










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por emailCompartilhar

 Permalink
PermalinkRevista Brasileira de Educação Médica
versão impressa ISSN 0100-5502versão On-line ISSN 1981-5271
Rev. Bras. Educ. Med. vol.49 no.1 Rio de Janeiro 2025 Epub 15-Mar-2025
https://doi.org/10.1590/1981-5271v49.1-2024-0198
ORIGINAL ARTICLE
Entrustable professional activities for family and community medicine residency in the Brazilian context
1
2
, study concept, data curation, formal analysis, investigation, methodology, project administration, writing of the original draft, review and editing of the manuscript http://orcid.org/0000-0002-2807-6256
http://orcid.org/0000-0002-2807-6256
1
, research and methodology, formal analysis, validation, review and editing of the manuscripthttp://orcid.org/0000-0002-7728-1184
1
, research and methodology, formal analysis, validation, review and editing of the manuscripthttp://orcid.org/0000-0002-5148-5517
1
, research and methodology, formal analysis, validation, review and editing of the manuscripthttp://orcid.org/0000-0002-1895-0106
2
, research and methodology, formal analysis, validation, review and editing of the manuscripthttp://orcid.org/0000-0001-7886-4384
1
, study concept, formal analysis, investigation, methodology, supervision of the project, writing of the original draft, review and editing of the manuscripthttp://orcid.org/0000-0002-2527-6500
1 Universidade Estadual de Campinas, Campinas, São Paulo, Brasil.
2 Hospital Israelita Albert Einstein, São Paulo, São Paulo, Brasil.
Introduction:
Entrustable professional activities (EPAs) describe units of professional practice of a specialty and, therefore, fundamental to be offered as training by residency programs. EPAs for residency in Family and Community Medicine (FCM) have already been described in other countries. In Brazil there is still no description of these EPAs for the specialty.
Objectives:
Develop EPAs for FCM in the Brazilian context and validate them using the Delphi technique.
Method:
FCM experts and teachers with expertise in medical education analyzed the national competency matrices for FCM residency and the EPAs previously described in other countries for the specialty. This core group formulated EPAs considering the population’s health needs, the legislation of the Brazilian Unified Health System (SUS) and the specificities of FCM training in the country. FCM specialists with experience working in medical residency were invited to form a Delphi panel to evaluate the proposed EPAs. A Content Validation Index of 80% was considered for consensus.
Results:
14 EPAs were defined by the core group. The Delphi panel consisted of a group of 24 preceptors and program supervisors, with an average length of experience as educators in FCM residency of eleven years. It took two rounds to establish the consensus and all 14 EPAs were approved.
Discussion:
Brazil has specificities related to its population and the health system organization that differentiate it from countries where EPAs for FCM have been described. There is a uniqueness in FCM training in the country, with the need to develop local EPAs. This was demonstrated by the need to formulate EPAs considering operations in health care networks, addressing vulnerabilities and health care considering the operation territory.
Conclusion:
This study describes a proposal for the development and validation of EPAs for the Family and Community Medicine residency in Brazil. The specification of these activities has the potential to support the orientation of residency programs in the specialty and reduce differences in FCM training in the country.
Keywords: Family and Community Medicine; Medical education; Medical residency
Introdução:
As atividades profissionais confiáveis (APC) descrevem unidades de prática profissional essenciais de uma especialidade e, portanto, fundamentais a serem ofertadas como treinamento por programas de residência. As APC para residência em Medicina de Família e Comunidade (MFC) já foram descritas em outros países. No Brasil, ainda não há descrição das APC para a especialidade.
Objetivos:
Este estudo teve como objetivos elaborar APC para MFC no contexto brasileiro e validá-las através por meio da técnica Delphi.
Método:
Especialistas em MFC e docentes com expertise em educação médica analisaram as matrizes de competências nacionais para residência de MFC e as APC descritas anteriormente em outros países para a especialidade. Esse grupo central formulou APC considerando as necessidades de saúde da população, a legislação do Sistema Único de Saúde (SUS) e as especificidades da formação em MFC no país. Especialistas em MFC com experiência em atuação na residência médica foram convidados para compor um painel Delphi para avaliação das APC propostas. Considerou-se para consenso um índice de validação de conteúdo de 80%.
Resultados:
O grupo central elaborou 14 APC. O painel Delphi foi composto por um grupo de 24 preceptores e supervisores de programa, com tempo médio de experiência como educadores na residência de MFC de 11 anos. Foram necessárias duas rodadas para estabelecimento de consenso, e todas as 14 APC foram aprovadas.
Discussão:
O Brasil possui especificidades relacionadas à sua população e à organização do sistema de saúde que o diferencia de países onde as APC para MFC foram descritas. Há uma singularidade na formação em MFC no país, com a necessidade de desenvolvimento de APC locais. Isso foi evidenciado pela necessidade de formular APCs considerando a atuação em redes de atenção à saúde, a abordagem de vulnerabilidades e a atenção à saúde considerando o território de atuação.
Conclusão:
Este trabalho descreve uma proposta de elaboração e validação de APCs para a residência de em Medicina de Família e Comunidade no Brasil. A especificação dessas atividades tem potencial para apoiar a orientação de programas de residência na especialidade e redução das diferenças em formação em MFC no país.
Palavras-chave: Medicina de Família e Comunidade; Educação Médica; Residência Médica
INTRODUCTION
Competency-based medical education has brought important changes to the training of residents, including the possibility of training directed to their learning needs and focuses on the outcomes of the professional practice of the student in training. In addition, it also brought improvements to the quality of care delivered to patients and allowed the description of curricula based on the needs of the health system1),(2. Competencies describe the student’s individual attributes to perform a given task in a specific context and these attributes may vary, for example, according to the student’s degree of education and the action scenario. The competencies, therefore, describe important qualities to be developed by the resident in training, but do not delimit the practical activities that should be performed by a given specialty3.
