











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
The pandemic caused by the new coronavirus (SARS-CoV-2), has led to major social changes and also changes in the operations of various economic and commercial sectors of society1. Due to the high contamination rate of SARS-Cov-2 and its associated high number of cases, local authorities decreed the closure of universities and schools, which has forced these institutions to come up with innovative solutions for the continuation of their activities. Therefore, new technologies are being increasingly used by medical training centers and their students’ performance with the use of these technologies point to an inevitable renewal in medical education2.
In recent decades, technological advances have provided new ways of accessing knowledge. A wide variety of innovative teaching tools and devices are now available to optimize learning, making it possible to have classes and teaching support materials available online, which can be repeatedly used by the students. Another innovation is the application of exams and questionnaires through forms, which are also sent remotely. Lastly, it is also possible to have videoconferences in which the teacher can interact with students in real time3. E-Learning has proven to be fundamental and a successful strategy for medical schools in countries with limiting factors for face-to-face teaching, such as resources, as well as the availability of specialists and educators4.
In 2015, the World Health Organization (WHO) released a report in which 33 studies analyzed the level of knowledge acquired by the students for both e-learning and traditional face-to-face teaching. The results showed that 11 (33%) of those studies included in the report demonstrated a significant gain in knowledge with e-learning, when compared to the traditional face-to-face method; 19 (58%) did not find a statistically significant difference between the two types of teaching; and 2 (6%) showed mixed results, with variations according to the knowledge indicator used5.
Few studies have been carried out to prove the effectiveness of online teaching of practical skills and medical procedures in medical schools. However, the effectiveness of theoretical teaching through e-learning has been previously demonstrated6),(7. In order to establish a more effective approach to teaching anesthesiology to residents, a group of researchers proposed that face-to-face classes should be solely interactive, with dynamic discussions of clinical cases8. To do so, the students would have to acquire a previously established knowledge, which would then be consolidated in the classroom. In this context, e-learning may prove to be a means of providing adequate theoretical content to students, so that they can optimize their use in their practical and face-to-face activities.
One of the main missions of academic medical centers is to train qualified medical professionals, able to diagnose conditions, prescribe medications and take appropriate measures for their patients. In these centers, specialized professionals are responsible for the transmission of knowledge to the students. However, being an expert is not the only qualification necessary for teaching to be carried out efficiently; it is essential that the teachers have didactic competence and know how to use tools capable of contributing to greater student learning9.
In addition, the impact of e-learning is also present economically-wise. A previous research found that the blended learning approach costs about 24% less than face-to-face teaching, without considering any transition costs10. The existence of several studies that prove the effectiveness of distance learning and its optimization in learning, considering the current situation related to the COVID-19 pandemic, contributes to the development of new teaching strategies.
The aim of this study is to assess both the impact and level of satisfaction amongst undergraduate medical students of the online teaching of theoretical anesthesiology as an alternative method to face-to-face teaching due to the difficulties imposed by the COVID-19 pandemic.
METHODOLOGY
This is an observational, cross-sectional study, approved by the Research Ethics Committee of Universidade Federal de Sergipe (UFS). Student selection was carried out by voluntary enrollment through the Integrated System of Management and Academic Activities (SIGAA, Sistema Integrado de Gestão e Atividades Acadêmicas) belonging to UFS. Sixty-one students enrolled in the medical program at the Federal University of Sergipe, in the Aracaju campus (Urban) and in the Lagarto campus (Rural), who enrolled in the extracurricular, non-mandatory project “E-learning of Theoretical Anesthesiology” were included in the research. Participation in this research was voluntary and the participant had full autonomy to decide to withdraw their participation at any time, without any consequences.
The method consisted of conducting online classes, taught by a specialist using the Microsoft Teams platform (Microsoft Corp, Redmond, WA), in which the following topics were covered in 8 modules: surgical anesthetic risk and pre-anesthetic assessment (module 1), basic life support in cardiorespiratory arrest (module 2), advanced life support in cardiorespiratory arrest (module 3), anesthesia inhalation systems (module 4), ventilatory assistance (module 5), venous and inhalation anesthetics (module 6), neuromuscular blockers in anesthesiology (module 7) and neuraxial blocks (module 8). Each topic was taught in two subsequent classes, with a one-week interval, so that the topics could be discussed in subgroups supervised by monitors who are part of the course coordination.
