











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
As the world becomes increasingly interconnected, both economically and socially, the adoption of technology remains one of the defining factors of human progress1. Particularly, the smartphone is the currently available main means of technology use, with its use being common nowadays as, according to the United Kingdom, 93% of the population has a smartphone2. Smartphones have many incentives to offer, such as improving social skills, entertainment and social identity preservation3.
However, it is a habit that can become an addiction, being a common problem among adults worldwide4, and, based on that, many harmful events can occur in the social, mental and academic areas5. Nomophobia then arises as a result of this misuse. The term ‘nomophobia’, which comes from the English phrase ‘NO MObile PHOne PhoBIA’, is a mental condition caused by the fear of being detached from mobile phone connectivity6, in which the individual is afraid to be without the electronic device, most commonly the smartphone. Moreover, nomophobia is directly associated with depression, anxiety and stress7),(8. Also from this perspective, the World Health Organization (WHO) considers addiction as a disease, making it important to further investigate this problem, which is common in society. Furthermore, it is necessary to understand that smartphone addiction is closely related to nomophobia and may even have the same characteristics9.
An investigation showed that 60% of its sample of medical students had moderate and 22.1% had severe nomophobia10. An even higher prevalence was found among medical students from a medical institution: 100% of the students had this condition11. This problem can lead to several adverse effects; among them, the decrease in connectivity between the orbitofrontal cortex and the nucleus accumbens. Additionally, withdrawal symptoms and higher serum cortisol levels were also observed12. From a structural point of view, a European study showed that individuals with smartphone addiction had less gray matter in the inferior temporal region, in the parahippocampal cortex and in the left anterior insular region13.
Nomophobia is a very prevalent pathology among students, especially those in the healthcare field. Although knowledge and mastery of this subject are important, few studies have been carried out with health care students in Brazil; therefore, further clarification is required to understand the topic. This scarcity of information supports the relevance of the present study, which aims, therefore, to assess the prevalence of nomophobia among medical students and its association with depression, anxiety, stress and academic performance.
METHOD
Study and sample characterization
This is an observational cross-sectional study of medical students from Centro Universitário Christus. For sample size calculation, the prevalence of nomophobia of 24.12%, recently identified among dental students in a cross-sectional study was considered, as well as a type II error of 20% (80% power) and a significance level of 95%, leading to a minimum sample of 305 individuals14. Properly enrolled students who attended at least 75% of classes and had a smartphone were included. Students considered unable to answer the questionnaires due to physical, mental or psychological disability were excluded from the study. Students who did not accept to participate in the study were considered as absent cases for subsequent sensitivity analysis.
The medical course at Centro Universitário Christus is a reference course, with 14 years of existence and has hybrid curriculum (conventional classes and Problem-Based Learning). Students were approached in person from March to June 2019 and after agreeing to participate in the study, they signed the free and informed consent form and filled out a sociodemographic questionnaire and two validated questionnaires: the Depression Anxiety and Stress Scale 21 (DASS-21) and the Nomophobia Questionnaire (NMP-Q).
Measurements
NMP-Q and DASS-21
Nomophobia was measured using the Nomophobia Questionnaire (NMP-Q)6. The NMP-Q has 20 questions, which are asked on a 7-point Likert scale, with 1 being “strongly disagree” and 7 “strongly agree”. This scale was validated for the Brazilian Portuguese language in 202015. The interpretation, according to the authors, is based on the number of scored points. The total score of the NMP-Q is 20 as the minimum score (20 * 1) or 140 (7 * 20) as the maximum score, and the results can be classified as: less than 20 points: no nomophobia; 21-59: mild level of nomophobia; 60-99: moderate level of nomophobia and 100-140, severe nomophobia.
Depression, anxiety and stress were measured using the DASS-2116, a simplified version of the DASS instrument. The DASS-21 questionnaire was validated for the Brazilian Portuguese language17. The questionnaire contains of a set of three 4-point Likert-type subscales (0-3) of self-response, starting with 0 (not applicable at all) to 3 (totally applicable, or applicable most of the time), in which the symptoms of stress, depression and anxiety are grouped together. The first one is defined by the presence of negative affection, such as depressed mood, insomnia, discomfort and irritability, which are nonspecific symptoms associated with stress; the second one encompasses factors that constitute structures representing specific symptoms of depression (anhedonia, absence of positive affection); and, finally, the last structure refers to the specific symptoms of anxiety (somatic tension and hyperactivity).