A complexity observed in the literature about competencies is the fact that they are usually presented in a textually extensive way4),(5. As an example, there is the matrix of competencies for Family and Community Medicine (FCM) residency described by the National Medical Residency Commission (CNRM, Comissão Nacional de Residência Médica) in 2019, which brings a total of 334 items to be evaluated during the two years of residency training6. These items are separated by year of training, some have repeated thematics, only increasing the level of complexity, which can make their use difficult in practice. Moreover, it is considered that competencies, as they describe attributes or qualities expected of physicians in training, can often be described in an abstract way and make it difficult for educators to evaluate the residents’ performance5.
To serve as a bridge between the residents’ competencies and professional practice, the Entrustable Professional Activities (EPAs)7 were described. While the competencies describe individual attributes of the resident in training, the EPAs describe practical and essential tasks of the specialty, which enable an inference whether the student has the competencies to work within the specialty scope5),(8.
EPAs are defined as a set of fundamental practice units that define a specialty. They may be entrusted to a resident once they have demonstrated proficiency to perform them without supervision. They are, by definition, observable activities that can be carried out independently. Because of that, they facilitate the measurement of the resident’s evolution in their practice. With a more accurate assessment of the resident’s progression, the result is an increase in the provided quality of care and an increase in the safety of patients, educators and residents9),(10.
Entrustable Professional Activities and competencies are complementary and non-exclusive concepts. EPAs enable a practice-focused assessment of the resident’s acquisition of skills. The implementation of an EPA requires the recruitment of one or more of the competencies by the individual performing them. As an example, the hypothetical EPA “Perform anamnesis and physical examination” would recruit the competencies of medical expertise, patient care, communication, and professionalism11. And, therefore, the evaluation of this practical and observable activity would allow us to infer the individual’s acquisition of competencies5),(8.
In summary, the original description of the literature cites as competencies the individual’s attributes or qualities for professional practice, while the EPAs describe the work to be done in practice. Despite the difference between the concepts of competencies and EPAs, they can be mistaken, as the common use of language over time has often attributed as competencies concepts that are actually entrustable professional activities8. As an example, the CNRM6 FCM competency matrix for the year 2019 has some items listed as competencies that could be classified as “educational objectives” or even “entrustable professional activities”.
Considering the importance of these two concepts, it is recommended that a matrix be made in the curriculum descriptions that integrates EPAs and competencies5),(8.
Figure 1 schematically illustrates a model of integration between competencies and EPAs proposed by Ten Cate, Snell and Carraccio in 20105.
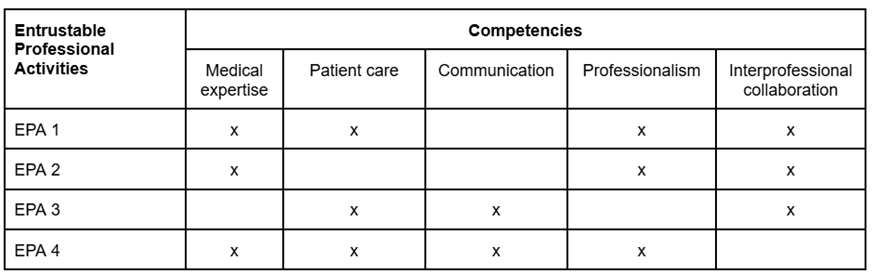
Source: Adapted from Ten Cate, Snell and Carraccio 20105
Figure 1 Integration matrix between EPAs and competencies.
There are already international descriptions of EPAs for residency in Family and Community Medicine (FCM)12),(13),(14),(15. In the national context, some specialties such as Gynecology and Obstetrics made an effort to describe the EPAs for the context in our country16. There is yet no description of the EPAs for the Family and Community Medicine Residency Programs in the Brazilian context. This description is important as an effort to define fundamental activities of the specialty and to support the definition of the specialty itself and differentiate it from the practice of the general practitioner.
It is recommended that each country develop its own Entrustable Professional Activities for residency, since local health contexts and needs vary17. The model proposed for this establishment involves the elaboration of an initial description of the EPAs by physicians of the specialty who have expertise in medical education and a subsequent validation, through consensus methodologies, by a larger group of physicians of the specialty10.
This study aims to describe the processes carried out for the initial proposal of EPAs for the Family and Community Medicine residency in the Brazilian context and the validation of these EPAs using the Delphi methodology to establish consensus.
METHOD
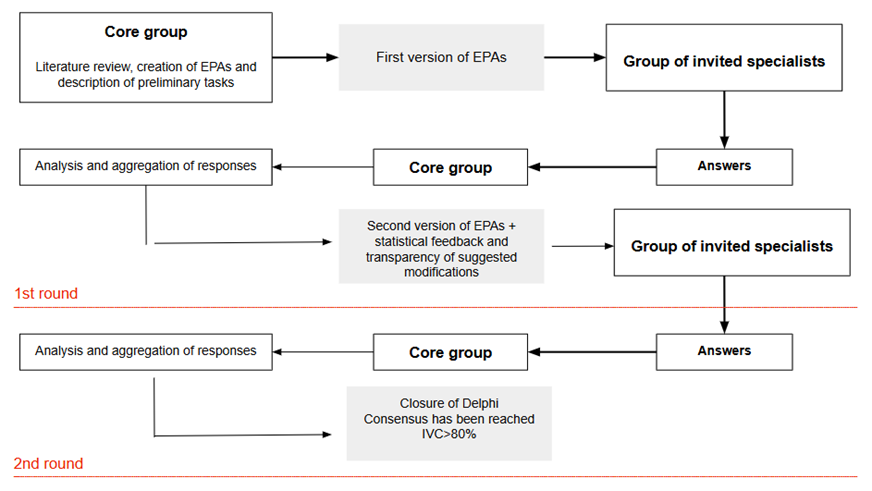
This study consisted of two phases: the first comprised the creation of the EPAs and tasks by a core group of experts, and a second of consensus using the Delphi technique. This consensus methodology is used to systematically combine the experts’ opinion to answer a problem18),(19. The model used was e-Delphi, with digital questionnaires, using the Google Forms® platform. This method was chosen because it allows greater agility and versatility in the response processes by participants and in the analysis by researchers, and this method does not detract from the traditional method20),(21),(22. Through this methodology, we aimed to reach consensus about the entrustable professional activities (EPA) and their task descriptions initially prepared by the group of researchers. Figure 2 illustrates and summarizes the methodology used in the research.
