











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
The mistreatment of medical students is prevalent throughout the world and has been pointed out since the early 1980s1. In 2011, The Association of American Medical Colleges2 more specifically described mistreatment through a list of behaviors with an effort to clarify the definition. Examples include sexual harassment, humiliation, psychological or physical punishment, and harassment based on race, religion, gender, or sexual orientation; behaviors which portray disrespect for the dignity of others and unreasonably interfere with the learning process.
A considerable number of studies3)-(6 have found that most medical students around the world experience high incidence rates of mistreatment during training. A meta-analysis carried out in 2014, including 59 studies, reported that the combined prevalence of harassment and discrimination of medical students was about 59.6%7.
Although mistreatment situations are not exclusive to medical training environments, Rautio et al.8 found a higher prevalence in medical courses when compared to courses in human science and technology areas. Some teachers have stated that these abuses are an unavoidable part of medical education9),(10. However, abusive behaviors result in negative effects on the students’ well-being and learning abilities. Reports indicate9),(11),(12 that perceived abuse has been associated with long-term mental health consequences such as depression, alcoholism, and suicidal attempts. Students who have been victims of mistreatment, belittlement, harassment, or bullying report a loss in their relationship with teachers, are more dissatisfied with their professional choice, and more frequently consider dropping out of the course, feeling more stressed and depressed.
Therefore, it is noted that in addition to representing a common phenomenon in the medical training environment, mistreatment can result in several types of damage with different characteristics. Some result from sporadic situations, while others, from persistent ones. Some represent immediate damage, such as impairment in the relationship with the teacher and in the acquisition of knowledge. Others, however, are identified later and can have a long-term impact on the students’ lives, including depression, increase consumption of alcoholic beverages and even dropping out of the course. Thus, the question arises: how to collect data involving such a sensitive subject and with such diversified outcomes, using an ideal approach? What has been practiced in the existing literature?
Thus, the main goal of this study was to analyze/evaluate the methodology used in recent research describing the consequences of a hostile learning environment on quality of life, mental health and/or academic performance and propose a new approach.
METHOD
Study type: short review
A literature search was carried out from November 2019 to January 2020 to evaluate the recent literature related to the effects that any type of mistreatment can cause to undergraduate medical students and residents.
Keyword selection and database search
A comprehensive literature search was performed in 6 databases: PubMed, Scopus, Web of Science, SciELO, PsycINFO and Cochrane Library. The terms initially used in the search included descriptors and words from the text associated with key concepts related to the review topic. The terms were divided into 2 broad categories: 1) mistreatment types in the academic environment (“mistreatment”, “harassment”, “sexual harassment”, “belittlement”, “abuse”, “intimidation”, “bullying” and “violence”); 2) target population (“medical students”, “medical school”, “residents”, “clinical internship” and “medical interns”). The search terms were refined during the bibliographic search and different combinations of descriptors and keywords were used according to the database and available controlled vocabularies. The Endnote® program was used to organize and manage references, as well as to eliminate duplicates.
Eligibility criteria
Inclusion/exclusion criteria were applied using a modified PICO - Population, Intervention, Comparison, Outcome - framework, which offers a useful, structured, and tailored approach to determine whether an article could be included or excluded from the research. However, the PICO formula was modified by substituting ‘comparison’ for ‘environment’ (Table 1).
Table 1 PICO framework.
| P (population) | medical student OR medical school OR resident OR medical intern OR clinical internship |
| I (intervention) | harassment OR mistreatment OR belittlement OR bullying OR sexual harassment OR abuse OR intimidation OR violence |
| C (comparison) | clinical workplace OR hospital OR learning environment OR academic environment |
| O (outcome) | deleterious effects on life quality OR depression OR alcoholism OR stress OR anxiety OR poor learning environment OR satisfaction/dissatisfaction with career planning |
Inclusion criteria using the PICO method. P Population, I Intervention (variable of interest), C Comparison (substituted for Environment as it more accurately aligns with this research), O Outcome.