Academic Performance Index (API)
The API is the result of a complex mathematical operation that results in a student’s average grade in the semester and serves as a reference index for pedagogical monitoring at Unichristus. It is a grade obtained through a calculation, representing a student’s average grade in the course to date. The API is calculated using the following formula:
In which FG(D1S1) means the final grade (or final average) of the 1st discipline/module obtained in the student’s 1st semester record only for the PASSED disciplines in the record, except for the subject called Complementary Activity, FG (D2S1) is the final grade (or final average) of the 2nd discipline/module obtained in the student’s 1st semester record only for the PASSED disciplines in the record, except for a discipline called Complementary Activity. And so forth, up to the last discipline that the student passed in the 1st semester, which will be FG(DNS1), which means the final grade (or final average) of the Nth discipline/module obtained in the students 1st semester record only for the disciplines in which the student PASSED in the record, except for the discipline called Complementary Activity. NDS1 means the number of disciplines (passed and failed only, except for the disciplines called “Complementary Activity”) taken in the 1st semester of the student’s record. The FG(D1S2) means the final grade (or final average) of the 1st discipline/module obtained in the student’s 2nd semester record only for the disciplines in which the student PASSED in the record, except for the discipline called Complementary Activity.
FG(D2S2) means the final grade (or final average) of the 2nd discipline/module obtained in the student’s 2nd semester record only for the disciplines the student passed in the record, except for the subject called Complementary Activity. And so forth, up to the last discipline in which the student passed in the 2nd semester, which will be FG(DNS2), which means the final grade (or final average) of the Nth discipline/module obtained in the student’s 2nd semester record only for the disciplines that the student passed in the record, except for the discipline called Complementary Activity. NDS2 means the number of disciplines (passed and failed only, except for the disciplines called “Complementary Activity”) taken in the 2nd semester of the student’s record.
FG(D1SN) means the final grade (or final average) of the 1st discipline/module obtained in the student’s Nth semester record only for the disciplines the student passed in the record, except for the discipline called Complementary Activity. The FG(D2SN) is the final grade of the 2nd discipline/module obtained in the student’s Nth semester record only for the disciplines the student passed in the record, except for the discipline called Complementary Activity. And so forth, up to the last discipline the student passed in the Nth semester, which will be FG(NDSN), which means the final grade of the Nth discipline /module obtained in the students Nth semester record only for the disciplines the student passed in the record, except for the discipline called Complementary Activity. NDSN means the number of disciplines (passed and failed only, except for the disciplines called “Complementary Activity”) taken in the Nth semester of the student’s record. NAS means the number of academic semesters attended by the student.
Sociodemographic variables
The socio-demographic questionnaire consisted of five questions that addressed the semester the student would be attending at the time, the tutoring group (an environment in which learning is based on Problem-Based Learning, an active methodology for seeking knowledge), and the student’s number, which was necessary, so that we could associate the Academic Performance Index (API) data in a fully anonymous manner. In addition to these, data on the student’s age and gender were also collected.
Statistical analysis
Nomophobia, anxiety, stress and depression scores were expressed as mean and standard deviation and compared between API categories using the Mann-Whitney test, as well as being categorized as recommended in their validation articles. The API of students was divided into tertiles (<7.8; 7.8-8.3; >8.3) for the expression of absolute and percentage frequency and crossing with sociodemographic factors using Pearson’s chi-square test or Fisher’s exact test for categorical and Mann-Whitney for numerical variables. Correlation analyses with cubic extrapolation were also performed. A sensitivity analysis was performed with cases that refused to participate (13 students), and the variation in the associations was not significant. Values of p<0.05 were considered significant. The data obtained at the collection were tabulated and analyzed using IBM SPSS Statistics for Windows, Version 23.0 software, Armonk, NY: IBM Corp. IBM Corp. Released 2015.
Ethical aspects
This study was approved by the research ethics committee of Centro Universitário Christus and registered under CAAE 87329618.4.0000.5049. All information was collected based on the Brazilian Resolution 466/12, which regulates the principles of ethics in research with human beings. Free and informed consent terms were offered and obtained from all participants.
RESULTS
This study had a sample of 292 medical students from Centro Universitário Christus, among which 59.9% were females and 40.1% were males, 32.9% were attending the 1st to 3rd semesters, while 67.1% comprised students from the 4th to the 8th semesters. Moreover, 69.6% were over 20 years of age (mean 22, standard deviation 4).