Creation of EPAs and their tasks
The core group of researchers was responsible for the initial creation of the EPAs and their respective task descriptions. This group consisted of six specialist physicians: three specialists in Family and Community Medicine, and three other medical teachers with expertise in medical education.
The EPAs and their initial descriptions were created based on curricula of national competences6),(23) for FCM training and international descriptions of EPAs for FCM residency. These international descriptions were found based on a scoping review conducted by the group of researchers: the countries where there were descriptions of EPAs for FCM residency at the time of the initial creation of these EPAs by the group were the United States, Canada, and Australia12),(13),(14),(15.
The creation of the EPAs by the core group took place through face-to-face and remote meetings and was based on recommendations from the literature to ensure clear and specific writing, aiming at practical application. Using as the theoretical basis the curricula based on national competencies and the international descriptions of EPAs, the group described the entrustable professional activities of the specialty. Comprehensive descriptions of EPAs were chosen, as recommended by the literature in the context of medical residency. After describing these activities, the group detailed the tasks corresponding to each activity, based on the references and needs of FCM training in Brazil10),(17),(24.
Selection of Experts for Delphi Composition
The selection of experts who respond to Delphi is one of the most important steps in this methodology, since the expertise of the established panel has a great impact on the results and consensus19. The inclusion criteria for the invitation were: being a specialist in FCM and having worked in the specialty for at least two years. Additionally, another criterion was having worked with FCM residents’ education for at least six months.
The dissemination of invitations to specialists was made through the Brazilian Society of Family and Community Medicine (SBMFC, Sociedade Brasileira de Medicina de Família e Comunidade) through its official website and by email to members. The specialists who accepted the invitation to participate in the study received the Free and Informed Consent Form (FICF) for reading from the research team. The specialists who accepted the FICF were included in the research and became part of the Delphi group.
Sociodemographic data collection
Data collection from the group of participants took place through the Google Forms® platform, and sociodemographic data were collected to characterize the sample.
The sociodemographic data collected were: age group, area of activity (urban or rural), region of operation in the country, time since graduation in FCM, time as a teacher in medical residency and the nature of the main institution to which they are linked (public/private/both).
Delphi Rounds
A differential semantic scale was used with the variables: “this task is indispensable”, “this task is very important”, “this task is not very important”, “this task should not be included”. Two Delphi rounds were held until consensus was reached.
In the first round, the participants received a Google Forms® via email to vote on the tasks of each of the proposed EPAs. In addition, in this first round, the participants could suggest changes in the wording of the tasks, modifications in the allocation of the task, suggestions for new tasks, and suggestions for new EPAs.
In the second Delphi round, the participants received a new digital form containing statistical feedback from the first round and highlighting the changes made after the proposals brought by the participating group in the first round. In the second round there was no possibility of suggesting modifications but only voting on the tasks.
Analysis of the data from the Delphi rounds
The Content Validity Index (CVI) was used to define consensus. According to the literature, consensus is recognized when the CVI value is greater than 80%19),(26. To calculate the CVI, the votes for “this task is indispensable” and “this task is very important” were added. This sum was divided by the total number of votes in each task. The answers obtained in each Delphi round were analyzed by the group of six researchers.
After the first Delphi round, the group of researchers met to discuss and define changes in the wording of the EPAs and the tasks, based on the suggestions brought by the participants and decide on the inclusion of new proposed tasks. The CVI of each task and the mean CVI of each EPA were also evaluated. Finally, a new document was prepared, including suggestions from the first round and submitted to the second Delphi round.
It was decided to access the Content Validity Index (CVI) of each task instead of the EPA, since consensus on the tasks contained in the latter was considered important, and the participants were able to suggest modifications to the writing of each EPA. The calculation of the CVI of each EPA was attained through the simple arithmetic mean of the CVI of each task composed in the EPA, since the Delphi methodology used in the study did not propose to rank the items, but rather to list the essential tasks of the EPA19. Considering the recommendations most often used in the literature to describe EPAs, they should be evaluated as a whole in their tasks, and there is no description of the attribution of different weights or importance to each task of a given EPA10),(28.
After the second Delphi round was over, the group of researchers met again to evaluate the final CVI of each task and the mean CVI of each EPA. The consensus data of the voted tasks were discussed, as well as the decision to exclude tasks that did not reach the previously established 80% of CVI.
RESULTS
A total of 60 people accepted the initial invitation from the SBMFC to constitute the panel of experts to respond to Delphi. Among the participants, 24 people met the inclusion criteria and agreed to participate and answered the first round of the Delphi survey, after reading and signing the FICF. In the second round, it was decided not to include new panelists and there was a loss of half of the panelists of the first round, and 12 people, of the initial group of 24 panelists, responded to the study. The participants’ sociodemographic profile in the first and second rounds is described in Table 1.
Table 1 Sociodemographic profile of the panelists participating in the first and second Delphi rounds of the study.
| Profile of the panelists participating in the research | First Delphi round (total n =24 participants) | Second Delphi round (total n =12 participants) | |
|---|---|---|---|
| Age group between 25-35 years | n=9 (37.5%) | n=4 (33.3%) | |
| Age group between 36-45 years | n=9 (37.5%) | n=4 (33.3%) | |
| Age group between 46-55 years | n=1 (4.2%) | n=1 (8.4%) | |
| Age group between 56-65 years | n=4 (16.7%) | n=2 (16.6%) | |
| Age group over 65 years old | n=1 (4.2%) | n=1 (8.4%) | |
| Urban Location | n=22 (91.7%) | n=12 (100%) | |
| Rural location | n=2 (8.3%) | n=0 | |
| Time working in Family and Community Medicine | x̅a=12.35 years (sb=±8.52 years) | x̅ =14.58 years (s=±10.24 years) | |
| Time working in medical education | x̅ = 10.64 years (s=±9.08 years) | x̅ = 14.46 years (s=±10.16 years) | |
| Participants who declared working in a public institution | n=17 (70.8%) | n=8 (66.7%) | |
| Participants who declared working in a private institution | n=5 (20.8%) | n=2 (16.6%) | |
| Participants who declared that they worked in public and private institutions | n=2 (8.3%) | n=2 (16.6%) | |
| Participants by region of origin | Southeast | n=15 (62.5% | n=7 (58.3%) |
| South | n=6 (25%) | n=3 (25%) | |
| Northeast | n=2 (8.3%) | n=2 (16.7%) | |
| Midwest | n=1 (4.2%) | n=0 | |
| North | n=0 | n=0 | |
Abbreviation: n:number.