The Informed Consent Form (ICF) and the expectation questionnaire about the e-learning course were answered through the Google Forms platform (Google LLC, Mountain View, CA). At the end of the course, the satisfaction questionnaire was sent and answered by the students through the same platform. The personal assessment questionnaire was adapted from a previously applied questionnaire found in the literature11. The following items were graded by students on a scale from 1 (very low expectations / very dissatisfied) to 7 (very high expectations / very satisfied): course design, coordination, faculty and tutors, program schedule, available materials, work methodology, evaluation system, support services and technological infrastructure.
Each topic was discussed in two classes, the first being the theoretical content covered in an expository way and the other, discussions of clinical cases with stimulated interaction among the participants. The students were subdivided into six subgroups that had support from a monitor. Each subgroup held a virtual meeting between each module’s classes to discuss and answer questions about the clinical cases to be discussed in the upcoming class. The evaluation of the impact of the classes took place through questionnaires with 10 questions. The pre-test questionnaire was made available 20 minutes before the first class of each module, aiming to assess the participants’ previous level of knowledge. After the end of the module, the questionnaire was reapplied, aiming to assess whether there was significant progress in performance after the performed intervention.
The categorical variables were described by means of absolute frequency and relative percentage. Continuous variables were described using means, standard deviations, maximum and minimum values. The hypothesis of adherence of continuous variables to the normal intra-group distribution was tested using the Shapiro-Wilks test, which was not confirmed. Hence, the Wilcoxon test (two groups) was used to check the hypothesis of equality of central tendency measures. The adopted level of significance was 5% and the software “Statistical Package for the Social Sciences” - SPSS 22.0 was used for the statistical analysis.
One of the challenges faced during the research was that of encouraging students to stay in the course until the end, since some had family and friends affected by COVID-19, a delicate and difficult-to-handle situation. Another obstacle was the partial return of face-to-face classes, which made most of the students end up with a busy schedule, which we inferred to have been one of the factors responsible for the reduction in the number of questionnaires answered in the second half of the course. In addition, it should be noted that all preventive measures against SARS-COV 2 infection were taken, with no meetings or face-to-face classes taking place during the course.
RESULTS
Participants’ profile
In general, 61 undergraduate medical students accepted to participate in the study and answered the questionnaires, with an overall response rate of 83.2% (8120 responses out of 9760 possible ones). Student participation was similar in terms of gender, with 52.46% female and 47.54% male participants. Most were aged between 20 and 25 years old (91.80%) and were in the fourth year of the undergraduate medical school (62.29%). Less than 20% of the participants were graduating from a rural campus and only 32.79% of students said they had chosen anesthesiology for their medical residency. Among the possible reasons for choosing to take a course with a distance learning methodology, the development and consolidation of knowledge was the criterion most often chosen by the participants (91.80%), followed by the development of skills for professional application (80,33%) and the space flexibility due to the lack of displacement (75.41%). The selection criteria that were least cited by the participants included curiosity about the operation of distance learning (24.59%), conciliation with professional life (26,23%) and conciliation with personal and family life (22.95%). Table 1 summarizes the social and demographic characteristics of the participants.
Table 1 Distribution of the students according to personal and sociodemographic variables
| Variable | N | % |
|---|---|---|
| Sex | ||
| Male | 29 | 47.54 |
| Female | 32 | 52.46 |
| Age range | ||
| 20-22 | 28 | 45.90 |
| 23-25 | 28 | 45.90 |
| >25 | 5 | 8.20 |
| Semester | ||
| 6 | 1 | 1.64 |
| 7 | 23 | 37.70 |
| 8 | 15 | 24.59 |
| 9 | 15 | 24.59 |
| 10 | 5 | 8.20 |
| 11 | 2 | 3.28 |
| Campus | ||
| Urban | 51 | 83.61 |
| Rural | 10 | 16.39 |
| Considering anesthesiology as an option for residency | ||
| Yes | 20 | 32.79 |
| No | 41 | 67.21 |
| Reasons why students choose to take the e-learning course | ||
| Space flexibility | 46 | 75.41 |
| Time flexibility | 37 | 60.66 |
| Fitting with professional life | 16 | 26.23 |
| Knowledge development/consolidation | 56 | 91.80 |
| Developing skills to ally professionally | 49 | 80.33 |
| Appreciation and interest in the specialty | 32 | 52.46 |
| Fitting with personal/family life | 14 | 22.95 |
| Personal improvement | 21 | 34.43 |
| Profissional improvement | 39 | 63.93 |
| Expectations of advantagens in e-learning | 20 | 32.79 |
| Impossibility to attend in person | 22 | 36.07 |
| Cost reduction | 22 | 36.07 |
| Participation in a different learning experience | 38 | 62.30 |
| Curiosity about the operation of the e-learning | 15 | 24.59 |
| Autonomy in learning | 34 | 55.74 |
| Extra curricular certificate | 34 | 55.74 |
Source: Research Data, 2020. Subtitles: N - absolute frequency. % - relative frequency.
