











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Since March 2020, from the moment the World Health Organization (WHO) declared COVID-19, the disease caused by the SARS-CoV-2 virus a pandemic, the world has undergone an intense revolution. Up to July 2020, there were 15,012,731 COVID-19 cases confirmed worldwide, accounting for 619,150 deaths1. During the same period, in Brazil, more than 2 million cases were confirmed, with the state of Ceará showing one of the highest incidence rates2. This situation resulted in the publication of a decree that determined the closure of non-essential activities related to commerce, as well as public and private education institutions3.
Elective care was mostly suspended during the period, encouraging the use of remote care, even in the absence of due experience4. In Brazil, the public health system was aimed almost entirely towards the fight against coronavirus infection, with a direct impact on medical education, whether for internship students or medical residents5.
This change prevented the access to the main learning scenarios: classrooms, laboratories, simulation centers, community, hospitals, and primary care centers. Thus, the virtual environment has become the most appropriate one6. Distance learning (DL) has become an important tool for the cognitive domain development, which allows the sharing of information, conducting research, and expanding the theoretical knowledge, in addition to reaffirming of dominant values in today’s society, such as distinction and individualization7. Telemedicine can be considered in this context, expanding the scope for teaching, facilitating the acquisition of knowledge and decision making, in addition to the development of coordination and leadership skills among students8. The need for social distancing made pedagogical programs impossible, whether remote or face-to-face, making it necessary to provide a temporary system to provide instruction and educational support with a quick design, characterizing the concept of emergency remote teaching9. In the United Kingdom, practical activities and assessments in different university campuses have been blocked, with an impact on the confidence and training of students attending the last year of medical school10.
Given the entire context of insecurities and uncertainties, there is a real concern as to when and how health care will resume, as well as questions about how medical education will behave11. What obstacles are we facing and which ones will remain? What strategies can be carried out? There are several challenges and different types of solutions.
Based on this context, the article aims to report the experience of Centro Universitário Christus (Unichristus) regarding the changes that occurred in the practical scenarios of clinical experiences during the pandemic and social distancing period.
EXPERIENCE REPORT
Unichristus is a private education institution, located in the city of Fortaleza, state of Ceará, Brazil, and has an institutional Grade 5 according to the National Higher Education Assessment System (Sinaes). The medical course was implemented in 2006, with the highlight of being one of the first medical courses in Ceará to use active learning methodologies. It has a hybrid teaching plan, involving methodologies such as dialogued exhibitions, flipped classroom, simulation laboratory, problem-based learning (PBL), team-based learning (TBL) and clinical experiences. The latter takes place in some affiliated hospitals belonging to the public health care network, and, mainly, at the Clínica Escola de Saúde (CES) of the university center, where there are several specialties.
The CES, one of the social arms of Unichristus, provides free care in multiple specialties, integrating care and teaching, providing the development of several living scenarios for medical students. In the center, the Specialized Care Service (SAE, Serviço de Atenção Especializada) program for sexually transmitted infections (STIs) and AIDS stands out, through a partnership with the Brazilian Unified Health System (SUS, Sistema Único de Saúde).
Prior to the coronavirus pandemic, all semesters preceding the ninth (first semester of medical internship) included activities with experiences defined by the semester schedule, with emphasis on the eighth semester, when several experiences took place in clinical specialties (rheumatology, cardiology, pneumology, gastroenterology, nephrology, infectology, geriatrics, psychiatry, dermatology, endocrinology and internal medicine), pediatrics and gynecology. During this period, one of the objectives is to retrieve previous knowledge, relevant to the medical internship that is imminent.
During the pandemic, due to the social distancing and the closing of educational institutions by the state government, the CES services were suspended and the affiliated hospitals stopped receiving students, making the living experience scenarios unfeasible. This conduct was even reinforced by the Regional Council of Medicine of Ceará (CREMEC), which suggested the temporary suspension of health services considered to be elective. In this context, for students attending the eighth semester and about to start the medical internship, a telemedicine project was created together with a non-governmental organization, aiming to assist patients with suspected or confirmed coronavirus infection. The telemedicine services followed CREMEC Resolution N. 56/2020, with registration in electronic medical records, guaranteeing the integrity, safety and confidentiality of the data, and the issuance of medical prescriptions and certificates if necessary, bearing the physician’s digital signature. The signing of the patient’s Free and Informed Consent Form (ICF) was mandatory for the start of care.
Teachers from different CES specialties were submitted to previous training through dialogued exhibitions on SARS-CoV-2 virus infection lasting 60 minutes, followed by three hours of practice on the digital platform that was to be used. After this stage, telemedicine services were initiated, with the presence of the students in a virtual room created by the Google Meet® application. The patients, seen through another platform that contained digital medical records and video, were attended to while in the physical presence of a nursing team, responsible for checking vital signs, reading complementary exams and eventually solving a technical problem with the transmission. All professionals attending a face-to-face event followed the biosafety protocols12. The students, initially spectators, observed the remote care experience through a shared full screen and, after the consultation was concluded, there was a discussion about the case and other relevant aspects, without the patient in the room, similarly to what would happen in a real-life environment. In parallel with the project, students also watched lectures that addressed aspects of the disease at both the primary and tertiary levels of health.