Symbols: a: x̅=mean; b: S=standard deviation of the sample.
Source: Prepared by the author.
As for the composition of the panel of experts who agreed to participate in the survey, 75% were aged between 25 and 45 years. Regarding the place of work, 91.7% reported working in urban centers and 70.8% worked in public institutions. Most of the participants, 62.5%, worked in the southeast region of the country. The mean time working in Family and Community Medicine was 12.35 years and the mean time working in medical education was 10.64 years.
A total of 14 EPAs were created by the group of researchers and a total of 115 tasks describing these activities. In the first Delphi round, the participants answered a questionnaire containing 115 items, corresponding to the tasks and 37 of these tasks received suggestions for changes, including changes of terms to increase the clarity of writing, addition of contents and suggestion of transferring the described task to another EPA where it could fit better. It was also suggested in the first round the inclusion of a new task in the EPA called “to offer mental health care to the assisted individuals”, which is described as “knowing the criteria and making the diagnosis of common mental disorders indicating adequate initial therapy”.
Among the described tasks, two did not achieve a content validity index (CVI) greater than 80% in either of the rounds, and thus, they were excluded from the final description of the EPAs. The tasks were “to provide remote care to expand access in the first contact and continuity of care for patients”, which obtained a CVI of 66.7%, and “to recognize urgent and emergency situations in the virtual care modality and determine the action plan with patients and caregivers”, which obtained an IVC of 75%. The first belonged to the EPA named “to provide first contact access and longitudinality of care as part of a health system” and the second belonged to the EPA named “to manage the care of patients with medical emergencies”.
All 14 EPAs proposed by the researchers achieved an average CVI of the tasks greater than 80% and, therefore, were included. Consensus was reached with two Delphi rounds. Table 2 describes the average CVI of each EPA at the end of each of the two Delphi rounds and shows the final decision on the consensus.
Table 2 Mean CVI of the EPAs proposed by the researchers and consensus decision.
| Entrusted Professional Activities (EPA) proposals | EPA mean CVI after the First Delphi Round | EPA mean CVI after the Second Delphi Round | Decision on consensus |
|---|---|---|---|
| EPA 1 - Provide first-contact access and longitudinality of care as part of a health system | x̅a=94.91% (sb=±7.55%) | x̅=95.38% (s=±10.46%) | Yes |
| EPA 2 - Managing information continuity, coordinating care, and advocating for patients’ rights | x̅=93.06% (s=6.50±%) | x̅=94.79% (s=7.13±%) | Yes |
| EPA 3 - Act according to the needs of the local community context and provide patient- and family-centered home care | x̅=92.98% (s=4.89±%) | x̅=94.41% (s=5.57±%) | Yes |
| EPA 4 - Participate in interprofessional care activities | x̅=96.82% (s=3.46±%) | x̅=100.0% (s=0.0±%) | Yes |
| EPA 5 - To play a leading role in interprofessional health teams and act in a guided manner with a sustainable practice | x̅=91.67% (s=3.86±%) | x̅=93.51% (s=6.97±%) | Yes |
| EPA 6 - Provide women’s health care at all stages of life | x̅=96.78% (s=2.91±%) | x̅=98.08% (s=4.79±%) | Yes |
| EPA 7 - Offer care in a broad and longitudinal way to children and adolescents | x̅=100.0% (s=0.0±%) | x̅=100.0% (s=0.0±%) | Yes |
| EPA 8 - Offer care in a broad and longitudinal way to adults | x̅=97.49% (s=3.82±%) | x̅=99.17% (s=2.49±%) | Yes |
| EPA 9 - Offer care in a broad and longitudinal way to the elderly | x̅=98.09% (s=2.97±%) | x̅=96.21% (s=4.24±%) | Yes |
| EPA 10 - Provide mental health care to the assisted individuals | x̅=98.42% (s=2.03±%) | x̅=99.08% (s=2.61±%) | Yes |
| EPA 11 - Perform medical procedures in the primary health care setting | x̅=98.62% (s=1.96±%) | x̅=94.43% (s=6.22±%) | Yes |
| EPA 12 - Manage care for patients with medical emergencies | x̅=97.63% (s=5.80±%) | x̅=95.24% (s=8.74±%) | Yes |
| EPA 13 - Address vulnerabilities and complex conditions in PHC at all stages of the lifecycle | x̅=97.69% (s=2.85±%) | x̅=96.31% (s=4.12±%) | Yes |
| EPA 14 - Exercise self-regulation of the learning process and personal and professional development | x̅=97.23% (s=1.95±%) | x̅=97.23% (s=3.91±%) | Yes |
Abbreviations: CVI=content validation index; EPA=entrustable professional activity.
Symbols: a: x̅=mean; b: s=standard deviation of the sample.
Source: Prepared by the author.
The EPA with the highest degree of consensus were “Participate in interprofessional care activities” and “Offer care in a broad and longitudinal way to children and adolescents”, both with a CVI of 100%.
On the other hand, the EPAs “Managing information continuity, coordinating care, and advocating for patients’ rights”, “Act according to the needs of the local community context and provide patient- and family-centered home care “, “To play a leading role in interprofessional health teams and act in a guided manner with a sustainable practice “ and “Perform medical procedures in the primary health care setting” had the lowest CVIs, less than 95%. No EPA had a CVI < 90%.
At the end of the second Delphi round, Table 3 was constructed, containing the final description of the tasks of each EPA, as well as the CVI of each task. This CVI was obtained by the panelists’ voting in this second round, which contained the changes and written suggestions proposed by them in the first round.
