











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Physical activity (PA) has been recognized for centuries as an important contributor to health promotion1)-(3. According to Hippocrates (460-377 BC), a prominent philosopher considered the father of modern medicine and even the first physician to provide a written exercise prescription4, “if we could give every individual the right amount of nourishment and exercise, not too little and not too much, we would have found the safest way to health”2. Also, Plato (424-348 BC) said that the “lack of activity destroys every human being’s good condition, while movement and methodical physical exercise save it and preserve it”3. An old Indian medicine book reports that the first definition of physical exercise was recorded around 700 BC as any physical action capable of producing bodily stability and strength1. Nowadays, physical activity (PA) is defined as “any bodily movement produced by skeletal muscles that results in energy expenditure, but does not include the effect of diet-induced thermogenesis"; and physical exercise (PE) as “a subset of PA that is planned, structured, and repetitive and has as a final or an intermediate objective the improvement or maintenance of physical fitness”5.
The World Health Organization (WHO), which endorsed this concept of physical activity, the Brazilian Society of Sports Medicine and Exercise6, and nine more sports medicine societies7, have intensively emphasized the importance of PA in health promotion. Physical inactivity is reported as one of the leading causes of disability and mortality8, with significant economic9 and social10)-(13 impact, making it one of the most urgent health problems of the 21st century9. PA plays an essential role in preventing and treating several chronic illnesses14)-(17, mainly noncommunicable diseases (NCDs)18. Mortality from these diseases is rapidly increasing worldwide and already accounts for more than half of the global deaths under 70 years of age19. In low to middle-income countries, such as Brazil, the risk of premature death from NCDs is 1.5 times higher than in high-income countries20. Therefore, it is indisputable that people must be physically active and the governments must apply PA as a public policy9),(21.
Several studies have shown that medical counseling encourages patients to change behaviors towards healthier lifestyles, and this represents an essential strategy for health promotion7),(22)-(26. Besides, the promotion of physical activity in medical education could increase students’ advising skills aiming to modify patient behavior27. Therefore, physicians and other health professionals should encourage the practice of PA and warn patients about the risk of physical inactivity28. These physician-induced behavioral changes in patients’ lifestyles should be better accomplished by including PA in the undergraduate institutional curricula or training21),(29. In this context, in addition to the theoretical knowledge, the medical students’ practice of PA might also be a significant additional factor for counseling30),(31, and might contribute to necessary medical training and not only for the sports medicine specialty7.
The existence of static and outdated curricula undermines professional health education considering the constant updating of the global health system and the emergence of new health risks32. In recent years, discussions on medical education in Brazil have been stimulated, and they have, in general, emphasized the need to adopt active methodologies as pedagogical strategies33),(34. Although those discussions point out that the physicians from the 21st century should have transdisciplinary training that allows them to exert multi-professional activities aiming to improve the health problems solutions33, no mention of PA among these multiprofessional activities has been reported.
In some countries, PA introduction in medical education has been stimulated35)-(37 to prepare medical students for physical activity counseling to prevent and treat diseases. In Brazil, we still do not have a picture of this situation. Since the need to prepare medical students for physical activity counseling to prevent and treat diseases is a critical one, this study investigates PA topics regarding the Brazilian active medical curricula.
METHODS
Ethical Aspects
This study does not require prior approval by an ethics committee since public access to academic curricula is guaranteed by law38.
Sample
A cross-sectional survey was conducted by convenience on two different occasions (April 2015 and February 2019) regarding the curricula of the undergraduate medical courses offered by all Brazilian public and private institutions authorized by the Ministry of Education and Culture (MEC), which regulates and supervises the educational activities in the country.
Data Collection Instruments
Initial searches were carried out on the MEC website (http://emec.mec.gov.br), focusing on the curricula of undergraduate medical programs currently active in Brazil. No distinctions were made between traditional or non-traditional curricula. All the active curricula listed by MEC have been compiled from educational institution websites. Some institutions have more than one curriculum because they have more than one medical school (on different campuses) or because they have simultaneously two valid active curricula (a new and an old one).
