











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Cervical cancer is a public health problem, since it is the fourth most common type of cancer and the fourth cause of death due to the occurrence of neoplasia in the female population worldwide, the vast majority occurring in developing countries1. As an example, 16,590 new cases of cervical cancer per year are expected in 2020-22 in Brazil, according to data from National Cancer Institute, with an estimated average risk of 15.43 new cases per 100,000 women2.
Among the known risk factors for developing cervical cancer, high-risk Human Papillomavirus (HPV) infection ranks a prominent place3),(4. Experts estimate that most sexually active men and women will have contact with the virus at some point in their lives. However, spontaneous regression of the infection occurs in more than 80% of the cases5. Infection persistence is necessary for the onset of neoplasia and it has an estimated 85-99% prevalence in cervical cancer cases6.
The Brazilian Health System introduced the HPV immunization program in 2014. Currently, in addition to other specific indications, the quadrivalent HPV vaccine is available in the Unified Health System (SUS) for females aged nine to 14 years and males aged 11 to 14 years in a two-dose schedule with a 6-month interval7. The strong correlation between oncogenic HPV infection and cervical cancer makes vaccination an essential public health prevention tool8. However, although clinical trials established the vaccine’s safety and efficacy9, the adherence to vaccination falls short of conventional standards. In 2017, the cumulative vaccination coverage of the HPV vaccine in Brazilian girls aged nine to 14 years was 82.6% for the first dose and 52.8% for the second dose. Among boys aged 12 and 13, only 43.8% of them had received the first dose7.
Solid knowledge and a positive attitude towards the vaccine among medical students indicate a favorable outlook for their future actions as health service providers in adhering to screening and vaccination programs10. For example, in the United States, Afonso et al.11, using a 15-item survey, highlighted that fully vaccinated compared to non-vaccinated respondents had a better understanding and more positive attitudes. However, in Scotland, McCusker et al.12 revealed the lack of knowledge of first-year students about the extent of protection against cervical cancer provided by the vaccine, and in China, Wen et al.13 indicated poor knowledge of HPV and HPV vaccination among medical students.
Therefore, the study aimed to assess the medical students’ grasp of knowledge related to HPV, its relationship with cervical cancer, and the vaccine against the virus according to their profiles, level of study, and vaccination status. It was assumed that a significant relationship would be found between the students’ knowledge and their level of study and demographic profiles.
METHODS
Participants
In a cross-sectional study, students attending from the first to the sixth years of medical school at the University of Brasilia answered a survey devised as a test questionnaire. The survey test included questions about cervical cancer, HPV, and the vaccine against HPV, with possible responses including, Yes, No, and I Don’t Know. The development of the instrument benefited extensively from published examples in the literature8),(14)-(16. The Ethics Committee in Research on Human Beings of the School of Medicine approved the study (1,989,835).
The eligibility criteria comprised attendance in the second semester of 2017 by students aged at least 18 years old from each period (semester) of the undergraduate medical school. As a rule, students were contacted during class time. As reported elsewhere, 392 students returned the survey tool and the signed consent form, but 13 cases were excluded from the study (six because the respondents omitted information about HPV vaccination and seven because they were younger than 18 years old)17. Therefore, the analyses included the questionnaires from 379 students, 72.7% of 521 students enrolled in the second half of 2017. Therefore, the estimated sample size for a satisfactory response rate (95% confidence level, 3% interval) comprised 350 students.
Procedures
We grouped the participants according to gender, monthly family income, sexuality profile, vaccination status, and year at medical school. The family income, established according to the number of minimum wages earned per month upheld two groups: a higher-income (≥ five minimum wages per month) and a lower-income (< five minimum wages per month) group. Regarding the vaccination status, three groups were identified: one of vaccinated participants, a second comprising those who were not vaccinated but who wished the immunization and the third included the students who did not receive nor wanted the vaccine. As for the sexuality, celibates constituted one group and sexually-active participants the other. Finally, the study level separated students attending years 1 to 4 from years 5 to 6 (which includes the internship). This last criterion included students before and after approval in Gynecology and Obstetrics courses (held in the 8th semester of the medical program).
