











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por email
 Permalink
Permalink
INTRODUCTION
Since 2011, the National Curriculum Guidelines (DCN) for the medical course emphasize the training of a generalist professional with general and specific competencies, as well as who should be able to exercise good-quality medical practice1. With the DCN, the change in medical education aims to break the pattern of learning focused on hospitals and transfer it to basic health units2.
The central issue of medical training must be to guarantee the development, during undergraduate school, of the competencies necessary to meet the population’s health demands and needs with quality1. However, the super-specialization of Medicine makes the professionals more restricted and limited to their area. Thus, generalist training, in line with the new guidelines, wants to become broad and at all levels of health care2.
However, although there is a new focus on training professionals with a generalist profile, almost all medical courses follow the traditional medical training curriculum, which is based on the Flexner report. The courses are divided into a basic cycle, clinical cycle and internship without content integration and without a comprehensive view of the patient3.
In addition to the non-integration of medical education in undergraduate courses, the fact that general practitioners cannot perform certain diagnostic and therapeutic procedures contributes to a super-specialization, with professional value being associated to the acquisition of knowledge, the accumulation of learning and the use of technology.
Aiming to reduce the influence of the biomedical teaching model based on the Flexner report, some universities have already adopted the Problem-Based Learning (PBL) teaching model, which seeks to understand the patient’s history and use it to favor the diagnosis and treatment. The PBL method allows learning in a cognitive spiral and activities that enable the relationship between the biological, psychological and social dimensions4. Therefore, it promotes professional humanization by fostering an early relationship between the student and the patient through practice in basic health units, thus validating what the NCG predict.
Regarding the basic health units, Bland et al.5 carried out a comprehensive review of the literature on the choice to work in Primary Care after the medical course and demonstrate that the student enters medical school with a preference for Primary Care, but the priority changes, as they come into contact with the specialties during the course.
Furthermore, of the physicians working in Brazil, 61.3% have a specialist title, while the other 38.7%, the so-called general practitioners, do not, whether issued by a Society or via Medical Residency. It is noteworthy that among specialists, a relevant number of physicians have two or more specialties. Moreover, there are differences regarding the number of general practitioners and specialists in the different regions of the country due to age and gender, and six specialties concentrate half of the specialists: in addition to Internal Medicine (a specialty with the highest number of professionals, equivalent to 11.3% of all specialist titles), this group also includes Pediatrics, General Surgery, Gynecology and Obstetrics, Anesthesiology and Occupational Medicine. Thus, in Brazil, there are 55 recognized medical specialties and the trend is for the number of specialists to increase, due to the expansion in Medical Residency vacancies, among other factors6.
Several factors have been reported as having an impact on the choice of specialty among students. It is said that a lifestyle characterized by free time for leisure, family and recreational activities, with control of the total weekly hours spent on professional responsibilities, is a selection criterion for choosing the area. Moreover, studies report that this factor is more influential than remuneration and status7.
Therefore, the choice of the medical specialization has been an object of study, mainly because it has to be decided upon so early, at the beginning of the course. The lack of motivation for the practice of general medicine has worried managers around the world, in addition to going against the guidelines for training general practitioners8. The literature is still scarce regarding the factors that influence the choice for the generalist practice, including in the northeast of Brazil, given the great sociocultural diversity in the country.
Therefore, this study aimed to analyze the perception of medical students regarding their generalist training and the factors that influence the desire for professional practice. With these data in hand, intervention strategies can be developed, whether within a political or educational scope, aiming to change the current scenario.
METHOD
The present study is a quantitative, cross-sectional and descriptive exploratory investigation. The study was carried out from February 2019 to April 2019, and its target audience comprised medical students attending from the first to the twelfth semester of six educational institutions: 4 private and 2 public in the city of Salvador, state of Bahia, Brazil.
Population and data collection:
Participants were randomly invited by email or WhatsApp via cell phone to voluntarily answer a semi-structured questionnaire with 32 questions, via Google Forms, after signing the Free and Informed Consent Form (FICF). The questionnaire was developed by the researchers, in which the socio-demographic characteristics were analyzed, in addition to the perception of the curricular content in the generalist training, interest in specialization and generalist professional practice, as well as perspectives after graduation. The data were collected by the researchers, five medical students who are members of LAMEGE - Academic League of General Medicine.