Data Collection Procedures
The compiled curricula were randomly divided into three groups. Two independent reviewers analyzed each group regarding the presence of topics on physical activity (PA) in the name of the curricular unit, i.e., subject or thematic module (S/TM), and/or in its respective syllabus. PA presence as a main or secondary topic within a broader topic in the syllabus was considered an approach to the subject. In case of disagreement between the two researchers examining a curriculum, the study coordinator resolved the dispute. It is essential to note that throughout this study, the term PA refers exclusively to the definition adopted by the WHO5.
Qualitative Data Analysis
Subsequently, the information was filtered to reduce possible selection biases, and then the data were pooled. The S/TMs were classified according to the type of enrollment (mandatory or optional), type of activity (theoretical, practical, or theoretical-practical), and emphasis on the content (health, athletic performance, or health and athletic performance). Therefore, this study consists of documentary research using pre-existing thematic categories.
S/TMs classification concerning the type of enrollment and type of activity was made based on the information collected from each institution’s web site. S/TMs with only theoretical activities were considered theoretical; those comprising any practical activity, aiming recreation or training, were considered practical; S/TMs with the simultaneous theoretical and practical activities were considered theoretical-practical.
The S/TMs classification concerning the emphasis (health, performance, or both) was made in an inferential way. The S/TM titled Exercise Physiology: From Normal to Pathological, for example, which was found in one institution located in the state of the São Paulo, has focused on the associations of physical exercise with either cardiac (“acute and chronic effects of physical exercise on the cardiovascular system”) or respiratory (“acute and chronic effects of physical exercise on the respiratory system”) systems, and this characterizes it as having an emphasis on health. On the other hand, the S/TM Sports Medicine, which was found in another institution in the state of São Paulo, has guidelines for evaluating athletes, among other items, which means that it emphasizes athletic performance. In some situations, the emphasis was on health and athletic performance, as observed with the S/TM Exercise and Sports Medicine, found in one of the institutions in the state of Rio de Janeiro. The excerpts “to develop skills in the evaluation of athletes” and “clinical bases for the prescription of exercise in health and disease” present in its syllabus denotes a concern with both athletic performance and health.
Quantitative Data Analysis
The present study does not have a sample calculation with a description of statistical power because its objective was to analyze the universe of curricula made available by the institutions.
Data were described as frequency (%) using Microsoft ExcelTM (Microsoft Corporation, Redmond, WA), and the illustrations were edited using Microsoft PowerPointTM (Microsoft Corporation, Redmond, WA).
The subjects or thematic modules with names that indicated the approach to the topic were considered in the frequency calculation. Curricula with unavailable program content of curricular units were excluded from the analysis. However, to minimize sample loss, whenever the necessary information was not available on the institution’s website, it was requested from the institution at least twice by phone and/or e-mail. Only in the absence of a response from the institution, the curriculum was excluded from the analysis. Many of the unavailable curricula at the time of the search were under extinction and being replaced by new curricula, according to the e-MEC website.
A total of 83 (27.1%) of 306 active curricula in 2015, and 51 (15.1%) of 337 in 2019, were not analyzed.
RESULTS
A total of 223 (72.9%) of 306 active curricula in 2015, and 286 (84.9%) of 337 in 2019, were identified. All these curricula were then analyzed regarding disciplines, thematic modules, and even isolated topics on PA.
The selected S/TMs were subsequently classified according to the type of enrollment (mandatory or optional), type of activity (theoretical, practical, or theoretical-practical), and emphasis on the content (health, athletic performance, or health and athletic performance).
The number of S/TMs with PA content in each category was then converted into frequency (%).
Figure 1 depicts a diagram of the screening of Brazilian medical schools’ curricula concerning the frequency of PA contents in their S/TMs, as well as in the classification of these curricular units regarding the type of enrollment (mandatory or optional), type of activity (theoretical, practical or theoretical-practical), and emphasis on the content (health, athletic performance or both) in April 2015 and February 2019.