The inclusion criteria comprised original studies, which included longitudinal studies - cohort and case-control, cross-sectional studies, case reports, experience reports, and experimental studies. Only articles written in English, Portuguese, or Spanish languages from 2005 to 2019 that described deleterious/negative effects of different types of mistreatment in medical students or residents were selected. The exclusion criteria comprised articles published before 2005 and those addressing the issue of academic violence, but not describing its impact on students. Studies discussing the consequences of mistreatment of any health care professionals or students from other health areas were also excluded. Research letters, articles without abstracts (because the abstracts were checked to review the article) and book chapters were not included in this review.
After this first step, a manual search of the references from the selected studies was also performed and the relevant data were summarized and organized.
RESULTS
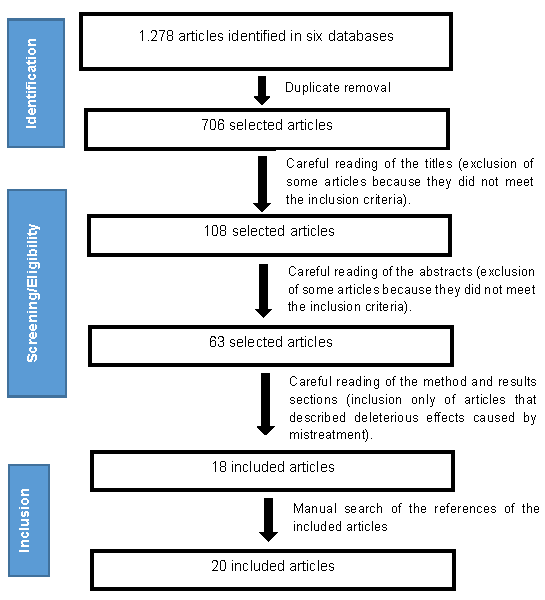
One thousand, two hundred and seventy-eight (1,278) articles were found in the six databases (PubMed: 203; Scopus: 347; Web of Science: 355; SciELO: 53; Cochrane Library: 31; PsycINFO: 289). After excluding the duplicates, 706 articles remained. From these, based on the eligibility criteria, 688 articles were excluded. Through a manual search of the 18 selected articles, two more were included, resulting in a total of 20 articles that were analyzed in this research (Figure 1).
This brief review showed that all abovementioned authors used questionnaires or scales as instruments to collect data. Some complemented their research with interviewing techniques. A description of all comparative parameters related to the methodologies used in these 20 studies was performed. The results are organized and displayed in Table 2.
Table 2 Comparative analysis of the methods used to determine the prevalence of mistreatment and its effects on medical students.
| Authors | Studied population | Main analyzed consequences | Method | Sample (S) /Response rate (Rr) | Prevalence |
|---|---|---|---|---|---|
| Shochet RB et al.13 (2013) | Fourth-year medical students from 1 school in the United States | Impact level on learning | Cohort survey using a questionnaire developed by the authors | S: 119 Rr: 71% | 42% |
| Cook AF et al.14 (2014) | Third-year medical students from 24 schools in United States | Burnout | Cross-sectional survey using a questionnaire + a validated two-item version of the Maslach Burnout Inventory | S: 919 Rr: 61% | ~70% |
| Wilkinson J et al.15 (2006) | Students from all medical schools in New Zealand | Both negative and positive consequences for mental health and quality of life | Cross-sectional survey using a questionnaire developed by the authors | S: 1660 Rr: 83% | 68% |
| Gan R, Snell L16 (2014) | Final-year medical students from 1 school in Canada | Suboptimal learning experiences | Qualitative descriptive study with focal group interviews + a questionnaire with open-ended questions developed by the authors | S: 174 Rr: 23% | 90% |
| Heru A et al.17 (2009) | Third and fourth-year medical students from 1 school in the United States | Symptoms of posttraumatic stress | Cross-sectional survey using a questionnaire developed by the authors + the revised Impact of Event Scale | S: 91 Rr: 78% | 73% |
| Owoaje ET et al.18 (2012) | Final-year medical students from 1 school in Nigeria | Only negative consequences involving mental health, quality of life, social relationships, and academic performance | Cross-sectional survey using a semi-structured questionnaire developed by the authors | S:269 Rr: 100% | 98% |
| Hardeman RR et al.19 (2016) | Undergraduate medical students from 49 schools in the United States | Depression symptoms | Longitudinal web-based survey using a questionnaire developed by the authors + PROMIS Emotional Distress - Depression short-form | S: 5823 Rr: 79% (in the first approach) Rr: 64% (in the final approach) | 95% (in the final approach, when students were in their final year) |
