











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por email
 Permalink
Permalink
INTRODUCTION
Learning can be defined as the process of acquiring knowledge, skills and attitudes aimed at a behavioral change1. It is an eminently personal, experiential process that presupposes a change in behavior2. The particularities in the adult learning process, in relation to the child, has defined a new field of studies, andragogy. For scholars in the area, the adult needs to understand the reason for the need to learn something, bringing with it the influence of previous experiences. Adult learners are more thematically and more specifically oriented, focused on real tasks and problems, and have an internal motivation to improve2)-(4.
Knowles, Ill and Swansom2 define adult learning as self-directed, when the individual takes the initiative themselves, with or without help from others, assessing their learning needs, defining their own objectives, implementing their own learning strategy and evaluating outcomes. Another important aspect of adult learning is highlighted by Kolb5, who highlights the experiential learning cycle (Figure 1 and Chart 1). For the author, this process is influenced by the learner’s personality, educational specificities, professional career, role in their work and adaptive skills. In this sense, knowledge is generated by the experience transformation, in which first there is a concrete experience or lived event, which brings observation and reflection, followed by the conceptualization of what occurs and its assimilation, thus modifying its performance5.
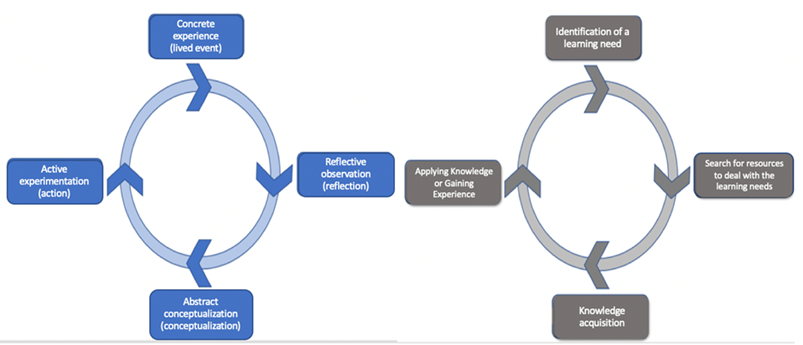
Chart 1 Comparison of explanatory learning models.
| Kolb’s Learning Cycle5 | Slotnick’s Physician Learning Sequence7 |
|---|---|
| Concrete experience | Identification of a learning need |
| Reflective observation | Search for resources to deal with the learning needs |
| Abstract conceptualization | Knowledge acquisition |
| Active experimentation | Applying knowledge or gaining experience |
A deeper understanding of the process of learning and building knowledge is particularly important for the development of professionals whose training process does not end with academic activities, as in Medicine. Physicians experience learning opportunities on a daily basis. In their continuing education, the use of everyday issues, combined with real experiences, both positive and negative ones, are considered key points for their interest in acquiring knowledge6. A classic study by Slotnick, in the late 1990s, shows an analysis of the physician’s self-directed learning, depicting four steps (Figure 1): identification of a learning need, search for resources to deal with the learning needs, the acquisition of knowledge and the application of knowledge or gaining experience7.
It is understood that more passive interventions, such as classes and conferences, tend to have little interference on physician performance and patient care outcomes. The time between continuing education efforts, such as courses and training, also seem to be inversely correlated with physician performance. In other words, the longer they go without new training, the worse their performance is, reinforcing the continuous and permanent nature of the training8),(9. Continuing education, in medical practice, is defined as any means by which the physician learns after completing their formal training, as a way to allow changes in their practice10),(11.
Currently, the easy availability of information and rapid changes, combined with the use of technological resources to enhance learning highlight the learner’s role and refer to self-determined learning, which reinforces the inclusion of aspects such as capacity, creativity and self-efficacy4. The dissemination of mobile devices has brought on a new reality for medical students and physicians12)-(14. Distance learning (DL), using problem-based learning methodologies, is capable of enabling the acquisition of skills and knowledge in remote areas and reaching many individuals, with similar outcomes to those of the in-person model15)-(17.
Primary Health Care (PHC) has distinct characteristics, expanding aspects for the training of undergraduate and graduate medical competences. In it, the student is able to experience the relationship of the individual, their community in a territory, the expansion of the clinical scope and its integration with other knowledges and professionals, having contact over time as an ally during this process18),(19. Different from the hospital-centric aspect, cultural aspects, popular knowledge and the individuals’ relationship with their territory are important factors in PHC18.