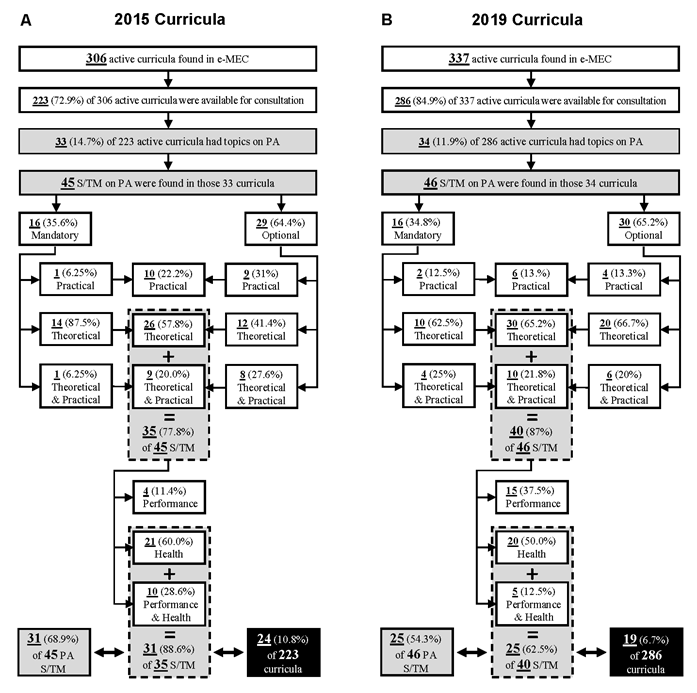
Figure 1 Diagram of the screening of Brazilian Medical Schools’ curricula concerning the presence of subjects or thematic modules (S/TM) with topics on physical activity (PA) in A) April 2015 and B) February 2019. The S/TM with topics on PA were classified concerning the type of enrollment (mandatory or optional), type of activity (theoretical, practical, or theoretical-practical), and emphasis on the content (health, athletic performance, or both).
In 2015, of the 223 analyzed medical schools’ curricula, only 24 (10.8%) had at least one S/TM with a topic concerning PA and focused on health or athletic performance and health. In 2019, this number dropped to 19 (6.7%) of 286 analyzed medical schools’ curricula.
Table 1 and 2 depict the distribution of S/TMs with topics on PA found in medical curricula of Brazilian educational institutions by federation state and also by the type of enrollment (mandatory or optional), type of activity (theoretical, practical or theoretical and practical), and focus (health, performance or health and performance) in 2015 and 2019, respectively.
Table 1 Distribution of topics concerning physical activity (PA) found in the medical curricula of Brazilian educational institutions, by Federation state, type of enrollment, approach and emphasis. Brazil, 2015.
| Subjects/Thematic Modules | Federation state | Type of enrollment | Type of activity | Emphasis | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mandatory | Optional | Practical | Theoretical | Theoretical & Practical | Performance | Health | Both | ||
| Physical Activity in Health Promotion II | AC | X | X | X | |||||
| Metabolism | AP | X | X | X | |||||
| Locomotion | AP | X | X | X | |||||
| Locomotion and Prehension | BA | X | X | X | |||||
| Sports Medicine | CE | X | X | X | |||||
| Sports Practice I | DF | X | X | ||||||
| Sports Practice II | DF | X | X | ||||||
| Sports Medicine | MA | X | X | X | |||||
| Sport Physiology | MG | X | X | X | |||||
| Sports Medicine | MG | X | X | X | |||||
| Aging and Physical Activity | MG | X | X | X | |||||
| Locomotion and Prehension | MG | X | X | X | |||||
| Biological Basis of Medical Practice | MG | X | X | X | |||||
| Musculoskeletal System: Skin and Attachments | MG | X | X | X | |||||
| Geriatrics | MG | X | X | X | |||||
| Clinical Exercise Physiology | MG | X | X | X | |||||
| Sports Practice I | MG | X | X | ||||||
| Sports Practice II | MG | X | X | ||||||
| Biological Functions | PA | X | X | X | |||||
| Metabolism and Nutrition | PA | X | X | X | |||||
| Sports and Exercise Medicine | PE | X | X | X | |||||
| Medicine for the Elderly | PE | X | X | X | |||||
| Sports and Exercise Medicine | PE | X | X | X | |||||
| Culture, Sports, Interpersonal Relations, Humanization | PE | X | X | X | |||||
| Locomotion and Prehension | PR | X | X | X | |||||
| Sports Medicine | PR | X | X | X | |||||
| Exercise and Sports Medicine | RJ | X | X | X | |||||
| Exercise and Sports Medicine | RJ | X | X | X | |||||
| Exercise and Sports Medicine | RJ | X | X | X | |||||
| Musculoskeletal system | RJ | X | X | X | |||||
| Exercise Physiology | RJ | X | X | X | |||||
| Exercise and Sports Medicine | RJ | X | X | X | |||||
| Physical Activity, Health and Quality of Life | RN | X | X | X | |||||
| Physical Activity, Leisure and Culture | RN | X | X | X | |||||
| Sports Practice I | RN | X | X | ||||||
| Sports Practice II | RN | X | X | ||||||
| Sports Practice I | RN | X | X | ||||||
| Sports Practice II | RN | X | X | ||||||
| Physical Activity and Health | RS | X | X | X | |||||
| Sports Medicine | SP | X | X | X | |||||
| Physical Education | SP | X | X | ||||||
