











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
The COVID-19 pandemic can be considered a traumatic event, due to the potential to trigger psychological distress, causing reactions such as extreme fear of contagion, anger, doubts, insomnia, malaise, in addition to the onset or worsening of mental disorders such as anxiety, depression, acute stress reactions and post-traumatic stress disorder. It may also be associated with risk behaviors, such as tobacco and alcohol consumption and an increased risk of suicide1)-(4. Given this scenario, several groups are being considered more susceptible to the psychosocial consequences of the pandemic, and among them, medical students5.
Considering that these students comprise a significant part of the workforce of health systems, it is necessary to reflect on the quality and homogeneity of their training, as well as the maintenance of their mental health, which can be compromised by the current health emergency5. Experiencing a moment of uncertainty, with potential professional implications for these students, places them in a position of psychological vulnerability. Moreover, there is fact that several studies, prior to the pandemic period, suggested that medical students are at high risk of developing mental health problems. A meta-analysis involving studies from 43 countries identified a 27.2% prevalence of depression or depressive symptoms and an 11% of suicidal ideation rate among medical students6.
When confronted with large-scale pandemic and disaster situations, one of the recommendations for coping, according to international protocols, involves offering alternative service channels (applications, websites, telephone)7. In this scenario, many countries have adopted telemental health service as a resource, which has a distinctive capacity to offer support, while maintaining social distancing. The telemental health service consists of the use of information and communication technologies (ICTs), such as phone calls, emails, videoconferences and electronic consultation systems, to provide remote health care8.
Among the potential benefits of teleservice is the possibility that communication technologies offer to connect people and strengthen their support network, which can bring benefits to the prevention of psychological distress, especially in situations of social distancing, as in the case of the COVID-19 pandemic9. Other positive factors include the saving of resources, the possibility of having access to specialists in distant regions, the collaboration of more experienced professionals with less experienced ones in emergency situations and avoiding patient displacement8),(10),(11. Some advantages are also reported, such as: viral transmission limitation and protection of people belonging to groups considered at risk; increased understanding of family dynamics; improved access to patients who have conditions that interfere with their ability to leave the home; increased privacy and a sense of security by reducing the need to go to a mental health facility; improvement in the organization of the medical agenda, as it facilitates the scheduling of appointments and decreases the rate of no-shows. On the other hand, there are some limitations related to technological aspects (such as increased chance of interruptions due to technical failures), limited access of some population groups to this type of care (elderly people, people who do not have access to technology, people with visual or hearing impairment, and/or migraine sufferers) and also the absence of physical contact, which prevents the performance of the necessary physical examination in some conditions, hinders the use of non-verbal communication and can harm the doctor-patient relationship12.
Before the onset of the pandemic, increasing investments and research in teleconsultations were observed worldwide, especially in England and the United States8. The teleconsultations could be carried out as an additional, alternative or partially substitutive to in-person treatment and, in general, required a first face-to-face consultation8. In the context of the pandemic, several countries have used ICTs for patient screening and monitoring, follow-up of chronic diseases, counseling and therapies (such as telerehabilitation for children and the elderly)10. Regarding mental health, teleconsultations can be carried out to monitor individuals previously treated at the service, but also to provide support to new cases that have emerged in the context of the pandemic. Some countries such as China and Australia have offered psychoeducation, counseling, supervision and training services through online platforms, targeting front-line professionals, patients with COVID-19 and their family members13.
In Brazil, the Telehealth Brazil Networks (Telessaúde Brasil Redes) program, created in 2011 by some universities in partnership with the Federal Government to promote the integration of Family Health teams with university referral centers in teleservice, thus promoting the qualification of the assistance in primary care, is highlighted14. Another example is the TelePsy Project, offered by the Ministry of Health in partnership with Hospital de Clinicas de Porto Alegre (HCPA). This project constitutes a free service to health professionals working in the front line of COVID-19 and has the support of psychology and psychiatry professionals15.