Practically all students (99.7%) had some degree of nomophobia, and 64.5% had a moderate or severe level of nomophobia. A total of 11.8% had severe nomophobia. More than 50% of the students had greater than mild degrees (from minimal to very severe) of stress, and 19.5% and 11.2% of students had severe or very severe anxiety and depression, respectively (Table 1).
Table 1 Prevalence of nomophobia, stress, anxiety and depression among the 292 assessed students.
| n (%) or mean ± standard deviation | |
|---|---|
| NMQ Score | 71.2 ± 24.1 |
| NMQ in categories | |
| No nomophobia | 1 (0.3) |
| Mild nomophobia | 104 (35.1) |
| Moderate nomophobia | 156 (52.7) |
| Severe nomophobia | 35 (11.8) |
| API in tertiles | |
| 1st | 112 (38.4) |
| 2nd | 92 (31.5) |
| 3rd | 88 (30.1) |
| DASS-21 | |
| Score in the stress domain | 16.4 ± 10.8 |
| Score in the anxiety domain | 8.2 ± 9.2 |
| Score in the depression domain | 8.6 ± 9.1 |
| Stress domain in categories | |
| Normal/Mild | 131 (47.2) |
| Minimum | 37 (13.3) |
| Moderate | 48 (17.3) |
| Severe | 40 (14.4) |
| Very severe | 21 (7.5) |
| Anxiety domain in categories | |
| Normal/Mild | 154 (55.7) |
| Minimum | 23 (8.3) |
| Moderate | 45 (16.3) |
| Severe | 23 (8.3) |
| Very severe | 31 (11.2) |
| Depression domain in categories | |
| Normal/Mild | 178 (64.4) |
| Minimum | 35 (12.6) |
| Moderate | 32 (11.5) |
| Severe | 13 (4.7) |
| Very severe | 18 (6.5) |
When analyzing the profile of cell phone use by the students, it was observed that most of them (60.5%) use it for a total accumulated time for a period of less than four hours, and this accumulated use is associated with API, with the lowest time of use being associated with the best API (p=0.021). However, most individuals check their cell phones every 5, 10, or 20 minutes. Among the purposes, the most prevalent were talking or sending messages to family and friends, followed by researching information, with more than 80% of respondents using it for this purpose. The use of e-mail, prevalent in almost 70% of the students, was associated with worse API (p-value of 0.04), as well as the use to schedule meetings (p = 0.001) (Table 2).
Table 2 Cell phone use profile and its association with API.
| API | |||||||
|---|---|---|---|---|---|---|---|
| Total | <7.8 | 7.8 or more | p-value | ||||
| Accumulated time of smartphone use per day? | |||||||
| Up to 4h | 150 | 55.1% | 46 | 46.0% | 104 | 60.5% | 0.021 |
| >4h | 122 | 44.9% | 54 | 54.0% | 68 | 39.5% | |
| Smartphone check frequency | |||||||
| Every 5, 10 or 20 minutes | 152 | 55.5% | 59 | 59.0% | 93 | 53.4% | 0.373 |
| Every 30 minutes or more | 122 | 44.5% | 41 | 41.0% | 81 | 46.6% | |
| Purpose of smartphone use | |||||||
| 203 | 69.5% | 68 | 62.4% | 135 | 73.8% | 0.041 | |
| Check class notes | 173 | 59.2% | 62 | 56.9% | 111 | 60.7% | 0.525 |
| Check social media | 250 | 85.6% | 92 | 84.4% | 158 | 86.3% | 0.649 |
| Playing games | 60 | 20.5% | 24 | 22.0% | 36 | 19.7% | 0.631 |
| Receive news | 164 | 56.2% | 56 | 51.4% | 108 | 59.0% | 0.203 |
| Spend time | 207 | 70.9% | 71 | 65.1% | 136 | 74.3% | 0.095 |
| Search for information on the internet | 262 | 89.7% | 95 | 87.2% | 167 | 91.3% | 0.264 |
| Listen to music | 205 | 70.2% | 77 | 70.6% | 128 | 69.9% | 0.900 |
| Schedule meetings and events | 112 | 38.4% | 28 | 25.7% | 84 | 45.9% | 0.001 |
| Talk to family/friends | 261 | 89.4% | 94 | 86.2% | 167 | 91.3% | 0.178 |
| Send messages to family/friends | 252 | 86.3% | 91 | 83.5% | 161 | 88.0% | 0.280 |
| Others | 14 | 4.8% | 5 | 4.6% | 9 | 4.9% | 0.898 |
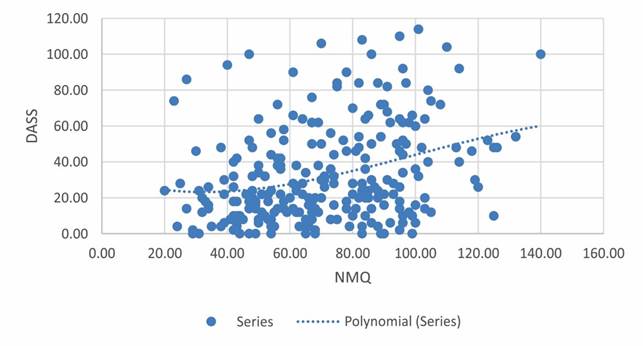
When analyzing the correlation of NMP-Q scores with DASS-21 scores, it is observed that increases in these scores lead to increases in the overall DASS score (p<0.001) (Chart 1), as well as in each of the domains of depression (p<0.001), anxiety (p<0.001) and stress (p<0.001).