| Sports Medicine | SP | X | X | X | |||||
| Exercise Physiology: From Normal to Pathological | SP | X | X | X | |||||
| Exercise Physiology: From Normal to Pathological | SP | X | X | X | |||||
| Physical Education | SP | X | X | ||||||
| Total | - | 16 | 29 | 10 | 26 | 9 | 4 | 21 | 10 |
Abbreviations: AC, Acre; AP, Amapá; BA, Bahia; CE, Ceará; DF, Distrito Federal; MA, Maranhão; MG, Minas Gerais; PA, Pará; PE, Pernambuco; PR, Paraná; RJ, Rio de Janeiro; RN, Rio Grande do Norte; SP, São Paulo.
Table 2 Distribution of topics concerning physical activity (PA) found in medical curricula of Brazilian educational institutions, by Federation State, type of enrollment, approach and emphasis. Brazil, 2019.
| Subjects/Thematic Modules | Federation State | Type of enrollment | Type of activity | Emphasis | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mandatory | Optional | Practical | Theoretical | Theoretical- Practical | Performance | Health | Both | ||
| Physical Activity in Health Promotion | AC | X | X | X | |||||
| Integrated Health Practices I | AC | X | X | X | |||||
| Integrated Health Practices II | AC | X | X | X | |||||
| Integrated Health Practices III | AC | X | X | X | |||||
| Integrated Health Practices IV | AC | X | X | X | |||||
| Teaching, service and community interaction practice | AP | X | X | X | |||||
| Geriatrics | CE | X | X | X | |||||
| Locomotor System | CE | X | X | X | |||||
| Geriatrics | CE | X | X | X | |||||
| Geriatrics | CE | X | X | X | |||||
| Integral Health Actions VI | CE | X | X | X | |||||
| Sports Medicine | DF | X | X | X | |||||
| Sports Medicine | ES | X | X | X | |||||
| Exercise Physiology and Sports Physical Activity - Futsal | MG | X | X | X | |||||
| Exercise Physiology and Sports Physical Activity - Volleyball | MG | X | X | X | |||||
| Physical and Sports Activity - Physical Exercises and Body Weight Control - Futsal | MG | X | X | X | |||||
| Physical and Sports Activity - Physical Exercises and Body Weight Control - Volleyball | MG | X | X | X | |||||
| Locomotion and Prehension | MG | X | X | X | |||||
| Sports Medicine | MG | X | X | X | |||||
| Sport Nutrition | MG | X | X | X | |||||
| Locomotion | MT | X | X | X | |||||
| Locomotion and Gripping | MT | X | X | X | |||||
| Locomotion and Gripping | MT | X | X | X | |||||
| Locomotion | PA | X | X | X | |||||
| Health and Quality of Life | PA | X | X | X | |||||
| Sports and Exercise Medicine | PE | X | X | X | |||||
| Exercise Physiology | PI | X | X | X | |||||
| Exercise Physiology and Sports Medicine | PR | X | X | X | |||||
| Sports Practice | PR | X | X | ||||||
| Sports Medicine | PR | X | X | X | |||||
| Exercise and Sports Medicine | RJ | X | X | X | |||||
| Sports Medicine | RJ | X | X | X | |||||
| Physical Exercise Physiology | RJ | X | X | X | |||||
| Exercise and Sports Medicine | RJ | X | X | X | |||||
| Sports Practices I | RN | X | X | ||||||
| Sports Practices II | RN | X | X | ||||||
| Physical Activity, Leisure and Culture | RN | X | X | X | |||||
| Sports Medicine | RN | X | X | X | |||||
| Body Practices in Health Promotion and Quality of Life | RN | X | X | ||||||
| Sports Traumatology | RO | X | X | X | |||||
| Physical Education - Sports Practice I | SC | X | X | ||||||
| Physical Education - Sports Practice II | SC | X | X | ||||||
| Introduction to Sports Medicine | SP | X | X | X | |||||
| Exercise Physiology Applied to the Medical Clinic | SP | X | X | X | |||||
| Exercise Physiology Applied to the Medical Clinic | SP | X | X | X | |||||
| Physical Activity and Health | SP | X | X | X | |||||
| Total | - | 16 | 30 | 6 | 30 | 10 | 15 | 20 | 5 |
