











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Cardiovascular diseases represent the main cause of death worldwide: more people die annually from these diseases than from any other cause. It is estimated that 17.7 million people died from cardiovascular diseases in 2015, representing 31% of all deaths at global level1. Among the main causes of Cardiorespiratory Arrest (CRA) are acute myocardial infarction, coronary heart disease and cardiac arrhythmias. In Brazil, between 2004 and 2014, 8.8% of deaths were due to myocardial infarction, angina and other ischemic heart diseases2.
External causes, such as traffic accidents, stab wounds or firearm injuries and airway obstruction by foreign bodies are also factors that can lead to CRA. They represent the second leading cause of death in Brazil in general terms, and the most important cause in the age group ranging from 1 to 49 years3. In the country, it is estimated that in 2019 more than 140,000 deaths occurred due to external causes4.
Basic Life Support (BLS) refers to the procedures that healthcare professionals must perform on patients in situations of CRA or airway obstruction. Cardiopulmonary resuscitation (CPR) is at the core of the BLS and consists in the set of performed maneuvers aiming at artificially maintaining arterial flow to the brain and other vital organs, until the spontaneous circulation resumes5.
CPR success depends on theoretical knowledge and also on psychomotor skills by the professionals who perform it, such as using the automated external defibrillator (AED) or adopting actions to clear the airway, among other possible measures6. The time factor is a determining variable, considering that any delay in treatment can result in sequelae and have an impact on patient survival7. Therefore, the training of health professionals in immediate and standardized care for this clinical situation can have favorable prognostic implications8.
Undergraduate courses in the health area are beneficial environments for the training of human resources prepared to deal with BLS. However, studies have shown a low level of knowledge about BLS in analyses by students from specific courses, such as Medicine9 or Nursing10, or in the comparative analysis between several courses in the health field11),(12. The low level of knowledge has been associated mainly with the lack of prior BLS training among students9),(12, and among professionals with little clinical experience13),(14. Most of the studies have as their target-populations students from different periods9),(12),(15, interns11 or professionals13),(14),(16),(17, and little emphasis has been placed on the undergraduate students from different courses in the health area. In this context, the present study aimed to determine the level of knowledge about BLS and the associated factors in undergraduate students attending health courses in a public university.
MATERIAL AND METHOD
Design and ethical aspects
This research was a cross-sectional study with a quantitative approach, carried out with undergraduate students from health courses (Physical Education, Nursing, Pharmacy, Medicine and Dentistry) at Universidade Estadual de Ponta Grossa (UEPG), Paraná, Brazil. The study was previously approved by the Research Ethics Committee of UEPG, with the protocol of the Certificate of Presentation for Ethical Appreciation (CAAE) number 03813818.0.0000.0105.
Study universe
The study was carried out with undergraduate students from courses in the health area in 2019. The University has an yearly entry system for all evaluated courses, with the Medicine course ending in August and the remaining courses in December 2019.
The study universe was made available by the Undergraduate Students’ Dean’s Office, distributed as follows: Bachelor of Physical Education (n = 44), Nursing (n = 35), Pharmacy (n = 41), Medicine (n = 46) and Dentistry (n = 57), totaling 223 eligible undergraduate students.
The inclusion criteria for the study were: being able to complete the health course in 2019; and agree to sign the Free and Informed Consent Form (ICF). The exclusion criteria were: having some unfinished discipline that would prevent the student from completing the course in 2019; students who took a break from College or dropped out of the course; or did not accept to participate in the study.