Table 3 Description of the tasks of each EPA and its CVI at the end of the second Delphi round.
| Entrusted Professional Activities (EPA) | Final description of the EPA tasks | End CVI of the task |
|---|---|---|
| Provide first-contact access and longitudinality of care as part of a health system | Manage a regular schedule that allows first-contact access and longitudinality in patient care according to their needs | 100% |
| Provide in-person care as an essential part of patient-centered care | 100% | |
| Plan access and ensure care for patients who are unable to come to the office | 100% | |
| Adopt a patient-centered approach and work to establish a bond and become a trusted ally over time | 100% | |
| Define and manage patient relationship boundaries when necessary | 91.70% | |
| Support patient autonomy in decision-making | 100% | |
| Respect patient privacy and confidentiality | 100% | |
| Respond to unscheduled demand according to the available resources | 100% | |
| Manage information continuity, coordinate care, and advocate for patients’ rights | Maintain an up-to-date medical record for each patient as part of longitudinality practice | 100% |
| Identify and appropriately refer cases with follow-up criteria at other points of care in the health care networks (HCN) | 100% | |
| Coordinate patient care at all points of HCN care and support care transitions | 100% | |
| Follow-up on assessments carried out by other professionals, monitoring the results of investigations and consultations | 83.40% | |
| Fill out medical forms and documentation in accordance with local management determinations and provide medical reports as needed by patients | 83.30% | |
| Manage resources and participate in activities that address the use of health system resources | 83.3% | |
| Provide patients with the information they need to make their own healthcare decisions | 100% | |
| Provide guidance to the patient, their family and support network, as part of an interprofessional team in accessing local health and social resources | 100% | |
| Develop proposals considering inequities, gaps in access to care, and safety concerns at the workplace, when necessary | 91.60% | |
| Act according to the needs of the local community context and offer patient- and family-centered home care | Use patient data and information to support care planning | 100% |
| Manage the time of activities to ensure a balanced distribution of the supply of care needed by the assisted population | 91.60% | |
| Participate in local health surveillance and management activities, recognizing the needs and particularities of the territory and enrolled population | 100% | |
| Facilitate health promotion and education of the enrolled population | 91.60% | |
| Collaborate with the entities that constitute the health care networks (HCN) contributing to the planning and provision of continued care in the community | 91.60% | |
| Conduct home visits and maintain first-contact access and continuity of care in the home setting | 100% | |
| Attend meetings with the people who constitute the patient’s support network | 91.60% | |
| Ensure personal safety and health practices in the home care environment | 100% | |
| Foster an environment where concerns can be expressed and addressed, and ask for feedback from patients and families about their care experiences | 83.30% | |
| Participate in interprofessional care activities | Acting collaboratively in the field of interprofessional action of PHC in patient care | 100% |
| Know the core role of primary care professionals and respect their ethical limits | 100% | |
| Develop person-centered care plans in collaboration with other team members | 100% | |
| Promote continuing education activities within the interprofessional team | 100% | |
| Play a leadership role in interprofessional health teams and act in a guided way with a sustainable practice | Demonstrate reflective behavior in relation to their own practice as a resource of a defined population | 100% |
| Seek opportunities for personal development, self-knowledge and strengthening of interpersonal relationships | 91.60% | |
| Demonstrate professionalism in the presence of stress and adversity in the workplace | 100% | |
| Contribute to professionally safe practice environments with adequate conflict management | 100% | |
| Analyze and engage in improvements, quality, safety and sustainability at the practice and health system level | 91.70% | |
| Promote team engagement to achieve agreed objectives | 83.40% | |
| Anticipate security concerns and take risk reduction measures and act on security incidents | 83.40% | |
| Provide women’s health care at all stages of life | Manage the most prevalent health problems at each stage of a woman’s life cycle | 100% |
| Incorporate promotion and prevention and screening activities in consultations, taking into account the particularities of the assisted person | 100% | |
| Guide and assist in decision-making about contraception, institute the agreed method, and monitor the patient | 100% | |
| Guide the person with a desire for pregnancy and know the initial approach to fertility problems | 100% | |
| Provide assistance to the person with suspected and confirmed pregnancy, including an unwanted pregnancy | 100% | |
| Provide embracement and clinical assistance in situations of miscarriage | 100% | |
| Provide routine prenatal care and health promotion at all stages of pregnancy, including the partner, family, or support network when desired by the person | 100% | |
| Recognize risk factors and pregnancy-related complications and refer to the appropriate point of care of the HCN | 100% | |
| Assess and offer care for common symptoms and health concerns in the postpartum period, including mental health | 100% | |
| Recognize emergencies related to women’s health by referring them to the appropriate point of care for care | 100% | |
| Know and incorporate the specificities of LGBTQIA+ with female identity in their care | 91.60% | |
| Provide care and establish shared care plans with the health care network for women who are victims of violence | 100% | |
| Know and discuss, when pertinent, the impacts of machismo and heteronormativity on women’s health | 83.40% | |
| Offer care in a broad and longitudinal way to children and adolescents | Establish a bond with the child and adolescent and the child’s guardians, promoting a culture of care and using shared decision-making from the perspective of medical confidentiality and current legislation | 100% |
| Recognize and discuss the different models of family dynamics, generational conflicts and their impact on child and adolescent development | 100% | |
| Provide specific care for the first thousand days of the child’s life, recognizing opportunities and vulnerabilities for adequate coordination of team care | 100% | |
| Provide age-specific prevention and guidance, risk assessment, and immunization as part of routine care | 100% | |
| Identify and manage the most common acute situations in children and manage the care of chronic situations compatible with PHC complexity | 100% | |
| Identify and address age-specific behavioral concerns and deviations from normal neuropsychomotor development and refer to focal specialists when necessary | 100% | |
| Prescribe and monitor medication use while mindful of risks and age-specific considerations | 100% | |
| Coordinate the care of children and young people in the health care network and contribute to the development of care plans with patients, families and support networks | 100% | |
| Assess and manage security and violence issues in this population and meet the duties of notification and provision of information when necessary | 100% | |
| Offer care in a broad and longitudinal way to adults | Provide age-specific support, guidance and health promotion advice | 100% |
| Provide age-specific prevention, screening, risk assessment, and immunizations as part of routine care and periodic health assessment | 100% | |
| Recognize the work context of the assisted people and correlate it to the health/disease process | 100% | |