With the pandemic onset, the expansion of teleassistance services and their regularization became urgent. The Ministry of Health published Ordinance N. 467/2020, which provides for telemedicine actions in the implementation of measures to fight the pandemic, under exceptional circumstances, authorizing its practice in the public and private spheres16. Then, Law N. 13,989/2020 was approved, which authorizes the use of telemedicine in any health care activities in Brazil, including teleconsultation, for as long as this health emergency lasts17. In this context, the Federal Council of Medicine (CFM, Conselho Federal de Medicina) recognized, through Official Letter N. 1756/2020, the possibility and ethicality of using telemedicine, “in exceptional circumstances and for as long as the actions to fight COVID-19 contagion last” (2020, p.1), in the modalities of teleorientation, telemonitoring and teleinterconsultation18. The Federal Council of Psychology (CFP, Conselho Federal de Psicologia) decided, through Resolution N. 4/2020, to authorize teleconsultations for all psychologists according to some guidelines, even for those who have not yet been approved on the e-Psi platform by their Regional Councils19. The Federal Council of Social Service (CFESS, Conselho Federal de Serviço Social) released a note on professional practice during the Coronavirus pandemic, which emphasizes that, unlike the CFP, the CFESS has not yet regulated a resolution for this type of care but protects the professional autonomy of social workers to define the most adequate type of care, highlighting the exceptional circumstances during the pandemic situation that the country is facing19),(20.
Considering this scenario, this article aims to report the experience of implementing a telemental health service aimed at medical students at the Federal University of Rio de Janeiro (UFRJ, Universidade Federal do Rio de Janeiro) in the setting of the COVID-19 pandemic.
EXPERIENCE REPORT
The increase in the spontaneous demand of medical students for mental health care at the Psychiatry and Psychology Service of the Clementino Fraga Filho University Hospital (HUCFF), as well as the demand for professors from different courses at UFRJ who sought help to deal with the problems reported by several students, motivated the Dean’s Office of UFRJ to create a working group to establish a Mental Health Care Policy for UFRJ Students21. As a result of this initiative, a Service Project aimed at students of the School of Medicine of UFRJ was initiated, and put into practice in May 2018, with the support of professionals from the Psychiatry and Psychology Service of the HUCFF and the Institute for Studies in Public Health (IESC /UFRJ). As of July 2019, the project has also started to have the support of a Social Worker from HUCFF. The Psychiatric and Psychological Care Sector for students of the School of Medicine is located on the 9th floor (room 9E28) of the HUCFF and became official on 3/7/2019 through BUFRJ Ordinance N. 1022.
In mid-March 2020, with the beginning of the COVID-19 pandemic, in-person classes were interrupted at the University and, consequently, the services provided to the students. From then on, the professionals of the division, through virtual meetings, started discussing about the expansion of the restrictive measures and social isolation, which would possibly have an emotional impact on the students. Thus, it would be relevant to organize an online support proposal for students during the pandemic.
The analysis of national and international studies, the social and economic reality of a significant part of the students, the interruption of the first semester and the perspective of also missing the second semester, as well as possible family difficulties generated by social isolation, raised concerns about the triggering, the recurrence and worsening of psychological distress episodes among students, especially those with a preexisting history of mental disorders. Moreover, the pandemic could result in an increase in mental problems, especially in students with greater psychological vulnerability23.
After a meeting with the principal of the School of Medicine, a protocol for remote care was organized for students who required support during the pandemic period. Initially, a message was sent regarding the offer of online assistance to students attending the School of Medicine of UFRJ through the Integrated Academic Management System (SIGA, Sistema Integrado de Gestão Academica). Students interested in the assistance should contact the program secretary directly by email, who forwarded the student’s contacts to the professional working on the project’s available team, consisting of 5 psychiatrists, 1 psychologist and 1 social worker, with a starting weekly availability of 4 hours each.