The bachelor’s degree in Physical Education course at UEPG started in 2010, and the first version of the Political-Pedagogical Project of the Course (PPC) is still used. The course lasts four years until course completion, with a minimum of 3,419 (three thousand, four hundred and nineteen) hours. The Nursing course at UEPG started in 2007. The fourth version of its PPC has been used since 2014, with five years until course completion, and a minimum of 4,800 (four thousand and eight hundred) hours. The bachelor’s degree in Pharmacy at UEPG started in 1956, and the fifth version of its PPC has been used since 2005. The course lasts five years until course completion, with a minimum of 5,028 (five thousand and twenty-eight) hours. The Bachelor’s Degree in Medicine at UEPG started in 2009. The PPC is in its second version and has been active since 2011. The course duration comprises a period of six years, with a minimum total of 8,258 (eight thousand, two hundred and fifty-eight) hours. The bachelor’s degree in Dentistry at UEPG started in 1956 and the evaluated class was using the tenth version of the PPC, implemented in 2005. The PPC has a minimum total of 5,164 (five thousand one hundred and sixty-four) hours.
The offer of a specific discipline that addresses the topic of Basic Life Support (BLS), it is described in the syllabus of disciplines of the courses of Physical Education, Nursing and Medicine. In the Physical Education course, there is a mandatory discipline called Hygiene Notions and Emergency Aid in Physical Education and Sports aimed at the specific professional training, with a 68-hour semester workload and a theoretical basis, and a semiannual offer in the first semester of the second academic year. In Nursing, there is a mandatory discipline of Emergency Nursing, aimed at the specific professional training of the course, with a workload of 68 hours, with a theoretical-practical basis, and a semiannual offer in the first semester of the fourth academic year. In the Medicine course, there are the disciplines of Internship in Surgical Urgency and Emergency and Internship in Clinical Urgency and Emergency, in the 5th curricular year, which is mandatory, with a workload of 420 hours each and a theoretical-practical approach.
Data collection
Data collection was carried out at the institution itself, through a self-administered questionnaire at the end of the course completion, carried out in July 2019 for the Medicine course, and November and December 2019 for the Physical Education, Nursing, Pharmacy, and Dentistry courses. The tool was organized into two parts: the first included sociodemographic data, professional training, and perceived self-knowledge18, and the second part assessed the level of knowledge using an instrument validated in previous research12, containing 20 multiple-choice questions, each containing four answer choices.
Variables
The study outcome was the undergraduate students’ level of knowledge, dichotomized according to the number of correct answers in 14 (70%) of the 20 questions answered in the questionnaire: high (greater or equal than 70% of correct answers) or low (<70% of correct answers) level of knowledge about BLS. This cutoff was adopted considering the average grade for approval in the disciplines by the University. Although the calculation was based on the correct answers, we chose not to exclude the unanswered questions from the analysis and the latter were classified as ‘not correct’.
The independent variables were divided as follows:
Sociodemographic variables: sex (woman and man) and age (up to 24 years and 25 years or older).
Professional training: undergraduate course (Physical Education, Nursing, Pharmacy, Medicine and Dentistry) and training for BLS (no and yes).
Course duration in hours: more than 40h (no and yes) or more than 100 hours (no and yes), offer of a specific discipline in BLS/emergencies during undergraduate school (no and yes), completion of the discipline (no and yes), modality of the offered discipline (optional or mandatory), discipline approach (theoretical and theoretical-practical/practical) and believing that the offered discipline was sufficient (no and yes).
Perceived self-knowledge: feeling confident (no/some situations and yes) and believing in the need to take courses (no and yes).
Data analysis
The data obtained were stored in a Microsoft Office Excel spreadsheet, and subsequently analyzed using the Statistical Package for the Social Science (SPSS) version 20.0 (IBM Corp., NY, United States). Descriptive statistics was performed using absolute (n) and relative (%) frequencies. For the association between the study outcome (high and low knowledge) and the independent variables (sociodemographic data, professional training and perceived self-knowledge), Fisher’s exact test or the Chi-square test was used (p <0.05). The regression was performed using a binary logistic model (crude) and multinomial logistic model (adjusted) (p <0.05), which used ‘high knowledge’ as the reference category.