Questionnaires and learnership
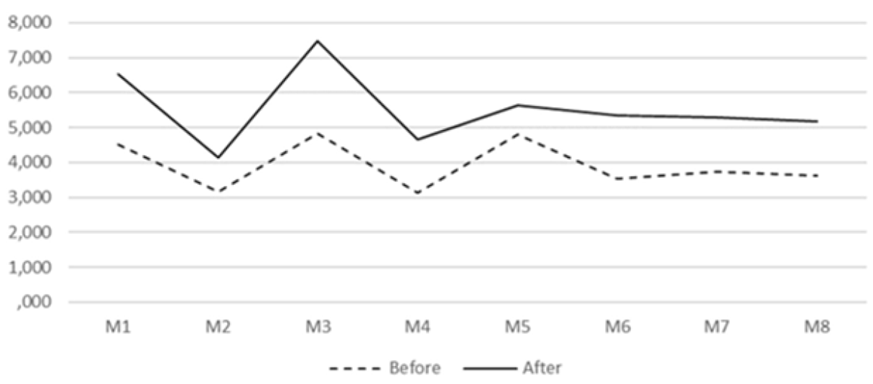
Of the 61 participants, only 36 answered all 16 questionnaires related to the 8 modules of the course. All questionnaires applied after the classes in the respective module showed a significant increase (p<0.05) in the average of correct answers when compared to the answers obtained before the classes, as shown in Table 2 and in Graph 1. After adding the questionnaires applied before and after meeting with the students, 812 were filled out of a total of 976; there was a significant increase of 41.61% in the average of correct answers (3.94 vs. 5.57; p <0.001). When considering only the responses of the participants who completed all the questionnaires, it was observed that there was no difference in the increase of the average between the different modules of the course (p >0.05).
Table 2 Comparison between the results of tests performed before and after each module
| Mean Score | |||||
|---|---|---|---|---|---|
| Modules | Before | After | After: Before | P-value | |
| Module 1 | N | 61 | 61 | ||
| Minimum | 1 | 9 | |||
| Maximum | 2 | 10 | |||
| Mean | 4.50 | 6.54 | 1.45 | <0.001 | |
| Std. Deviation | 1.66 | 1.94 | |||
| Module 2 | N | 59 | 59 | ||
| Minimum | 1 | 1 | |||
| Maximum | 7 | 8 | |||
| Mean | 3.16 | 4.15 | 1.31 | 0.001 | |
| Std. Deviation | 1.29 | 1.94 | |||
| Module 3 | N | 57 | 57 | ||
| Minimum | 1 | 10 | |||
| Maximum | 1 | 10 | |||
| Mean | 4.82 | 7.49 | 1.55 | <0.001 | |
| Std. Deviation | 2.12 | 2.13 | |||
| Module 4 | N | 54 | 54 | ||
| Minimum | 1 | 1 | |||
| Maximum | 6 | 9 | |||
| Mean | 3.13 | 4.67 | 1.49 | <0.001 | |
| Std. Deviation | 1.37 | 2.18 | |||
| Module 5 | N | 48 | 48 | ||
| Minimum | 1 | 2 | |||
| Maximum | 8 | 9 | |||
| Mean | 4.81 | 5.64 | 1.17 | 0.006 | |
| Std. Deviation | 1.39 | 2.09 | |||
| Module 6 | N | 46 | 46 | ||
| Minimum | 0 | 0 | |||
| Maximum | 7 | g | |||
| Mean | 3.54 | 5.35 | 1.51 | <0.001 | |
| Std. Deviation | 1.54 | 2.28 | |||
| Module 7 | N | 45 | 45 | ||
| Minimum | 0 | 1 | |||
| Maximum | 7 | 10 | |||
| Mean | 3.73 | 5.29 | 1.42 | <0.001 | |
| Std. Deviation | 1.51 | 2.46 | |||
| Module 8 | N | 36 | 36 | ||
| Minimum | 1 | 1 | |||
| Maximum | 7 | 8 | |||
| Mean | 3.61 | 5.17 | 1.43 | <0.001 | |
| Std. Deviation | 1.69 | 1.76 | |||
| General | N | 406 | 406 | ||
| Minimum | 0 | 0 | |||
| Maximum | 10 | 10 | |||
| Mean | 3.94 | 5.57 | 1.41 | <0.001 | |
| Std. Deviation | 1.72 | 2.31 | |||
Abbreviations: Std. Deviation - Standard Deviation. N - Number of tests performed. Wilcoxon’s test.