Brazil, since the introduction of the National Curricular Guidelines (NCG) in 2014, defines the generalist medical training, with distinct competences in the area of health care, health management and health education. This training process favors the Brazilian Unified Health System (SUS, Sistema Único de Saúde) and, particularly, training to work in PHC. On the other hand, these recommendations have disclosed faculty deficiencies in the training institutions, regarding the infrastructure of practice fields and in the way PHC health teams work20. The deficiency of the undergraduate training perceived in the practice of PHC work reinforces the need for improvement and the provision of postgraduate training21),(22. These actions are conducted by Federal Universities, which offer free continuing education processes using the distance learning model as advanced training, qualification or specialization courses, providing permanent education opportunities that can fit the learning needs identified by health professionals. Therefore, the learning strategy is focused on know-how, in which learning objectives are centered on everyday actions and provide learning for practice17),(23),(24.
There are few national studies that have assessed the learning process in physicians and these professionals’ perception of the individual learning process. In the context of strengthening and rapid expansion of PHC services registered in Brazil in recent years, it is relevant to know the perceptions of physicians who work in these services about self-learning. This information can facilitate the continuing education process for these professionals, potentiating the actions of health managers and reducing costs. Therefore, the aim of this study was to analyze the social representations of physicians working in PHC teams on self-directed learning.
METHODS
This is an exploratory, descriptive, quantitative-qualitative study, having as theoretical reference the Theory of Social Representations25, through the structural approach of the Central Nucleus Theory (CNT). This approach was chosen because it provides, through its propositions, a conceptual, theoretical-methodological refinement for the study of social representations. Knowing the social representations makes it possible to uncover the common knowledge of a social group. This knowledge brings the real experience and significance of this object, allowing the understanding of the learning process in which these participating individuals are included26.
The study was conducted in the municipalities of Ouro Preto, Mariana and Viçosa, in the state of Minas Gerais, Brazil. There was no sampling process. Data collection was carried out through a census, considering all 73 potential participants, which corresponds to the group of physicians who are registered and work in the Family Health Strategy (FHS) teams in the municipalities. The subjects included in this study are physicians who have been working for at least six months and are registered in FHS teams in the municipalities included in the study, both in rural and urban areas. Faculty or preceptors of undergraduate students in the health courses area were excluded, as well as those who were on leave due to vacations, medical or sick leave.
Data collection for the study was carried out by two interviewers, through a questionnaire created by the researchers, containing closed and open questions. The closed questions sought to characterize the interviewees regarding professional sociodemographic aspects and academic background. The open questions were used with the free-word evoking technique, and the inducing term was ‘medical self-learning’27. Each participant was asked to produce five words, expressions or adjectives that came to their mind, based on the presentation of the inducing topic. Subsequently, the participant had to point out which word or expression was the most important among all and, lastly, why that choice was made. The three open questions were recorded and later transcribed for analysis. By analyzing the spontaneously spoken words, it is possible to collect elements that constitute the representation content, according to Abric28),(29.
Data related to the sociodemographic profile and academic background were analyzed by simple descriptive statistical analysis using the software IBM SPSS 23.0 for MAC. Data from the free word evocation technique with the inducing term ‘medical self-learning’ were analyzed using the Pierre Vèrges’30 four-quadrant chart, which was constructed with the aid of the software Ensemble de programmes permettant l’analyse des evocations (EVOC®), version 200527.
Then, a similarity analysis was performed using the hierarchical similarity tree created with the aid of the software Classification Hiérarchique Classificatoire et Cohésitive - CHIC® (Version 4.1). For this analysis, this study considered all evocations present in the four-quadrant chart. The CHIC® software considered as significant similarity in this study the similarities between 0.5 and 1.00.
Finally, the analysis of the documented records was conducted based on the answers to open questions about the main word or expression of the evocation. The technique used was the Content Analysis31.
All ethical aspects were respected during the development of this study. The project was approved through Opinion number 3.040.247/2018 by the Research Ethics Committee, appropriately registered by the National Research Ethics Commission (CONEP, Comissão Nacional de Ética em Pesquisa). The managers of the municipal health secretariats of the municipalities included in the study, as well as the participating physicians signed the free and informed consent form. The privacy and confidentiality of the information were guaranteed to the participants.