A preliminary review of the responses to 57 knowledge items of the questionnaire excluded seven questions with a problematic discrimination index and item-total score correlation. For the remaining 50 questions, the reliability analysis showed acceptable internal consistency (Cronbach’s alpha = 0.87), even if a factor analysis detected multiple components in the students’ responses. Thus, a sum of correct answers was calculated for that set of items. Henceforth, the resulting total score, expressed as a percentage, was named the K-test score.
Statistical Analysis
In addition to means, frequencies, and proportions, the statistical analyses included t-tests for differences, Pearson’s correlations, analyses of contingency and one-way ANOVA, all for K-test scores between the student groups. Effect sizes and confidence intervals (CI) were calculated, and p<0.05 (two-tailed) was adopted for statistical significance. The SPSS software, version 17, was used in the statistical analysis.
RESULTS
The mean age of the 379 participants was 21.8 ± 3.1 years and, among them, 82 (21.6%) were aged 24 or older. Of the total, 218 (57.5%) were males, and among 368 respondents, 279 (75.8%) reported a monthly family income equal to or greater than five minimum wages. As for the sexuality profile, of the 372 respondents (who informed about recent sexual partners), 218 (58.6%) used barrier contraceptive methods, 97 (26.1%) declared themselves to be celibates, 93 (25.0%) reported two or more partners, and 44 (11.8%) admitted sexual initiation before 16 years of age.
Regarding the participants’ HPV-vaccination status, 80 (21.1%) reported being vaccinated, while 215 (56.7%) had not received the vaccine but wished to, and 84 (22.2%) had neither received it nor wanted to. However, the rates of vaccination were significantly different between males (9.2%) and females (37.3%); the odds ratio for female immunization was 5.88 (95% CI 3.36, 10.29); Fisher’s exact test < 0.0001.
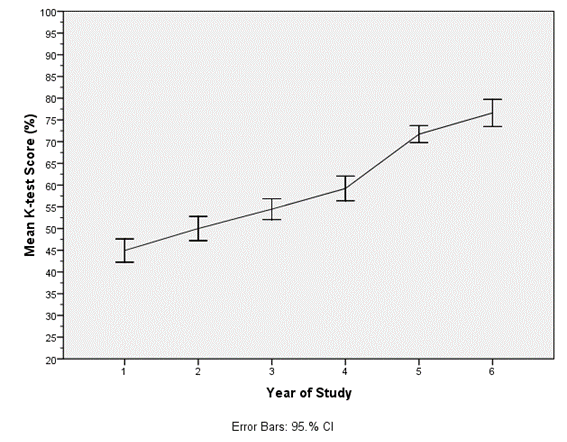
The K-test average score for the 379 participants was 60.6% (SD= 15.4%). The correlation between the student’s score and the year at the medical school was strong (r= .706, p<0.001). In addition, students attending years 5 to 6 had a much higher score than those attending years 1 to 4 (t = 19.0, df = 262.6, p <0.0001). Figure 1 shows the upward trend of the K-test results for students from year 1 to year 6 and highlights the increase in the growth rate from year 4 to year 5, in parallel to K-test topics’ formal learning in the 8th semester of the Gynecology-Obstetrics courses.
Sexually-active students had higher K-test scores than celibate students (t = 3.26, df = 275, p = 0.001). Likewise, students who reported higher family income had higher scores than those who reported lower income (t = 2.91, df = 366, p = 0.004). On the other hand, there was no significant difference between male and female students regarding the K-test scores (t = 0.47, df = 377, p = 0.638). The data depicted in Table 1 show the much larger effect size (Cohen’s d) of the study level when compared to the other conditions.