A pilot study was carried out with 15 participants, who did not participate in the investigation, aiming to test the instrument, identify problems in understanding the questions, make changes to the questionnaire and thus contribute to the organization of the study.
Sample:
Among the eligibility criteria, the inclusion criteria comprised: being a medical student and being 18 years old or older. The exclusion criteria comprised: not signing the free and informed consent form, refusal to participate in the study and incomplete questionnaire. The eligibility criteria were included in the Google Forms, so that, when present, messages were blocked from being sent. All answers received were eligible.
Sample calculation:
For the sample calculation, a significance level of 5%, power of 90% and chance of 50% of each student participating or not in the study were considered; thus, the minimum sample size is 375 students. A total of 523 answers were obtained for the study.
Description of variables:
Definition of the term “General Practitioner”:
It is known that there is no consensus regarding the use of the term “general practitioner”, whether in national or foreign literature. The definition of “general practitioner” adopted in this study refers to a physician without a specialist title. As a reference, the study Medical Demography in Brazil 2020 was used, as a result of the Technical Cooperation Agreement between the Universidade de São Paulo (USP) and the Federal Council of Medicine (CFM), which defines the general practitioner as a physician with general training in Medicine, that is, the term “generalist” does not refer to the specialist in Internal Medicine, a recognized specialty whose title holder is called “specialist in Internal Medicine”, commonly called “general practitioner” or “clinician”. Being a generalist, in this study, also does not refer to the specialist in Family and Community Medicine.6
Statistical analysis:
Categorical variables were expressed as absolute and relative frequencies (percentages). Quantitative variables were evaluated using the Shapiro-Wilk test and described as mean and Standard Deviation (SD) if the distribution was normal, or median and Interquartile Range (IIQ) if the distribution was non-normal. All quantitative variables were categorized to test the association with outcomes. For the statistical analysis, the sample was categorized into two groups: IS, which are those who want Immediate Specialization, and WG, who are those who want to Work as Generalists.
In the questionnaire, the variable “course semester that you attend” was categorized every three semesters. To analyze the association between the course semester at the time of the interview, the sample was organized into two groups, the Initial Phase of the course (IP) represented by students attending the 1st to the 6th semester, and the Final Phase (FP) group represented by students attending from the 7th to the 12th semester.
Categorical variables were investigated through bivariate analysis using the chi-square test and Fisher’s exact test. Variables with p < 0.05 in the bivariate analysis were considered significant.
The SPSS v. 17 program was used to assemble the database and for statistical analysis, raising possible justifications for the collected data.
Ethical aspects:
All individuals in the present research were studied according to the precepts of the Declaration of Helsinki and the Nuremberg Code, respecting principles involving research with human subjects, in accordance with the National Health Council (Res. CNS 466/12). The project was submitted to the Ethics Committee for Research in Human Subjects at Hospital da Bahia (HBA) and approved under number 3,102,415.
RESULTS
Of the 523 study participants, 72.7% (n=380) are female and the respondents’ age ranged from 18 and 25 years in 83.7% (n=438) of the sample. Fifty-one percent (n=265) are from the city of Salvador and 49% (n=258) are from some municipality in the countryside of the state. About half, 51% (n=268) of the respondents have a family member working in the medical area. When asked about what motivated the desire to become a physician, 89% (n=465) said it was a vocation, while 5.7% (n=30) said it was for the remuneration and 4.2% (n=22) were influenced by their parents. Regarding the semester they were attending at the time of the interview, 24% (n=126) are in the group attending the 1st to the 3rd semester, 37.3% (n=195) are in the group attending the 4th to the 6th semester, while 32% (n=168) are in the group attending the 7th to the 9th semester and 6.5% (n=34) attend the 10th to the 12th semester. Of these, 90% (n=470) are studying Medicine as their first degree and denied having, at that time, any paid work, whether formal or informal. Of those interviewed, 82% (n=427) study at private educational institutions and 38% (n=199) receive some type of student funding.