Finally, when analyzing the association between the DASS-21, in its domains, and API, it was verified that the first tertile of API, which represents the students with lower performance, shows higher scores and worse results of DASS-21 in all evaluated domains. The mean anxiety score in students at the first tertile is 9.9, against 6.3 in students in the top tertile (p-value of 0.044), and the prevalence of severe or very severe stress is 31.6% in students at the first tertile, being about two-fold that found in students at the third tertile (16.2%),with a p-value of 0.035 (Table 3).
Table 3 Association of measures in the evaluated domains of the DASS-21 and API tertiles.
| API in tertiles | ||||
|---|---|---|---|---|
| First | Second | Third | p-value | |
| n (%) or mean ± standard deviation | n (%) or mean ± standard deviation | n (%)or mean ± standard deviation | ||
| Stress domain score | 18.1 ±12.35 | 16 ±9.98 | 14.7 ±9.33 | 0.223 |
| Anxiety domain score | 9.9 ±10.33 | 8 ±8.27 | 6.3 ±7.91 | 0.044 |
| Depression domain score | 10.1 ±9.87 | 9.3 ±9.94 | 6.3 ±6.6 | 0.059 |
| Stress domain in categories | 0.035 | |||
| Normal/Mild | 41 (40.5) | 42 (50) | 45 (52.3) | |
| Minimum | 13 (12.8) | 11 (13) | 12 (13.9) | |
| Moderate | 15 (14.8) | 17 (20.2) | 15 (17.4) | |
| Severe | 19 (18.8) | 7 (8.3) | 14 (16.2) | |
| Very severe | 13 (12.8) | 7 (8.3) | 0 (0) | |
| Anxiety domain in categories | 0.326 | |||
| Normal/Mild | 49 (49) | 45 (53.5) | 56 (65.1) | |
| Minimum | 6 (6) | 9 (10.7) | 8 (9.3) | |
| Moderate | 19 (19) | 14 (16.6) | 11 (12.7) | |
| Severe | 11 (11) | 8 (9.5) | 4 (4.6) | |
| Very severe | 15 (15) | 8 (9.5) | 7 (8.1) | |
| Depression domain in categories | 0.203 | |||
| Normal/Mild | 56 (56) | 53 (62.3) | 64 (75.2) | |
| Minimum | 16 (16) | 10 (11.7) | 9 (10.5) | |
| Moderate | 12 (12) | 11 (12.9) | 9 (10.5) | |
| Severe | 7 (7) | 5 (5.8) | 1 (1.1) | |
| Very severe | 9 (9) | 6 (7) | 2 (2.3) | |
DISCUSSION
The present study analyzed the relationship of nomophobia with depression, anxiety, stress and API. A total of 292 students attending the 1st to the 8th semesters of the medical course at Centro Universitário Christus, in Fortaleza, Brazil, were evaluated. Our sample consisted of students of a wide age range and male and female. There was an important association of nomophobia with levels of anxiety, depression and stress, and the last three were associated with worse academic performance. Moreover, it was found that the cell phone uses most often associated with the worst performance are checking the e-mail and scheduling appointments.
