











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Since the establishment of the Portuguese court in Brazil, several changes have taken place in Brazilian medical education, including the Flexenerian reform implemented during the military regime, which proposed a university-based medical school with a pedagogical scientific-based program and a four-year course, two dedicated to the basic areas and two to practical activities. During this period, medical education was based on diseases and the medicalization aiming at their cure, without considering the individual’s psychosocial aspects1.
In 1988, with the creation of the Unified Health System in Brazil, the implemented health model started to cover the entire population, taking into account the individual health needs and the individual’s psychosocial character2, and thus, it became necessary to train doctors to meet these needs, which was materialized with the National Curriculum Guidelines (NCGs) for undergraduate medical school from 2001 and 2014. These NCGs proposed the training of general practitioners to work in the prevention, promotion, recovery and rehabilitation of the patient3),(4. Due to the NCGs, which came into effect on December 31, 20184, the student became the main actor of their learning, with the teacher being a supporting actor, a facilitator of the teaching and learning process, through which the student starts to be evaluated according to the skills acquired in learning, in addition to using active teaching methodologies1),(3),(5.
In order to determine whether or not the student has achieved the desired competences for medical training, an assessment is required. With the implementation of the NCGs, the assessments are no longer just aimed at attaining passing grades to find out whether the student is able or not to move on to another stage of the course, but becomes a formative assessment, aiming to investigate failures during practical activities, so that they are reflected by the students through the assimilation of concepts and scenarios that have been experienced and promote behavior changes, so that the desired skills are achieved6. The main characteristic of this type of assessment is the use of a learning instrument called feedback, which is performed immediately after an activity7.
Feedback in medical practice can be defined as the transfer of data observed by preceptors during medical practice, contextualizing cognitive knowledge, practical skill, decision making and whether the learning objectives were achieved, aiming at a student’s reflection, so they can rebuild their knowledge and change their way of acting, improving their performance so that they can attain the necessary skills for the profession for the patient’s benefit8. Feedback is important for students to reflect on their performance, what is the desired performance and to seek support to improve their resourcefulness in practical environments. Secondarily, feedbacks are important for students to act autonomously, through self-reflection and continuous learning6. Its objective is to emphasize good medical practices, appreciating the students’ good performance and promoting a critical reflection on the aspects that need improvement, in addition to how they can be improved6),(9.
For feedbacks to be effective, the rapport between teacher and student is necessary, as well as a clear communication, the student’s understanding and identification of the learning objectives that are desired by both the student and the preceptor8. Moreover, the time devoted to the observation, the place where the feedback was carried out, the content and type of feedback communication also influence the feedback effectiveness. Therefore, there are several obstacles to providing and receiving an effective feedback. There are reports that many preceptors are unaware of or are not used to communicating feedback to students11),(12. Furthermore, many students do not understand that they are receiving feedback8. Therefore, aiming to build proposals for the improvement of giving and receiving feedback, the main objective of the study was to evaluate the perception of preceptors and students at the USCS - Bela Vista, about the feedbacks in internships in Diadema.
METHODS
Type of study
A qualitative-quantitative cross-sectional study was carried out aiming to analyze the perception of a group of medical students and teachers about feedback. This study was approved by the Research Ethics Committee of Universidade Municipal de São Caetano do Sul (USCS). Opinion Number: 3.551.101 and REC protocol: 17717019.8.0000.5510.
Location
Data from this sample were collected from four public health sites: the Municipal Hospital of Diadema (HMD), the Municipal Emergency Department of Diadema (Central ED), the Mobile Emergency Care System (SAMU, Sistema de Atendimento Móvel de Urgência) of the municipality of Diadema and the Psychosocial Care Center (CAPS, Centro de Atenção Psicossocial), both located in the city of Diadema, municipality of São Paulo, southeastern Brazil.