RESULTS
Fifty interviews were carried out from December 2018 to February 2019, in the three proposed municipalities. Of the 23 non-interviewed individuals, three refused to participate and 20 met the exclusion criteria, such as being on vacation leave and working mainly as a preceptor to undergraduate students.
There was a slight predominance of females among the study participants, with age ranging from 25 to 54 years. The time elapsed since graduation in medical school was on average 64.1 months, with a maximum time of 300 and a minimum of 6 months. Regarding the title, approximately two-thirds of the physicians were general practitioners (Table 1).
Table 1 Profile of the interviewed physicians; Ouro Preto/Viçosa/Mariana, Minas Gerais, 2018.
| Variable | N | % | |
|---|---|---|---|
| Gender | Female | 27 | 54.0 |
| Male | 23 | 46.0 | |
| Total | 50 | 100.0 | |
| Age range | 20 to 30 years | 26 | 52.0 |
| 31 to 40 years | 16 | 32.0 | |
| > 40 years | 8 | 16.0 | |
| Total | 50 | 100.0 | |
| Time since graduation | Less than 1 year | 8 | 16.0 |
| 1 to 5 years | 26 | 52.0 | |
| 5 to 10 years | 8 | 16.0 | |
| > 10 years | 8 | 16.0 | |
| Total | 50 | 100.0 | |
| Time working in FHS | Less than 1 year | 9 | 18.0 |
| 1 to 5 years | 29 | 58.0 | |
| 5 to 10 years | 6 | 12.0 | |
| > 10 years | 6 | 12.0 | |
| Total | 50 | 100.0 | |
| Municipality where they work | Ouro Preto | 19 | 38.0 |
| Viçosa | 17 | 34.0 | |
| Mariana | 14 | 28.0 | |
| Total | 50 | 100.0 | |
| Title | Generalist | 29 | 58.0 |
| Specialist | 20 | 40.0 | |
| Master’s Degree | 1 | 2.0 | |
| Total | 50 | 100.0 |
Of the participants, 50% reported working in some activity rather than the FHS and 60% of the respondents did some activity related to learning. Of those who had labor activities in addition to the FHS, almost 70% reported emergency care activities in hospitals and Emergency Care Units (UPA, Unidade de Pronto Atendimento). Of those who reported participating in learning-related activities, about a third of the respondents were doing medical residency in Family and Community Medicine and the same proportion participated in distance learning (DL) activities.
Regarding the data comprising the evocations of the 50 interviewed physicians, 248 words or expressions were produced, with 122 different words or expressions and an average of 4.96 words or expressions per participant. The mean of the Average Order of Evocation (AOE) was considered for this construction, that is, the “rang” equal to 2.7, while the average frequency was set at 7 and the minimum at 4.
The analysis of the evocation results indicates the structuring trends (central and peripheral cores) of the social representation of the interviewed subjects. The interviewees more quickly and frequently associated the representation of self-learning with the following 16 evocations: knowledge, dedication, study, reading, necessity, internet, practice, time, scientific articles, confidence, case discussion, experience, interest, improvement, book and research.
In the upper left quadrant represented in Figure 2, which consists of the elements considered as likely to be central, are the expressions: “knowledge”, “dedication”, “study”, “reading”, and “necessity”, being the possible core elements of the Social Representation (SR) of the assessed physicians about medical self-learning.
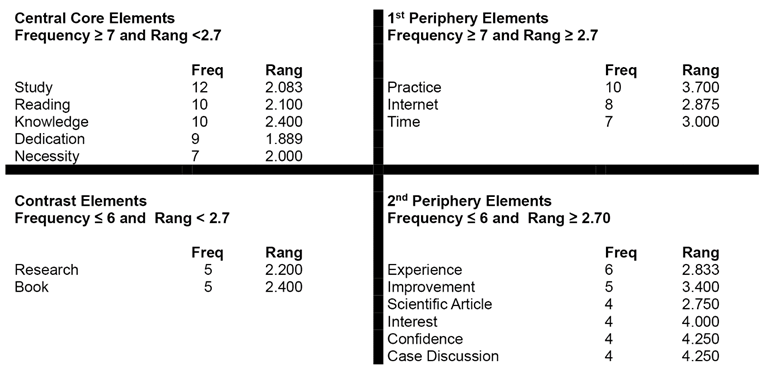
Figure 2 Four-quadrant chart frequency: distribution and average rank order generated by the Rangfrq of the EVOC® software of the database: physicians interviewed in 2018.