RESULTS
The study was carried out with 191 undergraduate students, totaling 85.6% of the chosen universe that met the eligibility criteria, with a proportion of participation per course of 37 undergraduate students from the Physical Education course (84.1%), 34 from Nursing (97.1%), 33 from Pharmacy (80.5%), 39 from Medicine (84.8%) and 48 from Dentistry (84.2%) (Table 1).
Chart 1 shows that the highest proportion of correct answers was 40% (11.5%) of the BLS questionnaire, followed by 35% and 65%, with 9.4% among the undergraduate participants.
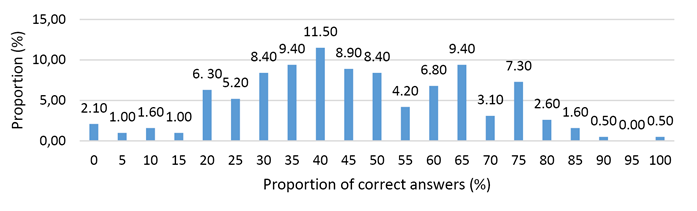
Chart 1 Distribution of the proportion of correct answers on Basic Life Support among undergraduate students from health courses. Ponta-Grossa, PR, Brazil, 2019.
Chart 2 shows that the greatest number of incorrect answers occurred in Question 1 (90.6%), which discussed the infant and child survival links, followed by Question 4 (64.9%), regarding the CPR sequence after the diagnosis of CRA. The question with the highest number of correct answers was Question 10 (74.3%), which was about the maneuver to be performed during the opening of airways, followed by Question 14 (69.1%), about the use of the Automatic External Defibrillator (AED).
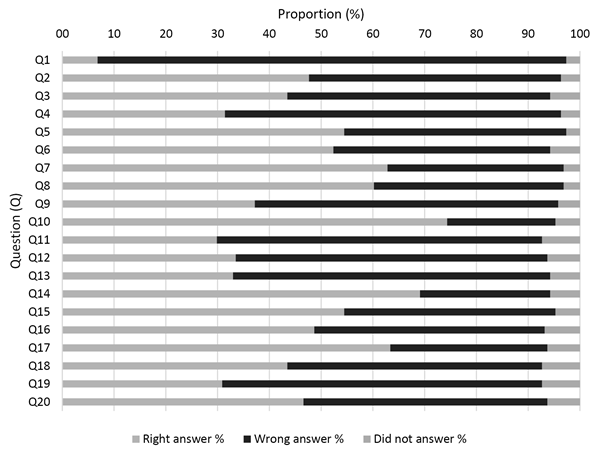
Chart 2 Distribution of errors, correct answers or no answers per question on Basic Life Support among undergraduate students from health courses. Ponta-Grossa, PR, Brazil, 2019.
A total of 30 participants (15.7%) showed knowledge that was greater than 70%, considered in the study as high knowledge about BLS. The highest level of knowledge about BLS was associated with the Medicine and Nursing courses (p <0.001). While 35.3% of Nursing and 46.2% of Medical undergraduate students had a high level of knowledge about BLS, none of the Physical Education, Pharmacy and Dentistry students showed sufficient knowledge (Table 1).
Table 1 Sample characterization and bivariate analysis between the level of knowledge about Basic Life Support and the health course attended by the undergraduate students. Ponta-Grossa, PR, Brazil, 2019.
| Course | Level of knowledge | Total n (%) | p-value | |
|---|---|---|---|---|
| Low n (%) | High n (%) | |||
| Nursing | 22 (13.7) | 12 (40.0) | 34 (17.8) | <0.001 |
| Physical education | 37 (23.0) | 0 (0.0) | 37 (19.4) | |
| Pharmacy | 33 (20.5) | 0 (0.0) | 33 (17.3) | |
| Medicine | 21 (13.0) | 18 (60.0) | 39 (20.4) | |
| Dentistry | 48 (29.8) | 0 (0.0) | 48 (25.1) | |
| Total | 161 (100.0) | 30 (100.0) | 191 (100.0) | |
Table 2 shows the sample characterization and the bivariate analysis. It was verified that the majority of the participants were females (64.9%), aged up to 24 years (74.9%). Of the participants, 64.6% were confident in performing first aid care, 63.3% affirmed they had previous extracurricular training and 66.8% confirmed the offer of the discipline (related to the topic. The majority considered the discipline to be insufficient (60.2%) and manifested the need to perform new courses within the topic (90.0%).