Eligibility Criteria
Medical undergraduate students from USCS attending the seventh and eighth semesters (Bela Vista Campus) and who had already attended the following clinical internships in Diadema: Internal Medicine - HMD, Pediatrics - Central PS, SAMU (Emergency Mobile Care Service) and CAPS (Psychosocial Care Centers), from March 5th, 2018, to August 21st, 2019, who agreed to participate in the research and signed the consent form, were included in the study. Also included in this study were the hired and/or tenured USCS preceptors responsible for practical internships during the same periods and in the same places who agreed to participate in the research.
Students attending the 7th semester that had not finished all internships (Internal Medicine, Pediatrics, SAMU and CAPS) during the study evaluation period were not included in this investigation. Students and/or preceptors who did not sign the free and informed consent form or who did not accept to participate in the research were excluded from the study.
Procedures
Potential individuals selected for this study were invited to participate in the investigation via WhatsApp. Questionnaires for the evaluation were provided to students at the University Secretary Office and provided to preceptors at their respective workplaces. From March 5th to August 21st, five groups of students went through the four practical internships, totaling fifty students. Of these, thirty students agreed to participate in the study and answered the questionnaire. Among the nine preceptors responsible for the practical internships, eight agreed to participate and were included in this study.
The evaluation questionnaires were based on questions by Maia et al13. The questions were adapted to categorical and qualitative questions in two questionnaires, being one for preceptors and one for students. The questionnaire adapted for student assessment contained 11 categorical questions and eight open questions that evaluated feedback. All categorical questions had five items as answer options that varied between “completely agree”, “agree”, “neither agree nor disagree”, “disagree” and “completely disagree”. The content of the questions asked to the students was whether they were aware of what feedback was and the goals of receiving it. How often they received feedback during the internships and what was the impact (positive and negative) of feedback on their practice. What situations made students uncomfortable during the practice of feedback and if they knew how to handle criticism when receiving feedback. It was also evaluated whether students noticed any changes in their practice after receiving feedback and whether they would like the feedback to be a constant practice. Moreover, what characteristics or qualities a preceptor should have and how the student would like to receive feedback were assessed. Finally, it was also evaluated whether the students were able to provide feedback to the teacher and whether they had already noticed any changes in the teacher after receiving their feedback. More details about the questionnaire applied to students can be seen in (Appendix 1).
To assess the preceptors, a socio-demographic questionnaire was applied, followed by the same version of Maia’s questionnaire, after being modified and adapted for the preceptors and containing nine categorical questions and six open questions13. All categorical questions had five items as answer options that varied between “completely agree”, “agree”, “neither agree nor disagree”, “disagree” and “completely disagree”. The content of the questions asked to the preceptors was how much knowledge they had and whether they knew how to provide feedback. How often they provided feedback or how else they assessed students. It was also assessed whether the preceptors knew the different ways to provide feedback, which ones they used and whether they could identify whether the feedback provided was effective for the student. Moreover, it was assessed whether the preceptors identified specific characteristics in the student to benefit from feedback and what were these characteristics. It was evaluated whether the preceptors had difficulties in offering negative feedback to the students and in which situations, and finally, it was evaluated whether the preceptor requested feedback from the students and whether they intended to modify their practice as a preceptor after the student’s feedback.
The primary study variables were questions regarding the difficulties met by students and preceptors in receiving and providing feedback, respectively. The secondary variables comprised the frequency of receiving and offering feedback, the preceptors’ experience with feedback, change in student behavior and what characteristics the preceptor and the student must have.
Statistical Analysis
Quantitative data from this study were analyzed using frequency analysis for categorical data, which calculates absolute numbers and percentages for each assessed question; and through descriptive analysis for continuous data, calculating the mean and standard deviation of each variable.
The qualitative statistical analysis was performed in 3 steps: (1) transcribing and organizing data into thematic units (words or phrases that described the topics present in the participants’ responses); (2) data exploration, which involved careful reading and organization of data into categories (these categories were created according to the frequency of thematic units identified in step 1 and using the content technique. This technique analyzes the data using the frequency inference method and also through the analysis by thematic categories14; and (3) data interpretation and summarization. All authors approved the thematic units and categories created during data analysis15.