Table 1 Differences (by decreasing effect size) in K-test scores between medical students grouped according to their level of studies, sexuality, monthly family income, and gender.
| Students’ Conditions | Groups | N | K-test scores | Difference (95% CI) | Cohen’s d |
|---|---|---|---|---|---|
| Mean (SD) | |||||
| Level of study | Years 5-6 | 108 | 76.6 (9.3) | 22.3 (20.1, 24.7) | 1.91 |
| Years 1-4 | 271 | 54.3 (12.5) | |||
| Sexuality | Sexually Active | 267 | 62.2 (14.7) | 5.6 (2.2, 9.0) | 0.37 |
| Celibate | 110 | 56.6 (15.5) | |||
| Monthly family income | >US$300 | 279 | 62.0 (15.3) | 5.4 (1.8, 9.1) | 0.35 |
| <US$300 | 89 | 56.6 (15.2) | |||
| Gender | Male | 218 | 60.3 (15.6) | -0.08 (-3.9, 2.4) | 0.05 |
| Female | 161 | 61.1 (15.2) |
K-test: knowledge (%) of items related to human papillomavirus and associated conditions.
CI: confidence interval. Cohen’s d: effect size.
Using one-way ANOVA procedures, no significant differences in K-test scores were found among respondents, grouped according to sexual behavior (F = 0.54, df = 2; 367, p = 0.593). Similarly, no significant differences emerged in K test scores between participants grouped according to HPV vaccination status (F = 2.85, df = 2; 376, p = 0.059). Nevertheless, the scores increased according to adherence status: from 58.3 (not vaccinated, nor willing to), to 60.3 (not vaccinated, but willing to) to 64.0 (vaccinated).
According to the students’ level of study, a distinctive upward trend in the percentage of correct answers was observed for most K-test items. Table 2 shows the association (for 13 selected items) between each item answer (correct or incorrect) and the level of study (1st to 4th year vs. 5th to 6th year). Again, significant associations appeared for both underperforming and high-performing items. However, in contrast to information-based responses, responses to attitude-related questions (e.g., vaccination and multiple sexual partners) were not associated with the study level.
Table 2 Measures of association (Odds Ratio) between the study levels and correct responses to survey items on the medical students’ knowledge about HPV-related topics.
| Survey items (ordered by increasing percentage of overall correct answers) | Correct/ Incorrect Response | Study Levels | Odds Ratio (95% CI) | Fisher’s Exact test | |
|---|---|---|---|---|---|
| Year 1-4 | Year 5-6 | ||||
| HPV is a cause of infertility | C | 7 | 34 | 17.2 (7.3,40.5) | <0.0001 |
| I | 263 | 74 | |||
| The preventive Pap smear can detect HPV infection | C | 16 | 32 | 6.7 (3.5,12.8) | <0.0001 |
| I | 254 | 76 | |||
| HPV causes genital herpes | C | 68 | 77 | 7.4 (4.5,12.2) | <0.0001 |
| I | 202 | 31 | |||
| HPV vaccine is available to both boys and girls | C | 95 | 90 | 9.2 (5.2,16.2) | <0.0001 |
| I | 175 | 18 | |||
| HPV can be transmitted by sitting on a toilet seat | C | 109 | 95 | 10.8 (5.8,20.2) | <0.0001 |
| I | 161 | 13 | |||
| HPV may cause anal and oral cancers | C | 151 | 85 | 2.9 (1.7,4.9) | <0.0001 |
| I | 119 | 23 | |||
| Early sex is a risk factor for cervical cancer | C | 164 | 99 | 7.2 (3.5,14.8) | <0.0001 |
| I | 107 | 9 | |||
| HPV vaccination is inadequate for males | C | 186 | 95 | 3.3 (1.7,6.2) | 0.0001 |
| I | 84 | 13 | |||
| Most HPV infections are symptomatic | C | 183 | 101 | 6.9 (3.1,15.4) | <0.0001 |
| I | 87 | 7 | |||
| HPV vaccination promotes sexual promiscuity | C | 205 | 85 | 1.2 (0.7,2.0) | 0.5922 |
| I | 66 | 23 | |||
| The efficacy of HPV vaccination is higher before sexual initiation | C | 210 | 101 | 4.1 (1.8,9.3) | 0.0003 |
| I | 60 | 7 | |||
| Multiple sexual partners are a risk factor for cervical cancer | C | 215 | 107 | 27.9 (3.8,204) | <0.0001 |
| I | 56 | 1 | |||
| The HPV vaccine is available in the public health services | C | 246 | 108 | 10.5 (1.4,78.9) | 0.0047 |
| I | 24 | 1 | |||
HPV: human papillomavirus. C: correct. I: incorrect. CI: confidence interval.