Abbreviations: AC, Acre; AP, Amapá; CE, Ceará; DF, Distrito Federal; ES, Espírito Santo; MG, Minas Gerais; MT, Mato Grosso; PA, Pará; PE, Pernambuco; PI, Piauí; PR, Paraná; RJ, Rio de Janeiro; RN, Rio Grande do Norte; SP, São Paulo.
In 2015, there was only one state (AC) with a mandatory theoretical-practical S/TM with topics focused on the PA benefits for health (Physical Activity in Health Promotion).
In 2019, the undergraduate program in Acre (AC) adopted a new curriculum and began to consider that topic as optional but added four subjects containing the topic of PA (Integrated Practices Health I, II, III, and IV).
In general, the curricular unit of Sports Medicine and other similar ones, which are not mandatory, are focused exclusively on performance.
It is worth mentioning that S/TM on pharmacology was mandatory in all assessed curricula.
Overall, the 2019 search showed that when S/TMs containing topics on physical activity were mandatory, PA was only a small part of a broad administered content (e.g., Geriatrics, Locomotion, Integrated Health Practices, among others).
There were some S/TMs (e.g., Exercise and Sports Medicine, in Table 1; Geriatrics, in Table 2) that appeared twice or more in only one federation state because they belong to different medical curricula.
DISCUSSION
To the best of our knowledge, this is the first study that investigated the presence of PA topics in the Brazilian medical schools’ curricula. Since regular physical exercise is widely known to bring people many health benefits17),(39)-(42, in addition to reducing health care expenses43-45, this study brings evidence that Brazilian physicians are not being prepared to consciously participate in the prophylactic and therapeutical use of physical activity. The supporting evidence is the scarcity of topics on physical activity in Brazilian medical curricula (Figure 1).
The reduction between 2015 and 2019 in the absolute number of curricular units that address PA in Brazilian medical curricula (Figure 1) sounds alarming and unsustainable in all possible aspects, given the need to improve quality, competence, efficiency, and reduction of public health costs, especially in a society where the physician plays an essential role in the health-promoting process. This curricular gap means that neither medical schools nor the Government are fully exercising their roles. Medical schools must comply with principles of ethical commitment and social relevance to implement, in the face of public policies for education, the necessary changes to adapt undergraduate medicine curricula to the demand for quality health services for the population33. It is worth mentioning that this reduction in curricular units that address PA occurs in the context of an increase in chronic diseases and their risk factors in Brazil46, which is absolutely unjustifiable, since physical exercise is one of the greatest allies in the prevention and control of these diseases47),(48.
About one-third of the world population is physically inactive49 and overweight, and obesity rates are alarming and have been increasing over the years50. In Brazil, 41.2% of men and 50.4% of women are physically inactive51. It is a consensus among experts that PA itself contributes substantially to health promotion. Up to 80% of coronary heart disease, 90% of type 2 diabetes, and one-third of cancers can be prevented by healthy habits, maintaining a desirable weight, and regular physical activity52. Also, at least 13 different cancer types show a risk reduction by leisure-time physical activity practice53. Physical activity contributes to the regulation of the immunological system and reduces systemic chronic inflammation17),(40),(41, which is the leading cause of comorbidities and death worldwide17.