RESULTS
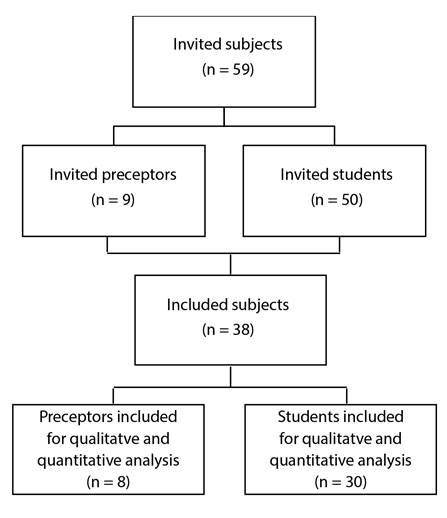
A total of 59 individuals were invited to participate in this study, as shown in Figure 1. However, only 38 agreed to participate and were included for data analysis in this study, eight preceptors and 30 students. The main reason that some invited individuals did not participate in the study was because the potential participant did not respond to contact attempts via email or WhatsApp.
Preceptors’ results
The preceptors included 4 men and 4 women, with a mean age of 39 years (SD = 5.4). Most were physicians (75%), the level of schooling varied between postgraduate education and residency, both comprehending 75% of the teachers, to master’s degree (37.5%) and doctoral degree (25%). A total of 75% of the preceptors had experience with health education and of these, the time of experience was on average 23 months (SD=39.9).
The preceptors’ self-report on feedback knowledge ranged from no knowledge (12.5%) to a lot of knowledge (25%). Most preceptors (75%) agreed that they knew about the objectives of providing feedback. The results on the frequency with which they provided feedback varied greatly according to each teacher; for instance, while 12.5% of the teachers never provided feedback, 25% of them provided it in all practical classes. Half of the teachers reported knowing about the different ways to provide feedback to their students, and the majority (37.5%) reported having no difficulty in providing feedback. Most preceptors (62.5%) declared that students need to have specific characteristics to benefit from feedback. Additionally, only 12.5% of teachers reported they have never asked for feedback from the student about their performance as a teacher, and most of them agree to change their behavior after receiving feedback from the student. More details on the preceptors’ quantitative results can be found in Table 1.
Table 1 Preceptors’ quantitative results.
| No knowledge | Little knowledge | Moderate knowledge | A lot of knowledge | Deep knowledge | |
|---|---|---|---|---|---|
| 1 - Do you know what feedback is? | 1 (12.5%) | 3 (37,5%) | 2 (25%) | 2 (25%) | 0(0) |
| I completely disagree | I disagree | I neither agree nor disagree | I agree | I completely agree | |
| 2 - I am aware of the objectives of providing feedback | 0(0) | 0(0) | 6 (25%) | 8 (75%) | 0(0) |
| 3 - I know the different ways to provide feedback | 0(0) | 2 (25%) | 2 (25%) | 4 (50%) | 0(0) |
| 4 - I can assess whether my feedback was effective | 0(0) | 2 (25%) | 4 (50%) | 2 (25%) | 0(0) |
| 5 - Students need to have specific qualities to benefit from feedback. | 1 (12.5%) | 1 (12,5%) | 1 (12,5%) | 5 (62,5%) | 0(0) |
| 6 -I have difficulty in providing feedback to the student | 0(0) | 3 (37,5%) | 2 (25%) | 2 (25%) | 1 (12,5%) |
| 7 - I am willing to change my method of assessment when a student criticizes my feedback. | 0(0) | 0(0) | 2 (25%) | 4 (50%) | 2 (25%) |
| Never | Rarely | Occasionally | Very often | In all practical activities | |
| 8 - How often did you provide feedback? | 1 (12.5%) | 2 (25%) | 1 (12,5%) | 2 (25%) | 2 (25%) |
| 9 - How often do you request feedback from students about your performance as a teacher? | 1 (12.5%) | 2 (25%) | 3 (37,5%) | 2 (25%) | 0(0) |
The results were presented in absolute numbers (percentage).