| Acik Y et al.20 (2008) | Residents from 7 hospitals in Turkey | The victim’s immediate reactions to the experience | Cross-sectional survey using a semi-structured questionnaire | S: 2442 Rr: 70% | 68% |
| Xie Z et al.21) (2017) | Undergraduate medical students from 1 school in China | Only negative consequences involving quality of life and career planning | Cross-sectional survey using a questionnaire developed by the authors + the Short Form-36 (SF-36) Scale Testing Quality of Life | S: 180 Rr: 87% | 30% |
| Peres MFT et al.22 (2016) | Undergraduate medical students from 1 school in Brazil | The way students perceive their course and professional choice | Cross-sectional survey using a questionnaire developed by the authors | S: 1072 Rr: 31% | 92% |
| Nagata-Kobayashi S et al.5 (2009) | Residents from 37 hospitals in Japan | Both negative and positive effects on mental health, quality of life and work performance | Cross-sectional survey using a questionnaire developed by the authors | S: 619 Rr: 57% | 85% |
| Rademakers JJDJM et al.23 (2008) | Medical internship students from 2 schools in Netherlands | Well-being and “professional” performance | Cross-sectional survey using a questionnaire developed by the authors | S: 311 Rr: 73% | 20% (only rated sexual harassment) |
| Nagata-Kobayashi S et al.24 (2006) | Fifth and sixth-year medical students from 6 schools in Japan | Only negative effects on mental health, quality of life and academic performance | Cross-sectional survey using a questionnaire developed by the authors | S: 559 Rr: 49% | 68% |
| Frank E et al.11 (2006) | Undergraduate medical students from 16 schools in United States | Only negative effects on mental health and quality of life | Longitudinal survey using a questionnaire developed by the authors | S: 2884 Rr: 80% (in the first approach) Rr: 48% (in the final approach) | 85% (in the final approach, when students were in their final year) |
| Maida AMS et al.25 (2006) | Undergraduate medical students from 1 school in Chile | Only negative effects on mental health and quality of life | Cross-sectional survey using a questionnaire developed by the authors | S/Rr: not described; 757 students participated | 91% |
| Gagyor I et al.26 (2012) | Undergraduate medical students from 1 school in Germany | Only negative effects on mental health | Cross-sectional survey using a questionnaire developed by the authors | S: 1222 Rr: 32% | 88% |
| Scott KM et al.27 (2015) | Medical students attending the final clinical-based training from 2 schools in Australia | The way students perceive their professional choice and evaluate their academic performance | Cross-sectional survey using a questionnaire developed by the authors | S: 151 Rr: 97% | 51% |
| Olasoji HO10 (2018) | Fourth-year medical students from 1 school in Nigeria | Negative effects on well-being and positive or negative effects on academic performance | Cross-sectional survey using a questionnaire + semi-structured interview developed by the author | S: 52 Rr: 90% | 85% |
| Puranitee P et al.28 (2019) | Pediatric residents from 1 hospital in Thailand | Burnout | Cross-sectional survey with a mixed-method design: Maslach Burnout Inventory, the Postgraduate Hospital Educational Environmental Measure (PHEEM), Work-Related Quality of Life scale (WRQoL) + an individual interview | S: 42 Rr: 97% | 51% |
| Hu YY et al.29 (2019) | Residents from 262 surgical residency programs in the United States | Burnout and suicidal thoughts | Cross-sectional survey using a questionnaire developed by the authors | S: 7464 Rr: 99% | 50% |
DISCUSSION
Training to become a physician and the practice of Medicine are activities that cause a significant amount of stress for individuals. Common sources of stress include negative aspects of the learning environment, heavy workloads, lack of time, competition among colleagues, financial concerns, health issues, and peer/faculty relations are some of most common social and environmental challenges faced by medical students around the world30. Several studies12),(30)-(32 indicate that these stressors have significant effects on individuals and that a significant percentage of medical students reports anxiety and/or depression symptoms in response to stressors. Why should another stressor be embedded into this training?