| Assess adults presenting with nonspecific conditions and manage their care | 100% | |
| Assess and manage clinical situations related to mental health and behavioral changes | 91.70% | |
| Identify and manage the most common acute outpatient conditions in adults in the territory served | 100% | |
| Coordinate care for adults with chronic illnesses, including self-care support | 100% | |
| Assertively communicate the results of evaluations with patients | 100% | |
| Prescribe and monitor a plan of care, including medication use, and be mindful of the individual’s specific risks and considerations | 100% | |
| Recognize the needs for referral and carry it out to the appropriate level within the health care network, performing joint follow-up of patients | 100% | |
| Offer care in a broad and longitudinal way to the elderly | Recognize the particularities of aging considering individuals and their needs | 100% |
| Know the instruments of the multidimensional assessment of the elderly and apply them when relevant | 91.60% | |
| Carry out age-specific health promotion and prevention for healthy aging | 100% | |
| Assess and manage the care of older adults who have nonspecific conditions | 100% | |
| Diagnose and manage acute conditions of low complexity | 91.70% | |
| Coordinate care for older adults with chronic illnesses, including multimorbidities and support self-care | 100% | |
| Prescribe and monitor the care plan, including medication use, and be aware of the risks of polypharmacy and the individual’s specific conditions | 90.90% | |
| Encourage autonomy and share the care plan with patients, their families, and/or their support network | 100% | |
| Recognize the needs for referral and carry it out to the appropriate point in the health care networks, carrying out joint follow-up of patients | 91.70% | |
| Offer mental health care to the assisted individuals | Diagnose and coordinate care of most common mental health conditions as part of an interprofessional team | 100% |
| Diagnose common mental disorders by indicating appropriate initial therapy | 100% | |
| Know the main mental health problems prevalent in the enrolled population, assessing vulnerabilities and recognizing signs of severity | 100% | |
| Assist in the coordination and continuity of care in the mental health care network and intersectoral network | 100% | |
| Recognize warning signs for complex mental health conditions and share care with the appropriate mental health network point | 100% | |
| Recognize and perform initial management of mental health emergencies | 100% | |
| Consider the particularities of the use of psychotropic drugs in PHC to make a safe prescription, taking into account individual factors, while paying attention to medicalization and other risks | 100% | |
| Recognize, stratify and plan the care of people with psychoactive substance use with an interprofessional team | 100% | |
| Include the family and key sources of support in care, as appropriate | 91.70% | |
| Perform medical procedures in the primary health care setting | Evaluate the indications, contraindications, and be prepared to respond to possible risks and complications of outpatient surgical procedures | 100% |
| Recognize individual and setting limitations and request support or refer the patient to appropriate HCN level equipment when necessary | 91.60% | |
| Prepare the patient, provide instructions, and obtain informed consent | 83.30% | |
| Monitor the patient after the procedure, being aware of late complications | 100% | |
| Refer surgical specimens for histopathological evaluation, when pertinent | 91.70% | |
| Inform the patient of the results of the evaluations in an assertive way and make referral to the appropriate level of the HCN as needed | 100% | |
| Manage care for patients with medical emergencies | Differentiate between urgent and emergency conditions | 100% |
| Anticipate and have action plans in place to respond to emergencies in the office, home care, and territory environments | 100% | |
| Perform patient risk classification correctly and establish an appropriate action plan according to the institution’s protocols | 100% | |
| Perform initial management of life-threatening common presentations and conditions | 100% | |
| Coordinate care for secondary and tertiary levels of care, always valuing patient safety, providing adequate medical transportation when necessary | 100% | |
| Perform patient follow-up after discharge from the emergency room to the community | 91.70% | |
| Address vulnerabilities and complex conditions in PHC at all stages of the lifecycle | Recognize conditions of vulnerability and the specificities of care for the population in this situation in their territory | 100% |
| Incorporate the social determination of health model as an integral part of care planning | 100% | |
| Work as part of an interprofessional team seeking to positively impact health outcomes associated with social and individual vulnerabilities | 100% | |
| Coordinate the care of patients with complex conditions and comorbidities by mobilizing resources from the HCN, the family, and the support network | 100% | |
| Recognize the impacts, on family dynamics, of people with complex clinical conditions and/or high demand for care, anticipating and acting in situations such as caregiver stress | 91.70% | |
| Build a shared and informed decision with patients, including family members and support networks, when relevant, about values and preferences in care | 91.70% | |
| Assess decision-making capacity and provide a substitute to make decisions when necessary | 91.70% | |
| Produce documents respecting ethical precepts with the necessary information, ensuring continuity of care for complex cases | 91.70% | |
| Deal with ethical conflicts in collaboration with people and their families and caregivers and seek resources and support from other professionals when needed | 100% | |
| Exercise self-regulation of the learning process and personal and professional development | Be available to offer, solicit and receive feedback from educators, co-workers or patients, demonstrating professionalism | 100% |
| Conduct a guided self-assessment using performance data in practice and of received feedback | 91.70% | |
| Create a continuous professional development plan with clear objectives, considering self-assessment and received feedback | 100% | |
| Recognize one’s own knowledge gaps and develop an action plan to respond to them autonomously | 100% | |
| Seek and critically evaluate evidence to solve specific clinical problems in care, integrating the person’s preferences | 100% | |
| Analyze data from their own practice and participate with the health team in improvement processes in the workplace | 91.70% |
Abbreviations: CVI=content validation index; EPA=entrustable professional activity.
Source: Prepared by the author.
DISCUSSION
The initiatives of local EPA creation are important and encouraged by the literature, since they take into account the specificities of each context27),(28. In Brazil, there are differences in relation to other countries in Family and Community Medicine residency: the time of training of the resident, which has a shorter duration of two years, the context of action focused on the needs of a universal and public health system, the SUS, and a territorialized PHC, with these factors not being contemplated in the evaluated international descriptions of EPAs for FCM. In addition, there is a variability of medical residency programs in FCM within the country itself29, which reinforces the importance of describing the activities and offers that are crucial for quality training.
Considering these needs, the group of researchers developed the EPAs taking into account international references for EPAs in FCM12),(13),(14),(15 and national curriculum descriptions for residency in Family and Community Medicine6),(23. For that purpose, it relied on the expertise of specialists working in Brazil. In the end, the fourteen EPAs prepared brought important elements of FCM into the Brazilian context, such as community care, action in the territory and work in health care networks (HCNs).