Qualitatively, the teachers were instructed to write about several questions when providing feedback to the student during a practical medical internship. The topics discussed with these teachers were: (1) objectives when providing feedback; (2) frequency with which they provided feedback; (3) types of feedback they more often provided; (4) how they assessed whether a feedback was effective; (5) in which situations it was difficult to provide feedback; (6) what qualities a student needs to have to receive an effective feedback. All contents reported in each of the topics are presented in Table 2, as well as the number of citations of each content according to the preceptors’ responses.
Table 2 Preceptors’ qualitative results.
| Topics/ Content | Number of citations* |
|---|---|
| Feedback Objectives | |
| Assisting in difficulties | 4 |
| Transmitting reflection on practice | 3 |
| Motivating strengths | 2 |
| Feedback frequency | |
| Always | 2 |
| Whenever necessary | 2 |
| Once per internship | 2 |
| Never | 1 |
| Types of feedback | |
| Oral | 6 |
| Constructive | 2 |
| Brief | 2 |
| Evaluating Feedback Effectiveness | |
| To observe attitudes | 6 |
| To ask the student | 2 |
| Difficulty in providing a negative feedback | |
| Fear of hurting the student | 2 |
| When the student does not know how to receive criticism | 2 |
| To correct aspects of the student’s personality | 1 |
| Student’s Qualities to Receive Effective Feedback | |
| Active listening | 4 |
| Interest | 3 |
| Resilience | 2 |
| Handling criticism well | 1 |
| Respect and empathy | 1 |
*The number of citations represents the number of times the content was mentioned in the preceptors’ responses. This decision was made because the open-ended questions did not limit the number of answers a preceptor could provide.
Students’ results
The students reported having moderate (40%) to deep (6.7%) knowledge about feedback, and the majority reported being aware of the objectives of receiving feedback. None of the students reported receiving feedback in all practical classes. According to the students, the feedback had a positive impact on their learning, with 53% and 40% of the students agreeing and completely agreeing with it. When asked about the negative impact of feedback on learning, 30% and 43% of the students completely disagreed or disagreed with this statement. Most students disagreed with feeling uncomfortable when receiving feedback after a practical performance (37% and 47%) and that they handle well receiving negative criticism during feedback (60% and 13%). Most students reported that they observed changes in clinical practice after receiving feedback (57% and 37%) and agreed (53%) and completely agreed (37%) that feedback should be a constant practice in their course. Finally, the students were asked if they could provide feedback to the preceptor and the answers were varied; some did it and even saw a change in the teacher’s practice, but most did not or could not find space and felt insecure to provide feedback to the teacher. More details on the preceptors’ quantitative results can be found in Table 3.
Table 3 Students’ quantitative results.