The professional contacted the student interested in scheduling the online service, which could be carried out through different applications, such as WhatsApp, Zoom, Skype, mobile technology such as cell phones and others, according to each student’s availability. Each session lasted an average of 1 hour. During the session, the professional followed pre-established conducts to deal with traumatic events, such as guidelines for coping mechanisms (muscle relaxation, physical exercises, yoga, mindfulness) and social support24.
Initially, four sessions were planned. If necessary, the professional would extend the care for as long as necessary. In case of psychiatric emergencies, the on-call doctor at the Psychiatry and Psychology Service at HUCFF would be called. Students who needed more effective support in the social area would have the support of the social worker. This support is mainly offered to students that entered the University through the Affirmative Action Law and from other Brazilian states or other countries, such as guidelines for obtaining the benefits available at the university, through the Student Assistance policy (Figure 1). In the first half of 2018, 45.29% of the students entered UFRJ through affirmative actions from public schools, and of these, 21% were part of affirmative income actions (per capita family income below 1.5 minimum wages) and 36% were migrants25. In 2020, 200 vacancies were offered for the medical course26.
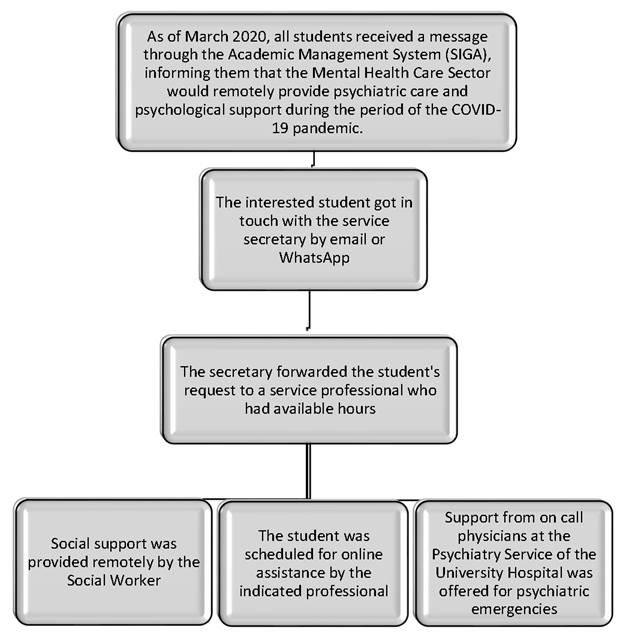
Figure 1 Flowchart of telemental health care for medical students at UFRJ during the COVID-19 pandemic.
At the end of the consultation, the professional filled out, in addition to the medical record, an Excel spreadsheet that contained sociodemographic and clinical data of all the treated cases. When necessary, such as at the prescription of psychotropic drugs, the psychiatrist followed the case together with the psychologist. The same procedure took place when the psychiatrist needed psychological support to be offered to a case. A professional from the team was responsible for monitoring data entry and the weekly release of the spreadsheet. All involved professionals participated in a weekly meeting, when cases were presented and discussed as a team and supervised by the service coordinator. The project will last for the period of time stipulated by the Dean’s Office of UFRJ for remote classes.
During remote consultations, a strong impact of the pandemic on the lives of these students was perceived. At first, the demands were characterized by the necessary adaptations to academic and social life, such as social distancing and remote teaching, which increased anxiety and depression. With the progress of the pandemic and the postponement of in-person activities, other emotional demands were added to this context: stress, irritability, frustration, loneliness, concentration difficulties, work overload and a feeling of low academic productivity, making the psychosocial support of these students essential in the reorganization of a new reality brought on by the pandemic.
DISCUSSION
The current replacement of in-person classes by remote ones has become a challenge due to the eminently practical nature of several subjects, which becomes a source of emotional overload. This fact is a dilemma, especially in the last two years of medical school (internship)27. Moreover, a significant part of these students are more vulnerable to mental problems, such as those with lower family income, who live in poor communities and with high rates of violence28)-(30. Similarly, migrants from other cities and states were, in many cases, forced to return to their states, while waiting for their return to school. Dealing with fear and insecurity, living with situations of illness, parental unemployment, and economic loss are sources of great psychological suffering31. In this context, the Department of Mental Health Care for Medical Students at UFRJ found in the telemental health service the possibility of continuing to provide care, considering that these students face unique stressors in the context of the pandemic.