The frequency of mistreatment, harassment, and other forms of aggression in medical school, despite the efforts to mitigate them, remains high. Since 2004, two main reasons have been suggested to explain it33. First, the existence of strongly hierarchical relationship patterns and a medical culture that permeates teaching and learning relationships, perpetuating mistreatment situations as “rites of passage”. Olasoji’s survey10 pointed out that almost half of the studied sample did not report mistreatment incidents because they thought they were not important enough to be reported and considered them as inherent to medical training. The second is related to the low success rates of implemented strategies to reduce inappropriate attitudes in the academic environment. This same survey showed that the majority (66.7%) of students who reported a “toxic” experience felt neutral to the outcome of reporting. Besides that, Wilkinson et al.15, alert to the possibility of the existence of an abuse cycle, whereby medical students who have been abused become the perpetrators in the future.
This study made it possible to reaffirm that mistreatment continues to occur very frequently and that the impacts resulting from inappropriate behaviors in the learning environment can move from social, mental, performance-related harm to long-term professional impairment. It was also noted that most of the surveys based their data collection methodology on the use of questionnaires and/or interviews.
According to Lakatos34, the research success depends on the researcher’s ability to correctly choose the appropriate method for the subject they wish to research. The use of questionnaires and the filling out of validated scales represent established methods in the analysis of mistreatment situations in the academic environment. They certainly have several strengths, which should be highlighted, such as the possibility that the participant has to respond at an appropriate moment for themselves and the possibility of maintaining anonymity. However, methodological weaknesses can also be raised. Prodanov35 states that questionnaires cannot suggest or induce responses. It was found that some questionnaires11),(18 addressed the impacts caused by mistreatment by directing answers to negative effects, giving the respondent no other choice of response. Only in the most recent studies, such as the one by Olasoji10, answers involving possible “positive” aspects were added, and what could have been considered by many authors as not possible so far, surprisingly pointed out that 37.5% felt the “toxic” practice was useful for learning and made them stronger.
Andrade36 warned that in surveys using questionnaires only, where you cannot have an interviewer present, answers can be biased, leading to an apparent uniformity. That can happen because of the difficulty some respondents may have to understand some questions. The data obtained from most articles13),(22),(27 that constituted this brief review result from questionnaire analyses only, without the association of a subsequent interview that would allow the participant to solve any type of doubt that arose during the filling out of the questionnaires, or to expose any type of feelings that they were unable to explain when completing the standard questionnaire. And here, it is worth mentioning that the impacts generated by any type of mistreatment represent a complex type of data to be collected, which can vary a lot, whether regarding the affected area or its intensity, as well as variations from individual to individual.
Although it does not represent the majority, some authors10),(16),(28 improved their research by associating questionnaires with interviews when collecting data. However, this is a sensitive issue, and several characteristics of interviewing techniques could also generate bias in the obtained results, but in a different way: the impossibility of anonymity, providing less freedom and security related to the answers and higher risk of bias due to the interviewer’s influence. Lack of anonymity when approaching such a subject can intimidate students into participating and/or giving actually true answers. In the study by Gan and Snell16, the participation rate was only 23%. Over the past few decades, several authors15),(33),(37 pointed out that students do not report mistreatment because they fear victimization or have concerns related to potential repercussions in performance evaluation.