The first and second peripheries comprise seven evocations: “internet”, “practice”, “time”, “scientific articles”, “confidence”, “case discussion”, “experience”, “interest”, “improvement”.
Subsequently, the 16 evocations present in the four-quadrant chart were submitted to hierarchical similarity analysis generated from the CHIC software, creating the Hierarchical Similarity Tree shown in Figure 3.
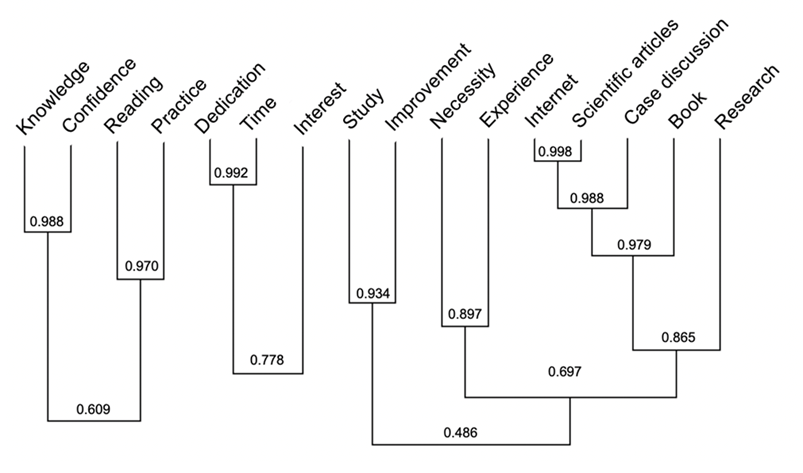
Figure 3 Hierarchical similarity tree of the categories generated by the CHIC® software from the database of physicians assessed in 2018.
It can be observed in the similarity tree that there are three large groups that do not show any connection with each other, one comprising “knowledge”, “confidence”, “reading” and “practice”; the second consisting of “dedication”, “time” and “interest”. And, finally, a larger group comprising “study”, “improvement”, “necessity”, “experience”, “internet”, “scientific articles”, “case discussion”, “book” and “research”.
The expression “study” appears in the central core and was the most frequently evoked word (12 times) with a “rang” of 2.083 and, in this research, it was associated with Study as a resource/tool for updating and improving patient care; a proactive and often solitary action, a connotation of theory acquisition; as a synonym for scientific research and its product;
[...] We need to study to... to learn, so...yes...you really need to read, you really need...yes...to sit down in order to learn. I had a background that was...it was not that traditional. My training was by PBL. And we had that a lot... yes... your study is very lonely, your study, you do not have many people to help you. You... are... you yourself go there and look for what you are seeking. I think that is why... that is why it came to my mind at this time that studying is the most important. (Interviewee 28)
[...] Because it’s the act itself, you have to start, you have to look for it. The book is there, the knowledge is there, the information is there, you have to look for it, it starts with you. So, I believe this is the most important part that has to start with me. (Interviewee 18)
The expression “reading” appears in the central core and was the second most frequently evoked word along with knowledge (10 times) with a “rang” of 2.1 and, in this research, it was associated with an action for those seeking knowledge, such as the path to theory.
[...] we always have to try to learn increasingly more, through reading, these distance learning courses, because there is always something we can learn. (Interviewee 9)
[...] Reading provides the training for the performance of medical actions and acts. Also important for improvement and updating. (Interviewee 47)
The expression “knowledge” appears in the central core and was the second most frequently evoked word (10 times) with a “rang” of 2.4 and, in this research, it was associated with base, substrate, foundation for evolution, being something that is continuously acquired and as something that is infinite, which cannot be depleted. It is considered an accumulation of experience and can be transmitted.
[...] we always have to try to learn increasingly more, through reading, these distance learning courses, because there is always something for us to learn. (Interviewee 9)
[...] evolution is the opposite of stagnation. So when I think about learning,...it is precisely this search, permanent and continuous search for information, right, for knowledge... so this is the way for us to evolve as human beings, as professionals. (Interviewee 38)
The expression “dedication” is the fourth evocation of the central core, with a “rang” of 1.889, which was evoked 9 times and, in this study, it was associated with a characteristic of the individual of renouncing something to keep the focus, stay motivated, and is related to an inner strength, also the idea of purpose, as only those involved are dedicated and know why.