The type of technology used can facilitate remote care, which was observed through the utilization of easy-to-use platforms, which teachers and students were already accustomed to. However, it should be noted that students who live in areas of greater vulnerability had difficulties in accessing these platforms, which interfered with the provision of care32. In addition to facilitating the adaptation to the technology, the previous existence of the service structure, with a team of already established professionals, made the implementation faster and its maintenance possible33.
Other indicated facilitators were the experience of professionals and familiarity with patients, achieved by the service, which included the presence of professionals who were already part of the institution, with extensive experience in mental health care33. Other aspects that contributed to the adequate implementation of the teleservice are highlighted, such as cost savings, reduced waiting time and time spent in transit for the consultation33. These points were experienced by our team, which observed cost savings, considering that the service implementation costs were low (on account of the prior existence of the structure and the type of technology used) and it was possible to reduce displacement and waiting time for services, improving accessibility and better adaptation to the extensive workload of students. Another observed important factor was the institutional support, such as that offered by the principal of the School of Medicine, which allowed the dissemination of the project through messages sent by UFRJ integrated academic management system, more comprehensively reaching the students.
Chen et al.12 (2020) indicate privacy and trust as advantages of teleservice. However, it was observed that privacy may have been compromised, mainly among the most vulnerable students, whose households have reduced physical space and it is necessary to share the same environment with other family members. The lack of privacy can interfere, for instance, with the spontaneous reporting of family problems experienced by these students.
The relationship of trust can also be facilitated by the credibility given by the students to the institution’s professionals, due to their academic knowledge in the area of mental health33. These professionals, however, are often overworked and have little time to dedicate to the care service. Although, as mentioned before, there is greater adaptability to the remote care format, the extensive workload of students can make it difficult to match their schedules with those provided by the professionals, which can hinder the creation of a bond and continuation of care.
Among the barriers for this type of service are also the patient’s health conditions33. A management difficulty was identified in psychiatric emergency situations, such as suicide attempts, despite the existence of the HUCFF emergency service, which is part of the Psychiatric and Psychological Care Sector, to which the student can be referred, if necessary.
The teleservice can also limit the doctor-patient relationship, preventing adequate non-verbal communication between them. It is possible that, during the remote care, useful expressions for the definition of diagnosis or management, such as the perception of looks, hand gestures, sitting positions, among others, are lost34),(35.
Additionally, another point that can act as a barrier to the teleservice implementation is the lack of specific training for professionals for this modality of care and the scarcity of guidelines that can help them in this process. With the advent of the pandemic, the need for adaptation meant that the remote modality was quickly adopted, but at an initial moment, making it impossible to train the team to adapt to this type of care36.
Thus, it can be observed that the teleservice, despite some limitations, constitutes an important space for listening and embracement, considering the psychosocial demands of these students, which has also been evidenced in surveys that demonstrated satisfaction both by health professionals and by patients, when this type of care is offered37),(38.
CONCLUSIONS
The implementation of the telemental health care service in Brazil is still in its initial phase and had to be carried out abruptly due to the circumstances and needs brought on by the pandemic. The same was observed at the implementation of the service, but despite the difficulties inherent in the process, the potential of technology to help the population at this critical moment is perceived, especially regarding the mental health care offered to specific groups, such as medical students.
Therefore, a window of learning opportunities is opened, together with the reconfiguration of care offers and accesses, with the potential of bringing benefits to students’ mental health care. The teleservice has to face the challenge of overcoming some barriers that hinder the access and availability of mental health care services on the university campus. However, the integration of in-person care and teleservice can improve mental health care in the period after the pandemic. The development of research is also important in assessing the acceptability and feasibility of these new technologies, aiming at expanding this type of care to other courses at UFRJ.