Table 2 Sample characterization and bivariate analysis between the level of knowledge about Basic Life Support and independent variables among undergraduate students from health courses. Ponta-Grossa, PR, Brazil, 2019.
| Variables | Categories | Level of knowledge | p-value | ||
|---|---|---|---|---|---|
| Low n (%) | High n (%) | Total n (%) | |||
| Sex | Woman | 104 (64.6) | 20 (66.7) | 124 (64.9) | 0.827 |
| Man | 57 (35.4) | 10 (33.3) | 67 (35.1) | ||
| Age | Up to 24 years | 126 (78.3) | 17 (56.7) | 143 (74.9) | 0.012 |
| 25 years or more | 35 (21.7) | 13 (43.3) | 48 (25.1) | ||
| Feels confident | No / some situations | 110 (68.8) | 12 (41.4) | 122 (64.6) | 0.005 |
| Yes | 50 (31.2) | 17 (58.6) | 67 (35.4) | ||
| Received training | No | 58 (36.7) | 11 (36.7) | 69 (36.7) | 0.996 |
| Yes | 100 (63.3) | 19 (63.3) | 119 (63.3) | ||
| Attended a course with more than 100 hours | No | 69 (90.8) | 10 (90.9) | 79 (90.8) | 0.999 |
| Yes | 7 (9.2) | 1 (9.1) | 8 (9.2) | ||
| Attended a course with more than 40 hours | No | 36 (47.4) | 6 (54.5) | 42 (48.3) | 0.656 |
| Yes | 40 (52.6) | 5 (45.5) | 45 (51.7) | ||
| Undergraduate discipline was offered | No | 62 (38.8) | 1 (3.3) | 63 (33.2) | <0.001 |
| Yes | 98 (61.3) | 29 (96.7) | 127 (66.8) | ||
| Type of discipline offered | Optional | 6 (6.4) | 2 (6.9) | 8 (6.5) | 0.922 |
| Mandatory | 88 (93.6) | 27 (93.1) | 115 (93.5) | ||
| Attended the discipline | No | 1 (14.3) | 0 (0.0) | 1 (11.1) | 0.571 |
| Yes | 6 (85.7) | 2 (100) | 8 (88.9) | ||
| Believes that the discipline offered was sufficient | No | 55 (60.4) | 16 (59.3) | 71 (60.2) | 0.912 |
| Yes | 36 (39.6) | 11 (40.7) | 47 (39.8) | ||
| Method of discipline approach | Theoretical | 5 (5.4) | 3 (10.7) | 8 (6.6) | 0.319 |
| Theoretical-practical/practical | 88 (94.6) | 25 (89.3) | 113 (93.4) | ||
| Believes in the need for extra courses | No | 17 (10.6) | 2 (6.7) | 19 (10.0) | 0.507 |
| Yes | 143 (89.4) | 28 (93.3) | 171 (90.0) | ||
In the crude analysis, there was a greater chance of having a low level of knowledge on BLS among younger undergraduate students (OR = 2.75; 95% CI: 1.22-6.21), those who did not feel confident to perform BLS (OR = 3, 12; 95% CI: 1.38-7.01) and those who did not have an offer for attending the discipline during undergraduate school (OR = 18.35; 95% CI: 2.44-138.1). After adjustment, only not having had an offer for attending the discipline during undergraduate school was associated with a low level of knowledge about BLS (OR = 13.41; 95% CI: 1.74-103.12) (Table 3).