Expectation and satisfaction indexes
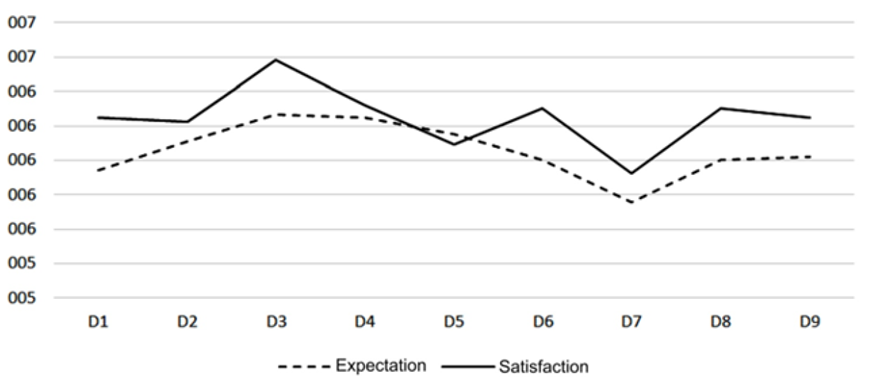
Table 3 and Graph 2 compare the responses of the participants regarding their expectations in relation to the course with the levels of satisfaction obtained at the end of the course. Out of the 61 participating students, 86.88% answered the quality assessment questionnaires. Only in variables 3 and 6, which analyzed the students and the methodology, respectively, there was a significant increase in satisfaction rates in relation to expectations (6.26 vs 6.58; 6.00 vs 6.30; p <0.05). Upon analyzing the variables individually, there was no significant decrease in the levels of satisfaction in relation to the expectations created before the beginning of the course. In general, satisfaction levels significantly exceeded the expectation levels (6.25 vs 6.05; p <0.001).
Table 3 Comparison between the levels of expectation and satisfaction of students regarding the e-learning course
| Mean Score | |||||
|---|---|---|---|---|---|
| Variables | Expectation | Satisfaction | Expectation: Satisfaction | P-value | |
| Design | N | 53 | 53 | ||
| Minimum | 4 | 3 | |||
| Maximum | 7 | 7 | |||
| Mean | 5.94 | 6.24 | 1.05 | 0.057 | |
| Std. Deviation | 0.95 | 0.94 | |||
| Coordination | N | 53 | 53 | ||
| Minimum | 4 | 4 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.11 | 6.23 | 1.02 | 0.418 | |
| Std. Deviation | 0.89 | 0.93 | |||
| Teacher and tutors | N | 53 | 53 | ||
| Minimum | 3 | 3 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.26 | 6.58 | 1.05 | 0.024 | |
| Std. Deviation | 0.96 | 0.82 | |||
| Program schedule | N | 53 | 53 | ||
| Minimum | 4 | 2 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.24 | 6.32 | 1.01 | 0.66 | |
| Std. Deviation | 0.83 | 1.01 | |||
| Materials | N | 53 | 53 | ||
| Minimum | 4 | 4 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.15 | 6.09 | 0.99 | 0.661 | |
| Std. Deviation | 0.82 | 1.00 | |||
| Methodology | N | 53 | 53 | ||
| Minimum | 4 | 3 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.00 | 6.30 | 1.05 | 0.039 | |
| Std. Deviation | 0.83 | 0.89 | |||
| Evaluation system | N | 53 | 53 | ||
| Minimum | 4 | 3 | |||
| Maximum | 7 | 7 | |||
| Mean | 5.75 | 5.92 | 1.03 | 0.346 | |
| Std. Deviation | 1.00 | 1.09 | |||
| Support services | N | 53 | 53 | ||
| Minimum | 4 | 3 | |||
| Maimum | 7 | 7 | |||
| Mean | 6.00 | 6.30 | 1.05 | 0.094 | |
| Std. Deviation | 0.98 | 0.99 | |||
| Technological infrastructure | N | 53 | 53 | ||
| Minimum | 4 | 3 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.02 | 6.24 | 1.04 | 0.185 | |
| Std. Deviation | 0.86 | 0.94 | |||
| General | N | 477 | 477 | ||
| Minimum | 3 | 2 | |||
| Maximum | 7 | 7 | |||
| Mean | 6.06 | 6.25 | 1.03 | <0.001 | |
| Std. Deviation | 0.92 | 0.97 | |||
Abbreviations: Std. Deviation - Standard Deviation. N - Number of responses. Wilcoxon’s test.