An unprecedented EPA in the literature was proposed by the group and approved with high CVI by the Delphi panel. This EPA is named “Addressing Vulnerabilities and Complex Conditions in PHC at All Stages of the Lifecycle”. It exemplifies the need for descriptions that respond to the local reality and needs, since for FCM training in Brazil it is important to act on individual, socioeconomic and territorial context vulnerabilities. Although the vulnerabilities are transversal in any reality, none of the descriptions of EPAs in FCM reported in the literature brought this focus and in our proposal this EPA was included with a high degree of agreement by the Delphi panel. By bringing this description as an EPA, the need to work on the topic in the residency curriculum is made explicit, highlights it as a fundamental task to be trained by the resident and denotes the reference to a socially responsible education17.
All the proposed EPAs described observable activities in the practice of the Family and Community Medicine resident, being innovative in the attempt to describe the specialty based on its main tasks. The use of the specialty description based on the EPAs, according to the literature, is expected to bring greater clarity to the content to be taught and in the practical offers provided by the residency programs9),(10.
The description of EPAs also has the potential to support the review of the description of the competencies expected of the FCM resident in training, since they are interdependent concepts. Author Olle Ten Cate5),(8, creator of the concept of EPAs, recommends the use of a matrix that correlates EPAs and competencies for a better assessment of the resident, and suggests that the way of starting from EPAs to describe competencies can be more effective and meaningful in the context of training and evaluation5.
Thus, the definition of national EPAs can support the orientation and reduction of differences in FCM residency training in Brazil by bringing greater clarity to the essential activities of the specialty and, consequently, the training offers of the programs13 and can also contribute to the strengthening of the specialty and its practice scenarios. Additionally, in the context of the country, the definition of EPAs contributes to the differentiation between the performance and practice of a Family and Community physician and a general practitioner.
All fourteen EPAs were approved by the Delphi panel through consensus. Only two tasks from two different EPAs did not reach consensus and were excluded, both of which were related to telecare and remote care. The group of researchers attributed this to the fact that telecare has been recently regulated in the country30 and that not all services and residency programs have availability and training to provide remote care.
As a weakness of the study, we must cite the low adherence to the Delphi panel, as in the first round 40% of those who received invitations from the SBMFC responded to the survey and in the second round we had a loss of 50% of those who responded to the first round. However, there was a high rate of agreement with the EPAs and proposed tasks.
The Delphi methodology has this difficulty because it requires evaluation more than once by the group of panelists18),(19. Furthermore, the questionnaire used took an average of 30 minutes to be answered, which was considered a potential factor for low adherence.
Nevertheless, in the participants’ analysis, a good representation of specialists was identified, and it was possible to select a good quality panel, considering experiences of work in the specialty and in teaching. The criteria for a qualified Delphi group according to the literature19),(20 incorporated by this study are: high average time of experience in the specialty and in the teaching of residents, representativeness of different regions of the country, representativeness of schools with different forms of financing, and the inclusion of diversity of generations of educators.
CONCLUSION
This study is innovative because, by describing the EPAs for the specialty of Family and Community Medicine in the Brazilian context, it contrasts the essential activities of the practice of the Family and Community physician and the expectations of the general practitioner’s working activities. This differentiation is important, because medical graduation in Brazil allows recently graduated physicians to work and they have PHC as one of the main action settings. By specifying the activities of Family and Community Medicine, it is possible to differentiate the performance in the complex and unique context of PHC and strengthen the specialty
The importance of developing EPAs for residency programs at the national level was evidenced, and that the transposition of EPAs described in other countries alone does not contemplate local needs. This was evidenced because thematics such as community care, activities related to specific public policies of our health system, network action and care for vulnerable populations, were highlighted by the group of researchers as specific to the Brazilian context and were validated by the Delphi group.
In addition, the potential of a qualified Delphi sample in the refinement and consensus of EPAs was demonstrated. The study offers as perspectives the initial implementation in FCM Residency Programs in different scenarios in Brazil, providing a methodology described for the programs that identify needs for local changes. It is recognized that future studies derived from this approach can be carried out to obtain a greater overview of national needs in FCM training.
ACKNOWLEDGEMENTS
To the Brazilian Society of Family and Community Medicine for supporting the development and dissemination of the research.
To the research group AFETO (Evaluation, Interprofessional Teaching, Student Engagement, Teacher Development and Curriculum) of Universidade Estadual de Campinas (Unicamp) and to Thalita Torres Sales.
To CNPq Universal Notice process number 421761/2023-7 for encouraging the AFETO research group.
