020 |
| Gender | -0.640 | 0.609 | 0.608 | 0.295 |
| Previous degree | -1.708 | 1.241 | 0.929 | 0.170 |
| Previous mental disorder | -1.773 | 0.784 | 0.054 | 0.025 |
| Utilization of emotions | beta | standard error | pcrude | padjusted |
| Age | -0.086 | 0.087 | 0.795 | 0.322 |
| Gender | 0.511 | 0.550 | 0.331 | 0.354 |
| Previous degree | 1.411 | 1.119 | 0.457 | 0.209 |
| Previous mental disorder | -0.286 | 0.707 | 0.539 | 0.686 |
Source: prepared by the authors
DISCUSSION
The objectives of this study were to compare the EI levels among students at three different years of medical school and to evaluate the factors associated with EI. Overall, there was no difference in total EI score, nor in its domain scores among the three groups. The observed scores were high, with 6th year students having slightly higher values than the other two groups, but with no significant difference. The 1st year students’ scores were higher than expected, suggesting that the sample was possibly underestimated and did not have sufficient statistical power to indicate whether there were really any differences between the groups. The initial analysis showed differences between EI levels and a previous degree, gender and self-reported mental disorders. There was also a positive weak correlation, but statistically significant, between age and EI.
The results of this study suggest that a previous degree might be associated with higher levels of EI, especially with regard to the Perception of Emotion domain. However, age could be a confounding factor in this association, as the students with a previous degree were older than those who were working toward their first degree (30.8 ± 5.1 years versus 22.3 ± 2.8 years; p < 0.001). The multivariate analysis showed that in the population studied, the true association was found between EI levels and age, rather than a previous degree. Several studies support this association. Fariselli, Ghini and Freedman showed that for most people, EI levels improve over time and through life experience10. More specifically, regarding age, Cabello et al. found an inverted “U” pattern in the association between age and EI levels measured by two different tests, demonstrating that younger (< 31 years) and older volunteers (> 45 years) can have lower EI levels than adults of middle age (32 to 44 years)11. In a study conducted in 2017, Sharma observed similar findings, which indicated that total EI score increases with age but that skill and sensitivity are greater between 24 and 34 years of age12. Further exploring this association with age, Atkins and Stough observed that the ability to use emotions to solve problems increases with age, while the ability to control strong emotions can decrease with age13.
The bivariate analysis revealed an association between gender and EI; however, this association was ruled out by the multivariate analysis. Nevertheless, it is important to discuss the association between gender and EI, as the initial results of this study indicated that men had higher scores than women in the Managing Own Emotions domain (38.0 ± 4.3 versus 36.3 ± 4.6; p = 0.013). This finding is contrary to that in the literature, which shows that higher EI levels are usually observed in women14-16. The effect of gender on EI levels has been the subject of intense discussion in recent years, as different studies support the hypothesis that women have a tendency to have higher EI levels than men, while others refute this hypothesis, demonstrating that this association may be due to methodological bias17)-(20.
In a study that evaluated 177 medical students, Carr observed higher EI levels (total score and its domains) in men21. In a cross-sectional study also carried out with medical students from different years, Vasefi, Dehghani and Mirzaaghapoor found no statistically significant difference in scores between genders. The authors suggest that even if women really have higher EI levels, they would be more susceptible to greater “emotional exhaustion” from everyday life difficulties, which would lead to a decrease in EI assessment test scores and a consequent reduction in significance when the two genders’ scores are compared22.
A possible explanation for the lack of an association between gender and EI in this study is the higher frequency of previous mental disorders in women (21.7% versus 5.6%; p = 0.003), as mental disorders are known to have a negative effect on EI and its domains23)-(28.
Although the frequency of previous mental disorders observed in the study is almost half the frequency of recent reports in the international and national literature, at 16.3% compared to 27.2%29 and 31.4%30, respectively, the multivariate analysis showed a negative association between reported mental disorders and total EI score (p = 0.033), as well as lower scores for the Managing Own Emotions (p <0.001) and Managing Others’ Emotions (p = 0.025) domains.
Hertel, Schütz and Lammers concluded that individuals with major depressive, borderline personality and substance abuse disorders have significant deficits in EI assessment test scores when compared to those without mental disorders25. In addition, the authors also indicated that this difference was even more significant when evaluating skills involved in the Perception of others’ emotions and Managing own emotions25. Moreover, Downey et al. concluded that EI levels measured by testing may be predictive of the early identification of individuals at risk for major depression31.
Fernandez-Berrocal, Alcaide and Extremera also demonstrated that anxiety and depression negatively correlate to EI levels32. In addition, this study also found that the ability to discriminate feelings and manage own emotions are skills associated with better psychological adjustment, regardless of the effects of self-esteem and thought suppression on these test scores32. Holt and Jones describe how the inability to regulate anxiety can affect an individual’s performance on EI evaluation tests and that would lead to lower scores on these tests due to these individuals’ greater distraction from the tasks in which they are involved33.
In addition to depression and anxiety, other mental and behavioral disorders are strongly correlated to lower EI levels. Khoshakhlagh and Faramarzi reported a statistically significant association between EI, mental disorders and internet addiction. They concluded that mental disorders such as anxiety, obsessive-compulsive disorder, aggression, phobias and hypochondria are good predictors of internet addiction and are closely related to lower EI levels when they are measured in tests34. These reports support this study’s observations.
One limitation of this study is inherent to the instrument used for EI level assessment. Self-report instruments have a tendency to overestimate EI levels, as respondents may offer the response that they consider socially acceptable, rather than an honest evaluation of their situation35)-(38. The alternative to this would be the use of performance instruments, requiring the individual observation of volunteers in a real or simulated environment, which is operationally infeasible for large-scale studies38), (39. Despite the possibility of an overestimation of scores, the values observed in this study are similar to those in other studies of university students in other countries8), (35), (40)-(47. Another limitation is related to the cross-sectional design, which evaluated different groups of people in different years of the course. The ideal design to evaluate the variation in EI levels over the course would be a cohort. However, this would entail a long, expensive and operationally complex study, as participants would have to be followed for at least 6 years. Other limitations are the fact that it is a single-center study and the absence of the assessment of specific mental disorders.
Despite these limitations, to the best of our knowledge, this is the first study to evaluate EI levels among medical students in Brazil and one of the very few in international literature that correlated mental disorders with low EI levels among medical students, which makes it unique. Moreover, it includes a suitable number of volunteers, and the observed associations showed high significance, which indicates the chance that the observations are true. This study can be used as a reference for future studies on EI in medical students and those on other courses in the health area. Some findings, such as the association between gender and age and the behavior of EI levels throughout the course need to be evaluated by further studies. Moreover, when considering EI as a skill, one must also evaluate the possibility of performing experimental studies that evaluate the effects of training of these skills on medical students.