When asked about the pedagogical model used in the educational institutions, 14.5% (n=76) of the students said they used the traditional model, while 40.7% (n=213) used the mixed method and 44.7% (234) used the Problem-Based Learning (PBL) methodology. (Table 1).
Table 1 General characteristics of the sample of medical students interviewed in the city of Salvador - BA.
| Variable | N=523 |
|---|---|
| Gender | |
| Female N (%) | 380 (72.7) |
| Age N (%) | |
| 18 to 25 years | 438 (83.7) |
| 26 to 35 years | 80 (15.3) |
| 35 to 43 years | 5 (1) |
| Birth place N (%) | |
| Capital city | 265 (50.7) |
| Countryside | 258 (49.3) |
| Has a family member who is a physician N (%) | 268 (51.2) |
| Has another degree N (%) | 53 (10.1) |
| Has formal or informal job N (%) | 55 (10.5) |
| Currently attending semester N (%) | |
| 1st to 3rd semester | 126 (24.1) |
| 4th to 6th semester | 195 (37.3) |
| 7th to 9th semester | 168 (32.1) |
| 10th to 12th semester | 34 (6.5) |
| Type of institution N (%) | |
| Private | 427 (81.6) |
| Pedagogical model N (%) | |
| *PBL | 234 (44.7) |
| Traditional | 76 (14.5) |
| Mixed | 213 (40.7) |
| Belongs to an academic league | 343 (65.6) |
| Receives some type of student funding N (%) | 199 (38) |
*PBL (Problem-Based Learning).
Of the students whose schools used the traditional model, 31.6% (n=24) believe that their curriculum completely contemplates the generalist training, while 53% (n=113) of those in the mixed model and 62% (n=146) of those who use the PBL model have the same perception, p<0.001 (Figure 1). The analysis of the role of educators in valuing the generalist performance showed that of the students who believe that their curriculum fully contemplates the generalist training, 65.4% (n=149) believe that their teachers value this proposal, while 38% (n= 62) think they value medical specialization and 54.5% (n=72) believe they are indifferent to it.
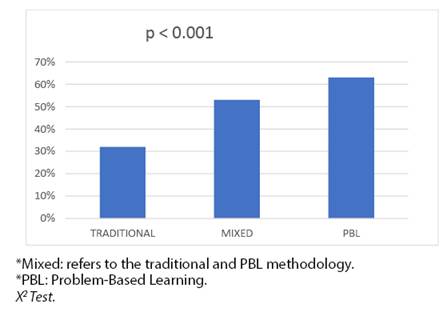
Figure 1 Influence of the pedagogical model on students’ perceptions regarding the generalist training.
The desire for specialization was present in 98.5% (n= 515) of students. The group that wanted Immediate Specialization (IS) was represented by 27% (n=132) and the group who initially wanted to Work as a Generalist (WG) was represented by 73% (n=381). Of these, 14% (n=73) have already decided on the specialization area even before starting medical school, while 17.3% (n=90) have decided during the course and 67.3% (n=352) have not decided yet. In the WG group, women represented 71.6% (n=273) of the sample and men 75.5% (n=108), while in the IS group, women represented 28% (n=107) and men 24.5%(n=35), P=0.399.
Of the students in the Initial Phase of the course (IP), 73.8% (n=237) belong to the WG group, while 144 (71.3%) belong to the group of students in the Final Phase of the course (FP), p = 0.524. In the WG group, 69.8% (n=139) receive some type of student funding and 74% (n=324) study with their own resources, p=0.227. When comparing the perception between the groups, it was found that 70.6% (n=320) of the WG group believe in medical residency as a curricular complement to medical training, as well as the students believe that the specialist is better paid when compared to the generalist, with RR: 1.03 (95% CI, 1.01-1.04), p=0.041, in addition to having better social status with RR: 0.63 (95% CI, 0.43-0.93), p =0.023 and have more credibility in society, with RR:0.66 (95% CI.0.45-0.98), p=0.044. (Table 2). When asked about the perception of the current labor market, 76.4% (n=400) believe that there is a lack of generalists, of which 74.8% (n=299) are from the WG group and 25.3% (n=101) from the IS group, p=0.078. The factors associated with the desire to work initially as a generalist were working at a public institution, RR: 1.77 (95%CI, 1.02-3.08), p=0.041; believing in the generalist’s capacity to solve problems at the end of the course with RR: 1.90 (95% CI, 1.21-2.99), p=0.005; believing in SUS guidelines RR:2.71 (95%CI 0.1.48-4.93), p=0.001; desire to contribute to society RR:1.71 (95%CI,1.17-2.56), p=0.005.