[...] we have to organize and have management, an organization of study over time so we do not to stop doing other things. To have a social life, to rest, to practice physical activity. (Interviewee 11)
[...] and dedication...if I want to dedicate myself, I have to be more about it...you have to be well aligned to get on with it, because if you do not, you can’t. We lose... as I have seen many times, people going and not being able to continue. It depends a lot on us. Willpower and motivation. (Interviewee 37)
The expression “necessity” is the fifth evocation of the central core and a “rang” of 2.000, which was evoked 7 times. In this study, the expression was associated with an inconvenience generated by changes, by the desire to perform a good practice, creating a necessity.
[...] I believe it is necessary to update oneself, medicine is changing all the time and there is this need. (Interviewee 7)
[...] even if you know that it is important and necessary... it does not flow, from my point of view, right... if you do not know why you’re doing it. (Interviewee 11)
The expression “practice” is the first evocation of the 1st periphery, which was evoked 10 times with a “rang” of 3.700, as a stimulus for learning and for its fixation, as a counterpoint to theory, as a “validator” of the theory.
That the practice that generates the demand for me to study that. For instance, today I treated a case for which I did not know 100% of the best conducts to be taken, right; this will lead me to seek new knowledge. Thus, I see the practice as a stimulus to seek new knowledge, take new courses, look for new books, new...new...follow new paths. (Interviewee 6)
Because I feel like in my... I learned more in practice. By practicing medicine, with these practices. I think I learned more from the patient, mainly in family health, a very psychological part. I learned more about dealing with the patient, with medicine. (Interviewee 19)
The expression “internet” is the second evocation of the 1st periphery, which was evoked 8 times with a “rang” of 2.875. Although evoked, it does not explicitly appear in the speeches, but it was considered a democratic, easily accessible locus, with a lot of content and information.
Because that is where, I think, there is more content to seek. And where you have more information with access. (Interviewee 23)
The expression “time” is the third evocation of the 1st periphery, which was evoked 7 times with a “rang” of 3.0. It brings the idea of a finite resource in the speeches, requiring management; moreover, it brings the idea of accumulation in the form of experience.
Due to the issue of time nowadays... and priorities in medicine, right... the issue of work, excess, [...] the amount of information we have... and dedication... if I want to dedicate myself, I have to be more in relation to that... you have to be well aligned to get on with it, because if you do not, you can’t. We lose... as I’ve seen many times, people going on and not being able to continue. It depends a lot on us. Willpower and motivation. (Interviewee 37)
Because over time, as you graduate, you come out inexperienced. You go looking for knowledge and improves. Always improving, otherwise you become outdated. (Interviewee 42)
The expression “experience” is the first evocation of the 2nd periphery, which was evoked 6 times with a “rang” of 2.833. One can perceive a sense that experience is the result of experimentation, a repeated practice leading to consolidated learning.
Because I think that through... the experimentation, right... the experience [...] I think more or less in this sense... that then you can have all your learnings, [...] it is no use at all the fact that you want to study, for instance, something that you are not there, having this experience, right... that will end up being lost... that is not fixed in the memory. (Interviewee 34)
The expression “improvement” is the second evocation of the 2nd periphery, which was evoked 5 times with a “rang” of 3.4. Its meaning, in the speeches, is to become more complete, able to carry out the work more fully, to have more knowledges and experiences.
It’s the objective [...] we want to learn, more...and [...] we want to specialize and learn more, improve more, so, in the medical case, to optimize patient care and improve your work; in my case, here inside the health unit, for instance. (Interviewee 39)
The expression “scientific article” is the third evocation of the 2nd periphery and was evoked 4 times with a “rang” of 2.750. It reinforces an idea of confidence, as it is something “scientific”, in addition to being more current and applicable to a more “real” situation, it brings an idea of evidence, once again constituting a sense of something that is more practical and less theoretical.