Table 3 Analysis of crude and adjusted associations between the low level of knowledge about Basic Life Support and independent variables among undergraduate students from health courses. Ponta-Grossa, PR, Brazil, 2019.
| Low Level of Knowledge | ||||
|---|---|---|---|---|
| Variables | ORa (95%CI) | p-value | ORb (95%CI) | p-value |
| Age | ||||
| 25 years or more | 1.00 | 1.00 | ||
| Up to 24 years | 2.75 (1.22-6.21) | 0.015 | 1.76 (0.74-4.21) | 0.197 |
| Feels confident | ||||
| Yes | 1.00 | 1.00 | ||
| No/Some situations | 3.12 (1.38-7.01) | 0.006 | 2.26 (0.97-5.29) | 0.600 |
| Undergraduate course offer | ||||
| Yes | 1.00 | 1.00 | ||
| No | 18.35 (2.44-138.1) | 0.005 | 13.41 (1.74-103.12) | 0.013 |
a Crude Odds Ratio. b Adjusted Odds Ratio. * The variable ‘training course’, despite being statistically different in the bivariate analysis, was not used in the regression, because there were no correct answers among some of the analyzed courses.
DISCUSSION
In the present study, the majority of the undergraduate students from the health area in the present study showed a low level of knowledge about BLS, especially those from the Physical Education, Pharmacy and Dentistry courses. In the literature, other studies have shown the low level of knowledge about BLS among students9),(10),(12, whether in studies with greater stringency regarding the proportion of correct answers in the definition of high and/or low knowledge about BLS, such as 84%12 or 50%9. The literature, shows a wide variation in the prevalence of correct answers, between 0.1%12 and 13% among medical students9 and 25% for Nursing students10. The difference verified in the present study in relation to the national12 and international11 literature may have occurred to the instrument used, such as the variation in the content of questions to assess knowledge about BLS, or because of the professional training between the realities in each of the health area courses. Although the data from the study is related to undergraduate students, studies have verified the low performance also among professionals, in which 10.2% of the Doctors and Nurses of a public hospital had a high level of knowledge about BLS17.
The courses in Medicine and Nursing were the only ones that had undergraduate students with a high level of knowledge, as none of the students from the Physical Education, Pharmacy and Dentistry course had scores above 70.0%. A study carried out with the same questionnaire in São Paulo showed similar data, with a higher level of knowledge among students in the medical course, followed by the Nursing course12. A study carried out in Saudi Arabia showed no difference in knowledge among the students of Medicine, Dentistry, Nursing and Pharmacy courses11. The results in the present study showing a prevalence of high knowledge in students from the Medicine and Nursing courses in comparison with other studies9),(11),(12, may result from the analysis being carried out only with undergraduates, and not with students from different years after course completion. The results obtained in the present study, with a prevalence of high knowledge in the Medicine and Nursing courses in comparison with other studies9),(11),(12, might be due to the fact that the analysis was carried out with graduates only, and not with students from different years of the course completion period. Moreover, the higher performance among graduates of these courses may be associated with the offer of the discipline towards the end of the course completion, offered closer to the time of the internship, carried out mainly in a hospital environment, and, consequently, with a greater probability of using BLS practices in the academic routine. This reality becomes different in the Physical Education course, which, despite having the same workload when compared to the Nursing course, has a theoretical approach and occurs in the beginning of the course completion period, and there were no students with high knowledge. This aspect has been previously revised by the Dentistry course: the new PPC, in its 11th version, active since 2016, included the content in the discipline of Diagnosis and Oral Surgery III, offered in the third curricular year, with a workload of 136 hours and theoretical-practical basis. Additionally, when considering a study with the eligibility of trained undergraduate students only, as in the present study, there is a greater gap between the moment the content is addressed in the discipline and the moment of data collection. The other courses, Pharmacy and Dentistry, did not have the BLS content in the menu of the offered disciplines, which can demonstrate the low knowledge. This aspect has already been revised by the Dentistry course, where the new PPC, in its eleventh version, which has been used since 2016, includes the content in the discipline of Diagnosis and Oral Surgery III, offered in the third curricular year with a workload of 136 hours, having a theoretical-practical approach.