As mentioned before, increasing the practice of PA has become an important global issue. Physical inactivity is one of the leading causes of disability and mortality8, with great economic9),(45, and social10)-(13 impacts, making it one of the most urgent health problems of the 21st century9. Therefore, PA should be prioritized worldwide as part of a comprehensive strategy to reduce illnesses, especially the NCDs17),(45. In this context, recently, Arocha Rodulfo suggested that a sedentary lifestyle should be considered a disease54. This suggestion makes sense. Muscles work as an endocrine gland55 and can interfere in all human systems17),(39. In turn, PA is essential to modulate muscle epigenetics56, promoting the release of thousands of proteins into the bloodstream57.
We observed that pharmacology contents appear as mandatory during the curricula evaluation, without exceptions. This observation contrasts with the presence of PA topic, which occurs in medical curricula as an exception and not a rule. However, PA may behave as a medication2),(14),(39),(58 in many cases, with actions comparable to or even superior to drug interventions14. While some medications used to treat the most common conditions, such as NCDs, may increase the risk of other diseases59)-(63, PA may even modulate the immune system, contributing to the prevention and/or treatment of several illnesses40),(41, and increase longevity64. This action of PA is why the pharmaceutical industry has been searching for pharmacological agents that can mimic the benefits of exercise, the ”exercise pill”65. A change in the disease-drug paradigm involves medical education, since the physician is the health professional who exerts the most significant influence on the population29.
The incorporation of lifestyle medicine in medical education has already been proposed21),(66),(67. Lifestyle medicine is the evidence-based practice committed to helping individuals and families to adopt and sustain behaviors that promote health and improve quality of life. These healthy behaviors include but are not limited to eliminating tobacco use, improving diet, increasing physical activity, and moderating alcohol consumption66. The need to include topics on PA, nutrition, personal care, and behavior changes in a topic called ‘Lifestyle Medicine’ in both the undergraduate medical curriculum and all continuing medical education levels is fundamental. PA should be present in longitudinal, transversal, and interdisciplinary discussions on the prevention and/or therapeutics of chronic degenerative diseases21),(68.
The promotion of physical activity in medical education requires that undergraduate medical programs increase the students’ awareness about PA’s benefits for their health and develop counseling skills to modify patient behavior27. Indeed, a robust dose-effect relationship exists between the volume of leisure-time PA and medical students’ quality of life69. Physicians who do not practice PA and have a body mass index (BMI) above the reference range considered normal do not feel confident recommending PA to their patients70. Additionally, physicians engaged in a physical exercise routine feel more confident and more prone to recommend exercise practice during the consultation70),(71.
The students and physicians’ lack of knowledge and confidence seems to be the worldwide reality. An informal survey of sports and exercise medicine practitioners suggested no significant teaching of sports and exercise medicine in the core medical curricula in Australia, Canada, Greece, Italy, the Netherlands, New Zealand, South Africa, or the USA72. The world situation does not seem to be so different from the situation described in the present Brazilian study.
Although many US medical schools report providing some PA content, the time dedicated to this topic is still lower than that dedicated to other topics, such as nutrition education35.
In Australia, most medical schools reported the inclusion of some physical training in their medical curricula. However, key topics, such as the national strength training recommendations, is not taught in most schools in Australia36.
In the United Kingdom (UK), sports and exercise medicine in the undergraduate medical curriculum was proposed almost forty years ago73. In a 2011 survey about the UK medical undergraduate curricula, in 25 of 33 medical schools that answered the survey, 100% included musculoskeletal medicine, 68% included exercise and obesity, and only 40% included sports and exercise medicine74. However, many studies describe a lack of coverage of this topic in the UK medical curricula72),(74)-(77. A 2013 study aiming to assess final-year medical students’ knowledge about the physical inactivity risks and their confidence in recommending PA concluded that the medical students do not have the necessary knowledge and skills to recommend PA to their patients, thus indicating the need for more solid medical training in this regard37. In a more recent study carried out at 22 UK medical schools, students had insufficient knowledge of the UK Chief Medical Officer’s Guidelines for adult physical activity, low confidence in counseling, and a tendency to better recognize the importance of exercise aimed at prevention but not for disease management, which reinforces the need to promote knowledge of the benefits of PA not only for the prevention of NCDs but also for its management78.