REFERENCES
1. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638-45. doi: https://doi.org/10.3109/0142159X.2010.501190. [ Links ]
2. Frank JR, Snell L, Englander R, Holmboe ES, ICBME Collaborators. Implementing competency-based medical education: moving forward. Med Teach . 2017;39(6):568-73. [ Links ]
3. Englander R, Cameron T, Ballard AJ, Dodge J, Bull J, Aschenbrener CA. Toward a common taxonomy of competency domains for the health professions and competencies for physicians. Acad Med. 2013;88(8):1088-94. doi: https://doi.org/10.1097/ACM.0b013e31829a3b2b. [ Links ]
4. Brightwell A, Grant J. Competency-based training: who benefits? Postgrad Med J. 2013 Feb;89(1048):107-10. doi: https://doi.org/10.1136/postgradmedj-2012-130881. [ Links ]
5. Ten Cate O, Snell L, Carraccio C. Medical competence: the interplay between individual ability and the health care environment. Med Teach . 2010;32(8):669-75. doi: https://doi.org/10.3109/0142159X.2010.500897. [ Links ]
6. Brasil. Resolução CNRM nº 9, de 30 de dezembro de 2020. Matriz de competências em Medicina de Família e Comunidade [acesso em 10 de julho de 2024]. Disponível em: Disponível em: http://portal.mec.gov.br/publicacoes-para-professores/30000-uncategorised/71531-matrizes-de-competencias-aprovadas-pela-cnrm . [ Links ]
7. Ten Cate O. Entrustability of professional activities and competency-based training. Med Educ. 2005;39:1176-7. doi: https://doi.org/10.1111/j.1365-2929.2005.02341.x. [ Links ]
8. Ten Cate O, Schumacher DJ. Entrustable professional activities versus competencies and skills: exploring why different concepts are often conflated. Adv Health Sci Educ Theory Pract. 2022 May;27(2):491-9. [ Links ]
9. Ten Cate O, Scheele F. Competency-based postgraduate training: can we bridge the gap between theory and clinical practice? Acad Med . 2007 Jun;82(6):542-7. doi: 10.1097/ACM.0b013e31805559c7 [ Links ]
10. Ten Cate O, Taylor DR. The recommended description of an entrustable professional activity: AMEE Guide No. 140. Med Teach . 2021 Oct;43(10):1106-1114. doi: 10.1080/0142159X.2020.1838465 [ Links ]
11. Obeso V, et al; for Core EPAs for Entering Residency Pilot Program. Toolkits for the 13 core entrustable professional activities for entering residency. Washington, DC: Association of American Medical Colleges; 2017 [acesso em 9 de outubro de 2024]. Disponível em: Disponível em: aamc.org/initiatives/coreepas/publicationsandpresentations . [ Links ]
12. Garvin R, Mazzone M. ENTRUSTABLE PROFESSIONAL ACTIVITIES (EPAS): THE NEXT STEP. Ann Fam Med. 2017 May;15(3):283. doi: 10.1370/afm.2082 [ Links ]
13. Shaughnessy AF, Sparks J, Cohen-Osher M, Goodell KH, Sawin GL, Gravel Jr J. Entrustable professional activities in family medicine. J Grad Med Educ . 2013;5(1):112-8. doi: https://doi.org/10.4300/JGME-D-12-00034.1. [ Links ]
14. Fowler N, Wyman R, editors. Residency training profile for family medicine and enhanced skills programs leading to certificates of added competence. Mississauga, ON: College of Family Physicians of Canada; 2021 [ Links ]
15. Valentine N, Wignes J, Benson J, Clota S, Schuwirth LW. Entrustable professional activities for workplace assessment of general practice trainees. Med J Aust. 2019 May;210(8):354-9. doi: https://doi.org/10.5694/mja2.50130. [ Links ]
16. Comissão Nacional Especializada de Residência Médica. As EPAs (Entrustable Professional Activities) na formação do especialista em Ginecologia e Obstetrícia. Proposta da Febrasgo. São Paulo: Febrasgo; 2022 [ Links ]
17. Taylor D, Park YS, Smith C, Cate OT, Tekian A. Constructing approaches to entrustable professional activity development that deliver valid descriptions of professional practice. Teach Learn Med. 2021;33(1):89-97 [ Links ]
18. Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications, Information & Management, Volume 42, Issue 1, 2004, Pages 15-29, https://doi.org/10.1016/j.im.2003.11.002. [ Links ]
19. Humphrey-Murto S, Varpio L, Wood TJ, Gonsalves C, Ufholz LA, Mascioli K, Wang C, Foth T. The Use of the Delphi and Other Consensus Group Methods in Medical Education Research: A Review. Acad Med . 2017 Oct;92(10):1491-1498. doi: 10.1097/ACM.0000000000001812 [ Links ]
20. Michels NR, Denekens J, Driessen EW, Van Gaal LF, Bossaert LL, De Winter BY. A Delphi study to construct a CanMEDS competence based inventory applicable or workplace assessment. BMC Med Educ. 2012 Sep 14;12:86. doi: 10.1186/1472-6920-12-86 [ Links ]
21. Rowe M, Frantz J, Bozalek V. Delphi study to develop a technology mediated teaching strategy. BMC Med Educ . 2013;13(51):1-8. [ Links ]
22. Spranger J, Homberg A, Sonnberger M, Niederberger M. Reporting guidelines for Delphi techniques in health sciences: a methodological review. Z Evid Fortbild Qual Gesundhwes. 2022;172:1-11. [ Links ]
23. Sociedade Brasileira de Medicina de Família e Comunidade. Currículo baseado em competências para medicina de família e comunidade. Rio de Janeiro: SBMFC; 2015. [ Links ]
24. Hennus MP, van Dam M, Gauthier S, Taylor DR, Ten Cate O. The logic behind entrustable professional activity frameworks: A scoping review of the literature. Med Educ . 2022 Sep;56(9):881-891. doi: 10.1111/medu.14806. [ Links ]
25. Chueiri, P.S., Harzheim, E. e Takeda, S.M.P. 2017. Coordenação do cuidado e ordenação nas redes de atenção pela Atenção Primária à Saúde - uma proposta de itens para avaliação destes atributos. Revista Brasileira de Medicina de Família e Comunidade. 12, 39 (ago. 2017), 1-18. DOI: https://doi.org/10.5712/rbmfc12(39)1363. [ Links ]
26. Bull C, Crilly J, Latimer S, et al Establishing the content validity of a new emergency department patient-reported experience measure (ED PREM): a Delphi study. BMC Emerg Med. 2022 Apr 9;22(1):65. doi: 10.1186/s12873-022-00617-5 [ Links ]
27. Cate OT. An updated primer on Entrustable Professional Activities (EPAs). Rev Bras Educ Med. 2019;43(1):712-20. [ Links ]
28. Hennus MP, Jarrett JB, Taylor DR, Ten Cate O. Twelve tips to develop entrustable professional activities. Med Teach . 2023 Jul;45(7):701-707. doi: 10.1080/0142159X.2023.2197137 [ Links ]
29. Simas, K.B. da F., Gomes, A.P., Simões, P.P., Augusto, D.K. e Siqueira-Batista, R. 2018. A residência de Medicina de Família e Comunidade no Brasil: breve recorte histórico. Revista Brasileira de Medicina de Família e Comunidade . 13, 40 (dez. 2018), 1-13. DOI: https://doi.org/10.5712/rbmfc13(40)1687. [ Links ]
30. Brasil. Lei nº 14.510, de 27 de dezembro de 2022. [acesso em 10 de julho de 2024]. Disponível em: Disponível em: https://www.planalto.gov.br/ccivil_03/_ato2019-2022/2022/lei/L14510.htm [ Links ]
Received: July 24, 2024; Accepted: November 17, 2024
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