The highest rates of correct answers were found in questions regarding the opening of airways and the use of the AED. Other studies also found a higher rate of correct answers regarding the question related to the opening of airways19 and a study with newly graduated doctors verified the same result regarding the use of AED13. A study carried out with Nursing professionals indicated a higher rate of correct answers in the question regarding the recognition of CRA and the initial management, but a higher number of incorrect answers in the question regarding the opening of airways and ventilation16. The higher rate of correct answers in these subjects may be associated to the fact that they are more general topics and addressed in a more diffused manner.
In the present study, there were a greater number of incorrect answers in questions related to the links in the infant and child survival chain, and about the sequence of CPR after the diagnosis of CRA. The issues related to infants and children within the BLS were rarely addressed in the literature10, giving preference to procedures in adults, thus being the reason of the difficulty in comparing the findings in the present study. However, other studies have found a large proportion of incorrect answers in questions about the CPR sequence11),(19. The difficulty in learning these subjects can be attributed to the lack of consistent and continuous study by the students.
In the crude analysis, age was an associated factor, where younger students had a lower level of knowledge about BLS. Other studies with undergraduate students showed that students attending more advanced periods of the courses obtained a higher number of correct answers12, as well as in a study with lay people in Portugal, where older age was associated with a higher level of knowledge20. Another study, also carried out with lay people carried out in the state of Minas Gerais, Brazil, did not verify this association21, as it was not verified between doctors and nurses17. The difference in results may be associated with the difference in methodology and the target audience participating in the study. Although older age does not necessarily imply greater knowledge, it is possible to assume that older people have had more opportunities to go through learning experiences or the practical need for its application, that is, age would not be a direct predictor, but the greater clinical professional experience, in studies with students or professionals in the area, or greater maturity among older individuals to deal with adverse situations, in the case of studies with lay people.
The fact that the present study considers courses with different course completion periods - for instance, the physical education course is completed in four years, while the medical course is completed in six years - might have interfered with the results. Additionally, considering that entering an educational institution generally occurs later due to the competitive entrance exam, the medical course may include older students. One must also consider the fact that Nursing students might have attended a technical course in the area. Based on these aspects, the results must be considered with care, as these variables are difficult to interpret. When the results were adjusted, there was no association with age in the final model.
In the crude analysis, another associated aspect was not feeling confident to perform the BLS and low knowledge. Moreover, an information verified here that needs to be explored was a minority of the undergraduate students feeling confident or able to perform emergency procedures, which demonstrates a priority necessity of training for these future professionals. A study with Nurses found a moderate positive correlation between the performance of BLS procedures and clinical experience14 and a study with newly graduated physicians showed an association between longer time in clinical practice and greater confidence when performing CPR13. Therefore, in the present study, health education with a longer time in the hospital environment, as in Medicine and Nursing, including the internship, may result in students feeling more prepared to deal with BLS issues.
Failure to attending the BLS discipline during undergraduate school was associated with a low level of knowledge, both in crude and the adjusted analysis, and therefore, within the limitations of the present study, the inclusion of curricular disciplines seems to be the most appropriate way to train future health professionals in BLS. While the studies show an association of the level of knowledge with previous BLS courses9),(12),(16, this variable is not associated in the present study, either with training, courses with lower or higher workloads. This aspect may be the result of the low adherence to extracurricular courses by the participants in the present study, even though 90.0% affirmed that attending the courses is important. Several factors can explain this result: the involved cost, the methodology used in the courses, the fact that the course was non-mandatory, or the students’ expectation regarding the possibility of the content being part of the curricular activities. Moreover, in Brazil, unfortunately there is no culture of preventive safety measures, with eventual and/or continuous simulations and/or training for disasters of different kinds.