DISCUSSION
As of February 2021, more than 2 million COVID-19 deaths have been recorded worldwide, with 110 million confirmed cases12. Even with the development of vaccines, several countries, including Brazil, have faced difficulties in acquiring and distributing the necessary doses to vaccinate the entire population13. In this scenario, several academic institutions persisted with an exclusively remote or hybrid teaching methodology, the latter consisting of face-to-face practical classes and theoretical classes conducted online14. To measure the applicability of this system, it is necessary to jointly assess the level of satisfaction and, consequently, adherence, as well as the impact on the participants’ theoretical knowledge.
The students’ adherence to the alternative teaching method and activities related to its methodology can be considered high, with an overall participation of 83.2%, represented by the answers obtained through questionnaires applied weekly. Of the 61 students enrolled in the course, 59.02% answered all questionnaires. Previous studies using questionnaires to assess knowledge acquisition during distance learning have shown a response rate between 41.18% and 65.3%4),(7),(15.
Students’ attendance can be linked to different variables. Low level of involvement, demotivation, limited flexibility, high levels of anxiety and stress, lack of self-discipline and poor interactions between students and facilitators can limit the learning and motivation process, reflecting the degree of participation throughout the project16. However, even with these factors, this study suggests that it is possible to have good student adherence and participation in distance learning conducted online.
When assessing the participants’ improvement regarding the theoretical content approached through the e-learning method, a significant increase of 41.37% was found in the average of correct answers. A prospective study, in which an online course consisting of six sessions on Evidence-Based Medicine given to 84 students, was assessed by means of questionnaires before and after the completion of the exams showed similar results. Amongst the participants involved in the course, 48 answered both questionnaires and there was an increase of 57.14% in the average of the post-course questionnaire (p <0.001)7. The methodological similarity between the present study and the aforementioned ones, as well as the equivalence in the good results obtained, allows the inference of the good effectiveness of the method. In Ethiopia, the teaching of anesthesiology by distance learning to residents was evaluated and obtained a significant increase in the overall average after the methodological intervention performed (54.5% vs 83.6%)4. This result is in line with that obtained in this study, and the content covered in both studies may have been responsible for this statistical similarity.
A longitudinal study, conducted in Brazil, sought to assess the increase in knowledge of residents of gynecology and obstetrics after taking an online course on sexuality during pregnancy. Tests were applied before and after the course and an increase of 36.36% (p <0.0001) in the average of the participants was observed15. Thus, with the statistical similarity obtained between different studies with a similar methodology, it seems that the e-learning methodology for the teaching of theoretical medical content is effective.
When comparing these results to the traditional teaching method, medical students at King Abdulaziz University, in Jeddah, Saudi Arabia, assessed that e-learning was able to replace classical learning on campus during the Covid-19 pandemic17. The uniform learning corroborates the success of this method and it can be satisfactorily added to the traditional form of teaching for medical students. When compared to each other, there was no difference between the increases in the averages of the different modules, suggesting that the proposed methodology took place uniformly throughout the course.
Regarding the participants’ acceptance, the expectation questionnaire about the course applied before the start of classes had a general average of 6.05, out of a maximum of 7, and the satisfaction levels exceeded the expectation levels, obtaining an average of 6.25. In a study carried out in Jordan, the general satisfaction rate in medical distance education was 26.8%, it was also observed that this rate was significantly higher in students with previous experience in distance education during medical training and with the instructor’s experiences and interactions14.
In Colombia, aiming to increase the knowledge of pediatricians and pediatric residents on rheumatological disorders in children, a hybrid course was held, with four online modules and two face-to-face meetings. Of the 41 participants in the course, 90.24% completed all online modules and 80.48% attended the final face-to-face session, with 94% of the participants reporting they felt an increase in medical knowledge and skill after the course, whereas 88% said they were satisfied with the teaching strategy used18. The significant increase in the level of knowledge and the high levels of satisfaction, corresponding to that found in the present study, contribute to the definition of e-learning as an effective method for medical teaching, which can be used as a complementary tool for the optimization of the current model, with exclusively in-person classes.
CONCLUSION
The present study had distance theoretical anesthesiology teaching as its main focus and its results showed considerable knowledge gain on the part of the participants and good acceptance of the used method, corroborating other studies carried out around the world. Finally, this research was not intended to show the superiority of one method over another but rather to be used as a model to demonstrate the effectiveness of the use of different technologies to support the training of future doctors, even in periods of time when it is impossible to have regular face-to-face meetings, such as during the COVID-19 pandemic.