Only three of the 50 K-test items (36, 49, and 50) showed a significant association with HPV vaccine acceptance among the 297 unvaccinated students. Table 3 shows the association between each response item (correct or incorrect) and acceptance of vaccination (unwilling vs. wishing). However, in an unplanned binary logistic regression analysis, four variables were significant predictors of vaccine desirability: gender (female; OR = 6.5, p <0.001), age group (<24 years; OR = 3.3, p = 0.001), sexuality (active; OR = 2.7, p = 0.002) and item 36 (incorrect; OR = 2.0, p = 0.029). In the regression model summary, Nagelkerke R Square was equal to 0.227 (meaning that those four items represent 22.7% of the variability in HPV vaccination desire).
Table 3 Measures of association (Odds Ratio) between medical students’ responses to items about knowledge on HPV-related topics and their acceptance of the HPV vaccine
| Survey Items (number) | Correct, Incorrect Response | Acceptance of Vaccine | Odds Ratio | Fisher’s Exact Test | |
|---|---|---|---|---|---|
| Not Wishing | Wishing | (95% CI) | |||
| 49. The HPV vaccine is available in the public health services | C | 73 | 205 | 3.1 (1.3,7.6) | 0.0137 |
| I | 11 | 10 | |||
| 50. The HPV vaccine is available to both boys and girls | C | 31 | 110 | 1.8 (1.1,3.0) | 0.0289 |
| I | 53 | 105 | |||
| 36. Most HPV infections are symptomatic | C | 55 | 167 | 1.8 (1.1,3.2) | 0.0390 |
| I | 29 | 48 | |||
| 11. Multiple sexual partners are a risk factor for cervical cancer | C | 65 | 185 | 1.8 (.95,3.4) | 0.0822 |
| I | 19 | 30 | |||
HPV: human papillomavirus. C: correct. I: incorrect. CI: confidence interval.
Concerning some specific items, 81% of participants satisfactorily recognized various risk factors for cervical carcinoma, and only 3.7% were unaware of the Pap smear test. Also, 94.7% knew that HPV could infect men and women, and more than 60% knew the causal association of HPV with various cancer sites. Furthermore, most of the students (73.6%) knew about the protection against cervical cancer offered by the HPV vaccine, but 23.5% of the participants suspected that vaccination could increase sexual promiscuity. Besides, 93.7% of students were aware of the availability of the HPV vaccine in public health services, but only 48.9% of them knew that the vaccine is available to both sexes.
DISCUSSION
As expected, a significant association emerged between the participants’ knowledge of HPV-related topics (K-test score) and level of medical study, a finding similar to what was reported by other authors18)-(21. Notably, the increase in the K-test score growth rate between the fourth and fifth years was associated with the approval in the Ob-Gyn courses in the 8th semester of the medical school. The robust odds ratios observed for 13 items in Table 2 corroborate the influence of that learning experience.
Also, significant differences in K-test scores emerged for the income and sexual activity groups. Regarding the family income, the means of correct answers were significantly lower in the lower-income group. Thus, income can be a potential influencer in terms of the students’ access and incorporation/ understanding of available information. As for sexual activity, it is interesting to note that celibate students scored lower on the knowledge of HPV-related topics, perhaps because it was not their concern at that time. A recent study found no association between receiving the HPV vaccine and sexual behavior, condom, and contraceptive method use22.