Because evidence-based medicine takes into account both the scientific part, right, which are the articles published on the subject, as it takes into account what we see in our daily lives. Then, sometimes, I have a certain option of a treatment or a... a... a diagnostic tool for a case, right... to diagnose a specific disease, let’s suppose... but in that one... in my specific case, in my work environment, for that specific patient, I could not use it. So evidence-based medicine, in addition to bringing what is top knowledge, in terms of innovation and what is best for the patient, it adapts to the situation. So, for me, it is the most important thing. (Interviewee 30)
The expression “interest” is the fourth evocation of the 2nd periphery and was evoked 4 times with a “rang” of 4,000. Its meaning is more associated with in the word ‘interesting’, something that arouses one’s curiosity, the unknown that exists as a desire to become known, the opposite of simple, being the complex, the most interesting, difficult.
Although there are diseases that we end up thinking are not important, but they are very important, just because they are very prevalent. [...] Medicine is like that, right... some colleagues, I do not know if all of them. I think there are many who also like it, right. You think, for instance, that hypertension is not interesting, but you see that many people even have difficulty to manage hypertension... (Interviewee 12)
The expression “confidence” is the fifth evocation of the 2nd periphery and was evoked 4 times with a “rang” of 4,250. In the speeches, the word confidence does not appear, but some speeches in which the expression was evoked seem to indicate the sense of feeling safe to take an action.
Because based on knowledge, I will feel confident to take action, make the correct diagnosis, manage the patient and feel like a more complete professional. (Interviewee 43)
The expression “case discussion” is the sixth evocation of the 2nd periphery and was evoked 4 times with a “rang” of 4,250. It points to the sense of contextualization and idea structuring format, in addition to a perspective of exchanging experiences with another person.
[...] when you’re discussing a case[...] it seems that you... you assimilate more, you... more doubts arise. When you are going to explain something, also any doubts... a colleague of yours is discussing with you. (Interviewee 25)
The first element of contrast is the word “research”, evoked 5 times with a “rang” of 2,200. The word brings the meaning of the search for knowledge, of structured actions to find some information.
[...] But with me it is like that, I think you only assimilate it when you are there researching and experiencing that, right... then, in a way, if that brings you any doubts, you will research, you will want to know, you will study, right... and from that point on, it gets fixed in your memory... (Interviewee 34)
The second element of contrast is the word book, which was evoked 5 times with a “rang” of 2,400; it brings the sense of a source of knowledge, the objectification of the theoretical, as a contrast to what is “outside of the book”, which brings the idea of practice.
The book is there, the knowledge is there, the information is there; you have to seek it, it starts with you... (Interviewee 18)
[...] in the consultation itself, there is something that we do not see in a book and we sometimes see it during a consultation... (Interviewee 9)
DISCUSSION
The analysis of the results allows us to infer that “knowledge” is the objective to be achieved by the physician who directs their learning. It brings “confidence” to “practical” actions and the more experienced they become, the more they accumulate knowledge and confidence. Kolb5 reinforces this concept by explaining the learning cycle, demonstrating that adult learning is based on experience, followed by reflection, conceptualization and new interaction. For this process, the meaning that the study physicians bring on is that individual characteristics of “dedication”, “interest” and “motivation” are essential factors for change and, in this case, an “improvement” of their performance. Knowles, Ill and Swansom2 verify that adults can be influenced by external motivational factors, such as better remuneration and jobs; however, internal motivational factors such as personal satisfaction, accomplishment in what they do, meaning in what they do, influence more the adult to learn, as shown by the analyses.
The first periphery of the social representations identified here shows procedural aspects of the search for knowledge. The interviewees point out that searching or “researching” for new information, which can occur through the “internet”, by reading “books” and/or “scientific articles” or “case discussion” help in the theoretical consolidation, or “study”, and its application in “practice”. Kolb5 shows, in the Experiential Learning Theory, the so-called conceptualization, that after living and reflecting, the adult seeks to consolidate knowledge for a new application. This concept, also present in the definition of SR, is reinforced by the first periphery, as shown in the results.
The “practice”, which appears in the first periphery, lives up to its effect of strengthening the central core because, based on the participants’ understanding, it is where the perception of knowledge necessities is triggered and, at the same time, when knowledge is consolidated - or its application. If some knowledge is applied satisfactorily in practice, it brings confidence, it generates experience. In adult learning, the orientation for learning focused on tasks to be performed or problems is defined, which make more sense for the student to face their reality, as also explained in the results regarding the performance in practice in environments aimed at the resolution of most of the problems2),(3),(32),(33.