| No knowledge | Little knowledge | Moderate knowledge | A lot of knowledge | Deep knowledge | |
|---|---|---|---|---|---|
| 1- Do you know what feedback is? | 0(0) | 0(0) | 12 (40%) | 16(53.3%) | 2 (6.7) |
| I completely disagree | I disagree | Neither agree nor disagree | I agree | I completely agree | |
| 2 - I am aware of the objectives of receiving feedback | 0(0) | 0(0) | 1 (3.3%) | 19 (63.3%) | 10(33.3%) |
| 3 - Feedback had a positive impact on my learning. | 0(0) | 2 (6.7%) | 16(53.3%) | 12(40%) | 0(0) |
| 4 - Feedback had a negative impact on my learning | 9 (30%) | 13(43.3%) | 6(20%) | 1 (3.3%) | 0(0) |
| 5- I feel uncomfortable receiving feedback after a practical performance. | 11 (36.7%) | 14(46.7%) | 4(13.3%) | 1 (3.3%) | 0(0) |
| 6 - I handle negative criticism well during feedback. | 0(0) | 0(0) | 8 (26.7%) | 18 (60%) | 4(13.3%) |
| 7 - There was a change in my medical practice after feedback from the preceptors | 0(0) | 0(0) | 2 (6.7) | 17(56.7%) | 11 (36.7%) |
| 8 - The preceptor needs to have specific characteristics to provide effective feedback. | 1 (3.3%) | 5 (16.7%) | 7 (23.3%) | 16(53.3%) | 1 (3.3%) |
| 9 - I would like feedback to be a constant practice in my course. | 0(0) | 0(0) | 3 (53.3%) | 16 (53.3%) | 11 (36.7%) |
| 10 - My teacher has already asked me to provide feedback on their performance. | 5 (16.7%) | 6 (20%) | 6 (20%) | 8 (26.7%) | 4 (13.3%) |
| Never | Rarely | Occasionally | Very often | In all practical activities | |
| 11- How often did you get feedback? | 1 (3,3%) | 10 (33,3%) | 11 (36,7%) | 8(26,7%) | 0(0) |
The results were presented as absolute numbers (percentage).
Qualitatively, students were instructed to write about several questions when receiving feedback from the preceptor, during their practical medical internship. The topics discussed with these students were: (1) objectives of receiving feedback; (2) the positive impact of feedback; (3) the negative impact of feedback; (4) what changes are observed after feedback; (5) what are the qualities of the preceptor to provide effective feedback; (6) characteristics of an ideal feedback; (7) characteristics of uncomfortable feedback. All contents reported by students in each of the topics are presented in Table 4, as well as the number of citations of each content.
Table 4 Students’ qualitative results.
| Topics/content | Number of citations* |
|---|---|
| Feedback Objectives | |
| To identify strengths and weaknesses | 18 |
| Technical improvement | 17 |
| Personal growth | 4 |
| Evaluation | 2 |
| Positive impact of feedback | |
| To identify and improve weaknesses | 16 |
| Clinical improvement | 10 |
| Change in behavior | 4 |
| To guide the studies | 4 |
| Negative impact of feedback** | |
| Aggressive attitude | 4 |
| Demotivation | 3 |
| No change in behavior | 2 |
| Changes observed after feedback | |
| Improvements in anamnesis and physical examination | 11 |
| Change in behavior | 8 |
| Improvement in the therapeutic alliance | 6 |
| Improvement in treatment | 4 |
| Improvement in the description of the medical record | 3 |
| Preceptor’s qualities to provide effective feedback | |
| To be respectful | 13 |
| To be constructive | 9 |
| To be clear | 7 |
| To be an expert on the subject | 5 |
| To be consistent | 4 |
| Ideal feedback | |
| To provide constructive negative criticism | 12 |
| To be Individual | 9 |
| To be more frequent | 7 |
| To provide positive criticism | 5 |
| Oral and written feedback | 4 |
| To be polite | 3 |
| Uncomfortable feedback ** | |
| Exposure in front of the patient | 6 |
| Exposure in front of colleagues | 4 |
| None | 3 |
| Criticizing without pointing out how to improve | 1 |
*The number of citations represents the number of times the content was cited in students’ responses. This decision was made because the open-ended questions did not limit the number of answers a student could provide.
**This item had a lower number of citations because most students did not answer the question, it was understood that these students did not observe negative or uncomfortable impact of the feedback.
DISCUSSION
The current study showed quantitative and qualitative data regarding impediments and suggestions for improvement in feedback assessment during practical internships in undergraduate medical school. The results were reported according to the students’ perception on feedback, but also according to the preceptors’ perception, since these two viewpoints are not always similar regarding the same concepts. From the preceptors’ point of view, the impediments comprising lack of knowledge and inadequacy regarding the ways of approaching feedback were identified, as well as an impediment regarding the lack of effective communication between preceptors and students. From the students’ point of view, the identified impediments comprised the frequency of feedback, students expect feedback more often, they do not mind negative feedback if it involves constructive criticism and they prefer the preceptor to assess them individually, without exposing them in the presence of the patient or their colleagues.