Therefore, the results of the present study demonstrated that the presence of a discipline offered in the PPC of the health area courses showed a greater impact on the level of knowledge than on the previously performed extracurricular courses. This may be associated with the fact that the disciplines have a workload distributed throughout a continuous teaching-learning process, rather than an eventual one, such as training courses. Moreover, the offer of curricular disciplines with evaluation activities that follow the standard for learning assessment may be more effective for students, since this methodology is less frequent in training courses.
Despite the contributions present in the study, some limitations should be highlighted, such as the methodological variability in the studies present in the literature and, therefore, difficulties for comparability. Different collection instruments were found to measure knowledge in BLS, which, although validated, were not the same11),(12),(20. Among these, the questionnaire by Tavares et al.12 was selected because it has been validated in Portuguese, applied to a sample containing different courses and has a large number of questions. The use of a questionnaire from another Brazilian study12 that achieved results that were similar to these presented here can reinforce the sensitivity of the questionnaire in measuring BLS and its reproducibility, even in samples from different locations, and thus, it seemed to be an adequate instrument to assess the knowledge. However, the study indicated a cutoff for the high level, with 84%22, a parameter considered high, in which a limited number of participants managed to reach this proportion. Therefore, considering the average grade for approval at the institution, it was decided to reduce the cutoff to 70%, and the knowledge was considered appropriate.
Another aspect that must be clarified is the limitation of using a questionnaire to measure the level of knowledge in BLS. About the procedural content, an assessment at the cognitive level only, in the theoretical field, becomes a limited way to assess the problem. That is, if the results shown here at the cognitive level demonstrate a low level of knowledge, they could be even worse if practical tests were performed. However, the use of questionnaires is still the main method of assessing knowledge, whether due to its low cost and the fact that it is easy to apply in different places around the world, such as in Brazil12, Peru9, United Kingdom15, or Middle East11, being instruments based on guidelines about the subject and subsequently validated. However, the existence of a standardized and universal questionnaire would be important for better comparability of results in different population samples. Additionally, the performance of longitudinal studies, capable of involving the evolution of the students’ knowledge throughout their training, is encouraged, to understand which moment of the training would be the ideal one to include the discipline about BLS. The use of data collection strategies that also included the verification of learning at a practical level could bring data more consistent with the reality about the participants’ level of knowledge.
Another question to be considered in future studies is the measurement of the participation in extracurricular activities in the area of urgency/emergency, such as leagues, monitoring activities or continuing education projects in the area. This information could help to better understand the apprehended knowledge and promote greater interest in the topic according to the intended future specialty.
Moreover, the sample is another factor of difficult comparability. While some studies include only one health course as the study universe9),(10),(15, others considered several courses regardless of the semester or year11),(12),(19, while others carry out studies with health professionals that have already graduated13),(14),(17 and even lay people20),(21. The present study assessed undergraduate students only, aiming to reduce the memory bias and increase the reliability of measuring significant knowledge. In this sense, the data from the present study become a matter of concern, considering that before working in a specific area of each profession in the health field, undergraduate students need to understand that they are health professionals and, for this reason, they must be prepared to deal with emergency situations inside and outside health services. Therefore, integrality and interdisciplinarity must be an ever increasing part of the training of human resources in health.
When verifying that knowledge about BLS was not absorbed by most undergraduate students, that is, when they should be ready for the work market, this result reinforces the need to include permanent BLS discipline in HEIs for all courses in the health area, and mainly including an adequate perspective for the common needs within each health professional’s field of action, as well as review and refresher courses of knowledge for graduated professionals, since even though they have had the training, the lack of continuous applicability of the learned knowledge can over time reduce the ability to use the clinical procedures necessary in specific cases of BLS.
CONCLUSION
Most of the study participants demonstrated a low level of knowledge about BLS, and only the students from the Medicine and Nursing courses showed a high level of knowledge.
The low level of knowledge about BLS was associated with younger age, not feeling confident in performing BLS procedures and not having attended the discipline about the topic during the professional training. However, after the adjustment, only not having attended the discipline about the topic was associated with low knowledge about BLS.