It was demonstrated in our study that medical students had a positive correlation between Nomophobia and Depression, that is: the higher the nomophobia scores, the greater the depression level. Corroborating our findings, in a study conducted with 329 American students, it was shown that problematic smartphone use is related to the severity of depression18. Demonstrating the correlation found in the present study, another study carried out with nursing students in India, also showed that nomophobia increases the levels of depression due to the pressure the individual suffers from being continuously connected19. Furthermore, also reinforcing our findings, in a Chinese systematic review and meta-analysis of a total of 13 studies showed a correlation between problematic smartphone use and depression20. This evidence suggests that there is a likely correlation between increased smartphone use and depression.
In addition to these previously demonstrated findings, a study showed that students who show prolonged smartphone use (>4h) have a lower academic performance. Moreover, it was observed that students who use their smartphone to look at e-mails and schedule meetings and events have a higher academic performance, with an API > 7.8 on average. This fact may be due to a more responsible use of the smartphone, as it is likely that using the smartphone to schedule meetings and check e-mails are eventual checks on the cell phone, that is, there is no feedback, so that the student spends less time connected. The role of the smartphone in academic achievement is currently the subject of several studies. In a study carried out with a large-scale survey in a public Chinese university, a correlation was found between the exacerbated use of smartphones and the students’ negative academic performance, through nomophobia21. Differently from the abovementioned findings, an investigation that used the same research instrument as the present study (NMP-Q), with a sample of 157 students, did not find an association between smartphone use and worse academic performance among students from a Physiotherapy course5. In the present study, no direct correlation was found between nomophobia and API; however, an indirect correlation was demonstrated, since students with low API show a correlation with anxiety, which, in turn, is statistically correlated with nomophobia.
As demonstrated in this study, a statistically significant association was found between Nomophobia and Anxiety, showing that students with high levels of nomophobia tend to have higher levels of anxiety. This relationship was reinforced in a systematic review including 42 articles, using the same instrument used in the present study for measurement (NMP-Q); in the vast majority of the studied articles, a positive correlation was found between nomophobia and anxiety22. The exacerbated use of smartphones and its relationship with this nomophobia as seen in our article is being studied worldwide. In an analysis carried out in China with adolescents, the existence of an important association between social anxiety and smartphone dependence was proposed23. Confirming the data found in our article, the use of cell phones has been described as being associated to high levels of anxiety, with time of use being the main associated factor24.
In addition to the relationship between nomophobia and anxiety, the present study showed that the individuals’ stress levels were also correlated with nomophobia, that is, the higher the levels of the former, the higher the levels of the latter. Such association implies believing that the exacerbated use of smartphones leads to stress mechanisms, having a significant impact on the individual’s quality of life and mental health. A systematic review and meta-analysis carried out with 41 articles showed that problematic smartphone use increases the levels of perceived stress among students22. Furthermore, an investigation of 270 smartphone users showed that nomophobia and stress have an intrinsic association, demonstrating a correlation between nomophobia, stress and working conditions8.
Some findings of this study show that depression, anxiety and stress are correlated, and the greater the one, the greater the levels of the other two conditions. Corroborating our findings, an investigation evaluated depression, anxiety and stress among medical students in India and found a high correlation between these three conditions in the sample, considering these diseases probably have a pathophysiological correlation among each other. On the other hand, in an investigation carried out with medical students conducted in Nigeria, no correlation was found between depression, anxiety and stress25.
This study has some limitations. The most important one is probably the use of the cross-sectional methodology, which can lead to reverse causality. We believe this is not the case in the present study, as we have evaluated students since the first semester (this being the most representative group), so the impact of API on the generation of stress, anxiety, depression or nomophobia is not likely a temporal one. We had an acceptable rate of missing values, and we used sensitivity analyses that showed little effect on the associations. As this was a self-administered questionnaire, one could experience information bias, but during the application, the confidentiality of information was guaranteed. Finally, although the API is not a perfect measure of academic performance, it is able to record student achievement in an acceptable and stable manner.
CONCLUSIONS
Our study suggests that nomophobia may likely increase anxiety and consequently lead to lower academic achievement. Therefore, educational technology policies are of the utmost importance inside the academic environment, aiming to warn students about abusive use, addiction occurrence and to help students to seek a therapeutic plan. Furthermore, our study observed that nomophobia is correlated with anxiety, depression and stress. Educational institutions need to alert students and help them with this problem, as these comorbidities can lead to extremely harmful consequences for the individual, such as suicide. Moreover, further studies will be needed to confirm the findings of this study and thus, this subject can be more effectively dealt with.