Regarding the feedback objectives, the preceptors and the students showed agreement regarding the answers and reported, for instance, that clarifying doubts is one of the objectives, as well as reinforcing the positive aspects of the practical activity, in addition to motivating critical reflection on the performed actions. These concepts are in line with the literature; feedbacks should focus on the student’s development in practical activities, informing them about necessary changes that contribute to improve their performance, in addition to motivating students to reflect on how to solve the detected problems16. The objectives of the feedbacks also include making students aware of their good practices during the internship and which knowledge domains, be it cognitive, psychomotor or behavioral, need improvement to help the student obtain the desired skills during the internship6. Moreover, the feedback must contain information with guidelines for students to perform better in future activities17.
The frequency of feedback is very important to ensure an effective assessment; while from the preceptors’ viewpoint, feedbacks were offered with a high frequency or in all practical classes, none of the students reported having received feedback in all practical classes, and few students said they frequently received them. This finding is similar to what was observed in the study by Liberman et al.18, in which the authors reported that 86.2% of surgeons gave feedback immediately after the practical activity and only 12.5% of the residents observed this frequency18. Teachers often do not understand the practice of feedback and how to convey it, so the frequency of communication may be lower than what the preceptors reported16. This reinforces the fact that being a specialist in the subject to be transmitted, as well as the length of experience in the field of medical education does not necessarily mean being a good preceptor, that is, one who encourages student reflection and promotes information about the necessary improvements. The difficulty in communicating feedback can occur when medical preceptors do not keep up-to-date; they convey the content according to the way they learned it, because they believe that their length of experience is enough to meet their pedagogical needs. This difficulty in conveying the feedbacks can affect the students’ perception; the fact that the feedbacks do not have specific information on which behavior should be modified and do not contain suggestions on how to improve them, make students unaware of the feedbacks17. Therefore, it is necessary to improve the interaction between teachers and students, to provide clear, constructive and targeted feedback, so that it can be effective.
There are data that show that alone, students have difficulty understanding where and how they can improve their clinical skills; thus, the ability to give specific, timely and clear feedback is a fundamental skill for the preceptor17. For Nottingham et al.19, preceptors with less experience provided a fewer number of feedbacks to the students, while more experienced ones provided more feedbacks19, which is also observed in this study, where preceptors with longer experience in the area of health education (two years and 10 years ) offered feedback in all practical classes.
In the present study, the types of feedback used by preceptors were oral, brief and constructive. Although there are several ways to provide feedback, students preferred the oral feedback, probably because it is easier to provide and receive immediately20. Other types of feedback that could be incorporated are: (1) Brief feedback, which aims to provide information on the need to change some action at the time it is observed; (2) formal feedback, in which information is given at the end of the activity, focusing on one or two specific skills, lasting from 5 to 20 minutes; (3) major, which is the guidance given in the middle of the internship or at its end, regarding more complex performances and behaviors, culminating with an action plan to attain improvements before the end of the internship cycle, lasting from 15 to 30 minutes20.
Regarding the evaluation of the feedback effectiveness, only a quarter of the preceptors reported knowing how to evaluate. This result differs from a previous study, in which 90.9% of surgical preceptors reported evaluating the effectiveness of the feedback offered to the residentes18. The feedback effectiveness can be assessed by observing the tasks and actions for which improvements were proposed and whether these were carried out, in addition to the students’ degree of motivation to rebuild their knowledge to perform the necessary changes. Feedback is not always accepted by students, leading to self-reflection and behavioral changes, especially when the information given by the tutors is in conflict with the students’ ideas. When this happens, there may be failure in the acquisition of clinical competences and, therefore, the effectiveness that the feedback proposes is not attained21. In the present study, half of the preceptors found it difficult to provide negative feedback to students. Teachers have the perception that providing negative feedbacks can cause a break in the teacher/student relationship, in addition to affecting their popularity. To alleviate these effects, preceptors address criticisms in a lighter way, conveying messages indirectly. The lack of feedback that is clearly directed to the student may not be an effective feedback21.