Given PA’s relevance for the prevention and treatment of many physical and mental diseases, it is unlikely that the attention it currently receives is sufficient to prepare medical students for their professional performance. As Jaques and Loosemore asked, “Why is PA medicine not adequately included in the undergraduate curriculum”72? Impediments include lack of curricular space, time, and qualified educators75)-(77),(79. Expansion of curricular units and secondary care clinicians’ education is part of the solutions for these impediments, besides the teaching of physical activity37. Multiagency coordination involving government departments and undergraduate and postgraduate curriculum leads is also needed37. Moreover, innovative ideas are needed to integrate greater quantity with better quality in PA use to train the next generations of physicians35.
Although the family doctor, who congregates preventive and personal health services80, has been identified by the community as the preferred PA information source among all health professionals81, medical education involves adequate training on the topic, regardless of professional specialization. In this aspect, the use of active methodologies to study the importance of physical activity in health promotion and treatment of diseases can be an innovative and an appropriate pedagogical strategy for medical education in this area of knowledge.
In Brazil, the National Curricular Guidelines for undergraduate medical courses cover health promotion and prevention practices, including PA82. However, the curricula do not show whether - and certainly not when and how - PA is addressed, as shown by this study, bringing great uncertainty regarding the debate on a necessary and urgent topic for future doctors. It is essential that the inclusion of PA in curricula be programmed and take place in different contexts, not only from a biological point of view or by a specific medical area - as this would probably lead to purely prescriptive and decontextualized guidance - but also from a perspective of salutogenesis, with an approach aimed at changing the population’s lifestyle. In this context, tools that contribute to a better doctor-patient relationship through adequate communication, such as motivational interview83 and patient-centered medicine84, are of great importance in the lifestyle change process, and therefore, the debate on PA should be included along with such tools.
It is a fact that PA is seen as part of other topics in medical schools and can be worked on within various curricular units. However, considering the findings of the present study and the raised discussions, it is essential that the approach be explicit and programmed in the medical curricula, not necessarily as a curricular unit, but longitudinally during the course and, ideally in conjunction with other discussions, aimed at both disease prevention and treatment. The mere presence of PA in the syllabus of mandatory curricular units can be an initial step to guarantee its adequate inclusion in medical education.
Strengths and limitations
The greatest strength of the present study is its pioneering characteristic, since this is the first study on the proposed topic carried out in the country. Another strength is its proposal to analyze all pedagogical programs of medical courses in the country. Since the study effectively analyzed 72.9% (in 2015) and 84.9% (in 2019) of the undergraduate medical curricula in Brazil, the points addressed herein represent the overall situation of Brazilian medical education regarding physical activity for health promotion.
It is essential to highlight that the unavailability of the medical schools’ curricula at the institutions’ websites totaling 27% (83/306) in 2015 and 15.1% (51/337) in 2019 does not represent a study limitation but constitutes a severe transgression by the institutions, since Brazilian law determines that universities and colleges must publish and keep up to date the curricula and curricular components of their courses on specific internet pages38.
One of the study limitations was not identifying curricular units that work with PA within broader topics and that do not necessarily contain the term PA in its name. Moreover, some of the accessed institutional documents were very succinct and did not allow an in-depth analysis of how PA was effectively addressed in its program.
CONCLUSION
The presence of curricular units with contents on physical activity in only 10.8% of the investigated curricula in 2015 and 6.7% in 2019 should serve as a warning for the medical education institutions about the need of reviewing their curricula to better prepare future physicians for the task of facing the practice of physical activities for their health, as well as to advising patients on the role of physical activity in disease prevention and treatment. The economic and social burden of physical inactivity enforces this need.
The inclusion of longitudinally distributed PA contents in medical curricula would include a mandatory type of enrollment, theoretical and if possible - practical approaches, and emphasis on health promotion and treatment of diseases. In addition to contributing to their health promotion, these changes can promote the engagement of the trained professionals during their lifetime, which is desirable, since those physicians who are engaged in a physical activity routine feel more confident and more prone to advising the practice of exercise to their patients.