No significant gender difference turned up in the K-test score, a finding similar to that reported by Liu et al.10. Notably, the HPV vaccination rate was significantly higher among women. However, the three-year delay in the inclusion of boys in the national HPV immunization program7) may partly explain the lower adherence to the vaccine by men. Additionally, the vaccination campaigns focused on cervical cancer prevention, not on penis, anal, and oropharynx cancer prevention21.
Several factors may explain the inconclusive differences in K-test scores concerning students’ vaccination status. First, the K-test score is a global measure of declarative HPV-related knowledge, and vaccination seems to be associated with specific information. Second, the immunization timing preceded the appraisal of knowledge in this study, given the students’ age profile. Third, we found evidence that personal advice (mostly parental) was a more powerful source of influence among those participants17. The finding that corroborates this line of reasoning was that only three information items were related to the acceptance (desire) of the HPV vaccine. Of course, health professionals’ attitudes, the standard of public health information, and various individual, social, and cultural factors may better explain acceptance and adherence to vaccination.
Overall, the data from the present study showed that most students satisfactorily recognized the risk factors for cervical carcinoma; 94.7% knew that HPV could infect both sexes, and over 60% knew the association between HPV and several cancer sites. However, Deriemaeker et al.16 found that despite the high HPV vaccination rate in Belgium, 46% of medical students and 26% of students from other courses knew that HPV could cause cancer in the anogenital region (anus and penis). In another study, only 44% of the medical students surveyed at a university in India correctly answered that HPV could cause vulva, penis, oral and vaginal cancer23.
Additionally, surveys from six Chinese universities found that only 14.4% of medical students who answered a questionnaire believed that persistent HPV infection could cause cervical cancer, and 48.8% of them that vaccination could prevent cervical cancer8. In the present study, most participants (73.6%) were aware of the protection against cervical cancer offered by the HPV vaccine.
Notably, almost a quarter of the participants admitted the influence of HPV vaccination on sexual promiscuity. This issue has been a concern of parents regarding girls’ immunization, mainly about the risk of stimulating early sexual intercourse24. A study conducted in 2009 showed that, for those people, sexuality should be discussed before vaccination, since many believed that campaigns could increase risky sexual behavior25. However, a study carried out in England did not observe differences regarding sexual behavior between groups of vaccinated and non-vaccinated adolescents26. Also, a Scandinavian study found that the mean age at the first sexual intercourse was not significantly different between women who had been vaccinated against HPV before or after the onset of sexual activity and the number of sexual partners27.
The present study has limitations. Because of its cross-sectional design, it not possible to establish a cause-effect relationship between the knowledge about HPV-related topics and the demographics, sexuality profile, and vaccination status of the participants. The test used assesses just a sample of declarative knowledge and not a deep understanding of HPV issues. Furthermore, since the study included medical students from a single school of medicine, it is impossible to generalize the findings to other schools or students.
Nevertheless, the results represent the student-body’s grasp of HPV-related topics, and some findings show compelling associations. For example, we found it interesting that several students asked for more information about some test issues after the questionnaire application, even those already covered in the medical curriculum. The findings suggest a need for improvement in screening and vaccination programs and educational strategies regarding HPV-related diseases. Better instructional strategies may help future physicians to instruct different social groups and to clarify their patients’ doubts about those topics.
CONCLUSION
The study revealed a strong correlation of medical students’ HPV-related knowledge with the year attended at the medical school and significantly higher scores among sexually active and higher-income respondents, but no essential difference between males and females or between vaccinated and unvaccinated students. Altogether, the results indicate that the medical students’ attributes and external backgrounds have a more considerable influence on the HPV-vaccination status than the educational environment and formal training.