On the other hand, the percentage of negative impacts caused by the provided feedbacks in this study was small. To reduce this negative impact, the feedback communication needs to be clear, respectful, non-judgmental, based on what was observed at the time and what is amenable to change, aiming to promote reflection and motivation, thus favoring changes in clinical practice22. The place where this feedback is provided seems to be the main reason for the discomfort. In a private place, feedback can be given in a clear, timely and specific way, providing an increase in student learning, as it facilitates the communication between the student and the preceptor without fear of being ridiculed by the colleagues23. Additionally, behavioral changes occur more often when there is an agreement between what was said by the teacher and the student’s way of thinking; moreover, the degree of feedback acceptance is associated with the student’s self-evaluation power24.
Regarding the positive impacts of feedback, the results observed in this study were positive and are similar to another study in the literature, in which 95% of the students tried to change their behavior according to the feedback that was received11. Another important point to highlight was that most students report that they wish the feedbacks were routine practices in practical internships. The students report that although preceptors have the knowledge and are aware of the objectives of the assessment instrument, it is not used constantly during the internships. In agreement with our results, 60 to 75% of the students in the study by Al-Mously et al25 considered the frequency with which feedback was provided was low to adequate, attributing it to the lack of a structural basis for the feedback communication to be carried out25.
The students’ feedback to the preceptors does not seem to be frequent during the internship practice. Students can give feedback to preceptors about their perception of this transmissibility, providing an exchange of information to be considered and offering the necessary changes, constituting a bidirectional learning17. It was observed that preceptors prefer to receive feedback from people who have the skills to assess their professional practice performance, which is also perceived by students, who prefer to receive feedback from teachers they consider to be professional role models10. Finally, preceptors who receive feedback and use them to improve their professional performance, whether as a doctor or teacher, are more committed to providing better feedback to the students25.
We emphasize that this study sought different ways to understand the difficulties in conveying and receiving feedback according to the viewpoints of preceptors and students, respectively; however, the study has some limitations. The main one is that the sample consisted mainly of a small group of students and preceptors involved in clinical internships in Diadema. These results may not reflect the total perception of students at the USCS (Bela Vista) and not all of Diadema’s practical internship preceptors. Therefore, another limitation is that it is not possible to extrapolate the results to all preceptors or students regarding the practice of feedbacks in clinical internships carried out in Diadema, nor to determine whether this practice was efficient or not.
Finally, the practical implications of the present study show that the effectiveness of feedbacks will be present when the preceptors propose corrections, promote reflections, are didactic and qualified for their communication. This can be achieved by structuring the feedback through the creation of a feedback guide, including information on how to structure an effective feedback, training on how to convey it under the supervision of trained preceptors and using practical scenarios, in which preceptors will experience situations on how to provide feedback, using the tools proposed by the guide. In order to adjust this transmissibility, it is necessary to verify how feedback is being carried out and interpreted by students in practical activities, through a feedback written by themselves on the preceptors’ role when conveying them.
CONCLUSION
We conclude that the preceptors’ improvement in carrying out an effective assessment through feedback is necessary. This study was able to list the necessary characteristics to perform an ideal feedback from the students’ viewpoint, such as, for instance, the fact that the feedback needs to be individualized, without exposing the student; to be respectful; clear; concise, and mainly involving constructive criticism. A point to note is that most preceptors report that they frequently provide feedback, although more than half of the students said they only received feedback rarely or occasionally. This point can be seen as an effective communication failure between the preceptor and the student. Moreover, students should be encouraged to offer feedback to the preceptors on how the feedback could be more effective, as an educational alliance is necessary to have better acceptance of the feedback, which means a better understanding between preceptor and student.