Furthermore, for the situation in question - impacts caused by a hostile academic environment - not knowing the circumstances in which questionnaires or scales were filled out, makes it difficult to control and verify the real extent of the damages caused versus those reported by the students. The cross-sectional nature of surveys using questionnaires, scales or interviews increases this possible bias. Some students, depending on the period of time that elapsed between the incidents and participation in the survey, may have already overcome the situation and, thereby, minimize the damage caused by them. Others, in contrast, in the absence of adequate social support that surrounds them and having low coping capacity, can maximize the losses. In one way or another, the retrospective nature of the collected data limits the available information, and the memory recall of unpleasant situations is often faulty and subject to various hindsight biases38.
Some authors11),(19 have proposed a longitudinal survey, with questionnaires being applied at two or more moments, and theoretically, this could minimize the bias of a cross-sectional analysis. However, invariably, these same articles faced the difficulty in maintaining good response rates, as they tend to decline throughout the study.
Besides that, studies always benefit from the use of different methodologies, whatever the area of interest is. The use of simulation could be a methodological alternative that would avoid many of the weaknesses pointed out so far, especially when determining the immediate damage from mistreatment situations in the learning environment (What actually happens to the student at the moment of the mistreatment?; Are learning and performance impaired?).
Riskin et al.39),(40 have already proven the usefulness of simulation for this type of research by conducting studies that aimed to assess the impact of rudeness on the performance of NICU (Neonatal Intensive Care Unit) medical teams. During training workshops, some teams were randomly assigned to an exposure to rudeness. In both surveys, they showed that rude attitudes had deleterious effect on the teams’ performance. Diagnosis and intervention, information sharing, workload, help, and communication were affected.
Setting up scenes of mistreatment in a simulation environment would provide prospective and recorded observation in a nonbiased fashion, typically using audio and video capture. Additionally, some other parameters could be monitored for further analysis, such as heart rate variability, facial and behavioral analysis, and assessment of the proposed task performance. They would be of great value to study with a little more depth the real effects of the stress caused by mistreatment in the academic environment.
It’s also necessary to make a very pertinent caveat when discussing the general belief that individuals learn better from stressful events, especially when the source of stress is mistreatment. According to Christianson41 the information of an event to be remembered will be retained very well if the event itself is the cause of the individual’s stress response. If the stress is caused by something peripheral to the information to be remembered, the consolidation of that information will not be improved. So, it is possible to infer that a student who feels stressed during a class where they are learning how to intubate a patient, for example, due to the presence of the teacher’s intimidating or abusive attitudes, they may develop a strong memory of the teacher’s attitudes and actions, but the memory they will have of the class itself, and of the associated essential learning points is unlikely to be improved.
Therefore, simulation would allow differentiating environments where the student must perform a certain action under intense pressure and stress because their patient’s life is at risk from those in which frequent abuse and verbal aggression occur, showing that such attitudes are unnecessary and closely related to learning impairment. Perhaps, it will help to end years of a hierarchical culture that confounds these concepts and postulates these attitudes as necessary for medical training.
CONCLUSIONS
Based on 3 important considerations, it is clear that a new approach is needed to study the impact of a hostile learning environment on students: 1. The prevalence indicated in the majority of the studies continue to show worryingly high rates of mistreatment of medical students; 2. Sufficient documentation already points out that mistreatment to students can result in a wide range of negative outcomes, both in the short and long-term; 3. This review allowed the identification of some methodological weaknesses of studies carried out in area to date.
For future studies, the simulation of learning scenarios showing inadequate teachers’ behaviors must be effectively put into practice in order to assess their effects on the students.