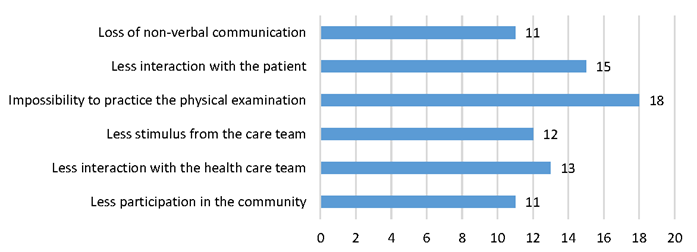
Subsequently, a satisfaction survey was carried out regarding the use of telemedicine at Unichristus, involving a total of 18 students, with the following advantages being mentioned (Chart 1): reduced risk of contamination (16/18), greater savings regarding transportation and fuel (13/18), in addition to maintaining the learning process (9/18). It is worth mentioning the little experience on the part of the interviewees, since 17 students had never participated in distance learning. Some disadvantages were observed (Chart 2): impossibility to practice physical examination (18/18), less interaction with the health care team (13/18) and with the patient (15/18). The loss of non-verbal communication was seen as a disadvantage by 11 students. Depending on the quality of the internet service for good practice was mentioned as a problem by 17 students.
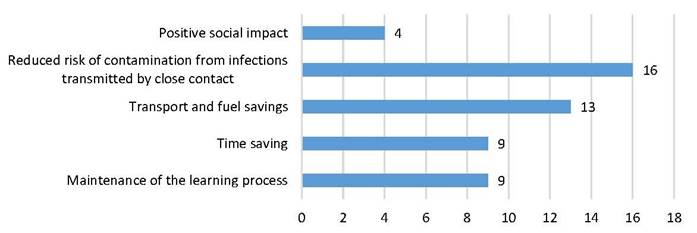
Chart 1 Advantages considered from the experience of practices through telemedicine by medical students (n = 18).
Infection-related rates continue to decline steadily in the state, mainly in the capital city, allowing a state government resumption plan, with partial opening of elective health services being allowed, following the biosafety criteria. The CES has resumed in-person care in the several specialties, with a smaller number of patients being scheduled, without the presence of students, according to the social distancing guidelines. After authorizing the operation of educational institutions, the intention is to return to real-life experience activities, with a restricted number of students per classroom, defined together with the institution’s safety engineering department.
DISCUSSION
Telemedicine consists in using the Information and Communication Technologies (ICT) to perform patient’s at-distance care, being useful for those located in remote areas. It is an accessible, lower-cost care system, which allows exercising equity in the health care system. In Brazil, there is great potential for the development of telemedicine, given the extensive territorial dimension and the irregular distribution of physicians in the country13.
Telemedicine was an important tool in minimizing the consequences of losing the scenario of real-life experiences during the pandemic. It was possible to offer assistance and information to the population, as well as the possibility of providing flexible, innovative, accessible and safe teaching, characteristics that are essential for remote teaching14. It is clear that the institution used a worldwide trend. In a multicenter study carried out in pediatric gastroenterology training centers in North America, it was observed that 98% of the programs did not use telemedicine before the pandemic, whereas currently, 76% of them started using it15. Using a tool that can improve care at a lower financial cost during this period is something to be considered16.
Other positive points can be observed. The institution aimed to follow the biosafety measures for individuals working in face-to-face activities, in addition to showing an example of social contribution at a time full of adversities. There was a clear perception about the need to change. A positive point of this pandemic period is the opportunity for professional development and innovations in medical education17. The technology, allowing at-distance discussion and sharing of information, allows the qualification on the topic in a pertinent manner. Videoconferences allow professionals from countries with greater incidence of the disease to share what is actually happening, facilitating the adoption of preventive and control measures in other locations18.
On the other hand, the absence of face-to-face experiences can generate some educational losses. Face-to-face practical activities can be beneficial, aiming to introduce the student directly into the community and make them feel as an integral part of the health care team. There is the greatest of all incentives, especially for doctors simultaneously involved in teaching and assistance activities, in face-to-face environments19.
Some technical problems regarding the quality of the internet connection and the performance of the involved platforms were observed. Data from other experiences in the literature have also reported these adversities. In another experience report involving centers on two continents (North America and Africa) during an 18-month period, it was shown that there were some interruptions in 30 meetings, either due to connectivity problems, audio or image delay20.
The experience report has some limitations, considering that the literature still lacks studies about the impact on students’ cognitive gain during this period, and also considering this is the students’ first experience with so many and varied technological tools. The impact of these teaching modalities on students’ confidence and security, especially those approaching the end of medical school, needs to be better evaluated.
Despite the existing limitations, it is important to minimize, as much as possible, the exposure of students to patients infected by the SARS-CoV-2 virus, while keeping the transmission of knowledge, in addition to the fact that it is a comfortable tool for the patient21. The experience with telemedicine can be complemented by e-learning, allowing the development of a new hybrid teaching model22. The pandemic has caused a disruption in medical education, resulting in irreversible changes. Online lectures have shown to be useful; however, there is no substitute for clinical internships, which are essential for the curriculum. Virtual medical education and telehealth service, whether at home or in a hospital environment, can be proposed as a complement to practical teaching23.
CONCLUSION
It is a fact that the current circumstances may promote some educational loss, such as the impossibility of training physical examination and better interaction with the health team and the patient. However, opportunities for changes, improvement and development of teaching methodologies can be created. Remote education can be consolidated in the future, becoming a complementary means to the current teaching methods, being part of the institutional curriculum. An accessible and flexible technological tool can facilitate the students’ acceptance, who belong to a generation that grew during the same period as Information and Communication Technologies (ICT), being considered digital natives24.
One can consider the current moment as before and after the pandemic, leaving the academic community, teachers and students, to reflect, extract and apply the positive experiences that occurred during the period.