It is also reinforced, in some speeches, that the result of the practical application is also an increase in the resolution of problems and satisfaction of the person being attended, an important conceptual factor in professionals working in PHC, who deal with complex problems, take care throughout time and, ideally, show a high level of effectiveness32. This aspect is also explained in the results regarding the practical work to solve most of the problems. The continued care of people in PHC makes the patient always return to this level of care whenever their problem has not been solved2),(3),(32.
Another very important element of the first periphery is “time”, pointed out both as a scarce resource by physicians and as a factor for measuring “experience” (those working on something for a longer time would have more experience). It reinforces core elements such as “dedication”, in the sense of “spending” time to develop knowledge in reading and studying. Moreover, considering the fact that self-learning is a necessity, as the doctors point out, time needs to be preserved and prioritized, as it is considered a scarce resource. Therefore, it ends up being considered a barrier as well. Heutagogy also reinforces the influence of time, both as a limiting factor and as a measure of what the student wants to learn and, therefore, they dedicate themselves to what makes sense and seek to direct their own needs. Time as a barrier, such as it occurs in the social representations of the study physicians, is also mentioned by Knowles as an obstacle or motivation blockade2)-(4.
The contrast zone of the four-quadrant chart consists of elements with low frequency but considered important by the subjects. Therefore, they reinforce the concepts present in the first periphery, being able to point out the contrast of some element that is being missed by a social representation or indicate the existence of a minority subgroup carrying a different representation34. In the present study, the word “research”, as the search for information, seems to reinforce several aspects of the first periphery, such as the “internet”, a possible locus of research. The word “book”, considering its space in the social representations of these subjects (contrast zone), seems to demonstrate that learning through books, as a source of consultation, of research, may be an element that might soon come out of this representation. On the other hand, it can also be indicative of a minority subgroup. The difference in age and education could be a relevant factor for such possible subgroups. Slotnick7 described the source of studies through the reading of medical journals, publications and books as less structured and informal permanent education modalities. The use of mobile devices and digital access to information is a reality, and it has changed the relationship with books12)-(14, a phenomenon that is compatible with a probable change in SR.
The results show that about a third of the participants who performed some activity related to distance learning, a fact that, associated with a context of abundance of information, may reflect the “necessity”, as shown in the interviews, of not being outdated, of keeping up with the evolutions of knowledge. It should be considered a warning the fact that the other learning activities mentioned by the physicians demonstrate educational formats with an instructional design more focused on the teacher’s needs to meet learning objectives and less on the autonomy advocated by heutagogy authors4),(35.
CONCLUSIONS
The way physicians learn has been changing with the inclusion of technology both for care and for knowledge acquisition. Evidence-based practice reinforces the need to create competences related to learning and not just knowledge, since the professional has to creatively deal with the scarcity of time, changes in scientific evidence and excess of information, which may not be reliable or require cautious interpretation.
Although permanent education is at present predominantly based on guidelines, summaries of evidence and protocols, “scientific articles” carry a symbolism of power and scientific evidence that is confused with the very search for knowledge as a validation mechanism for clinical practice. Medical knowledge implies applying knowledge for the care of those who come to consult, supporting and empowering their practice within a socially constructed and culturally recognized locus, precisely through the process of knowing how to access and interpret this information.
It is necessary to expand knowledge about more autonomous forms of learning that do not involve only the teacher-centered environment, with distance learning being such an example. This premise is especially true in PHC, in which the physician finds little opportunity for discussion with his professional category peers, given the isolation of each unit, when compared, for instance, with specialty clinics or hospitals. It is worth pointing out here the limitation that the absence of exchanges between peers brings, placing the model based on individual practices as a form of learning. On the other hand, the ability brought on by the internet to connect with other professionals and collaboration also bring different elements for a broader and more satisfactory training into this reality.
The need to understand how this learning process determined by the individual occurs and how the influence of individual and social factors and context can provide better training and inclusion in formal training curricula, such as undergraduate and graduate school, is emphasized. This process will necessarily take place by the fundamental task of teaching physicians to learn, that is, teaching them how to access information, evaluate its quality, analyze the evidence and apply it to the current situation, grounding their practice on the best available information, establishing contextual and meaningful learning. Additionally, they should be able to self-assess, improving their ability to learn in a continuous and effective manner.