Table 2 Analysis of factors associated with the desire for immediate specialization (IS) and working as a generalist (WG).
| Variables%(N) | WG N=381 | IS N= 132 | RR CI (95%) | P& |
|---|---|---|---|---|
| Female gender | 72% (273) | 28% (107) | 1.20 (0.77-1.88) | 0.399 |
| Having a physician in the family | 71% (190) | 29% (78) | 0.81 (0.55-1.20) | 0.303 |
| Having another degree | 68% (36) | 32% (17) | 0.76 (0.41-1.41) | 0.395 |
| Semester attended | ||||
| Group IP (1st to 6th semester) * | 73.8% (237) | 26.3% (84) | 0.87 (0.58-1.29) | 0.524 |
| Group FP (7th to 12th semester) * | 71.1% (143) | 29% (58) | ||
| Participating in Academic Leagues | 73% (251) | 27% (268) | 1.04 (0.70-1.57) | 0.815 |
| Student funding | ||||
| Does not receive | 74.7% (242) | 25.3% (82) | 0.78(0.530-1.163) | 0.227 |
| FIES**/PROUNI***/ | 60.85 (139) | 30.2% (60) | ||
| Private Bank | ||||
| Teaching institution | ||||
| Private | 71% (303) | 29% (124) | 1.77 (1.02-3.08) | [0.041] |
| Public | 78% (78) | 18.8% (18) | ||
| Generalist’s capacity to solve problems | 76% (316) | 24% (102) | 1.90 (1.21-2.99) | [0.005] |
| Believes it favors the specialist: | ||||
| Job market | 72% (325) | 28% (127) | 0.68 (0.37-1.25) | 0.252 |
| Better valued by society | 67% (81) | 33% (40) | 0.68 (0.44-1.06) | 0.096 |
| Credibility | 68% (137) | 32% (65) | 0.66 (0.45-0.98) | [0.044] |
| Social status | 68% (161) | 32% (76) | 0.63 (0.43-0.93) | [0.023] |
| Remuneration | 72% (370) | 28% (142) | 1.03 (1.01-1.04) | [0.041] |
| SUS guidelines | 86% (87) | 14% (14) | 2.71 (1.48-4.93) | [0.001] |
| Desire to contribute to society | 78% (216) | 22% (61) | 1.71 (1.17-2.56) | [0.005] |
| BHU Infrastructure**** | 74% (312) | 26% (111) | 1.26 (0.78-2.03) | 0.336 |
| Lack of Job and Career Plans | 76.5% (162) | 23.5% (50) | 1.36 (0.91-2.03) | 0.130 |
| Scarcity of Public Service opportunities | 69% (18) | 31% (8) | 0.83 (0.35-1.95) | 0.655 |
& x² Test: RR (relative risk): CI (confidence interval) **FIES: fundo de financiamento estudantil (student finance fund). ***PROUNI: programa de universidade para todos (university program for all) ****BHU: Basic Health Unit.
[ ]: Statistical significance p<0.005. *IP (initial phase of the course). *FP (final phase of the course).
DISCUSSION
Health care in Brazil has undergone strong changes in the 1980s and 1990s with the creation of a universal system, the Unified Health System (SUS, Sistema Único de Saúde). Despite being the current public health care system, supported by the Federal Constitution of 1988 and regulated by the Organic Laws of 1990, there are still many obstacles to its consolidation. Its democratic principles deal with guidelines, concepts and practices that were and still are against the hegemonic model in society. The hegemonic system, the so-called Flexnerian model, presents health care centered on curative, hospital-centric and super-specialized care, based on economic and corporate interests. The replacement of this system by the universal system, which seeks care models that value comprehensive, humanized care and health promotion, depends on the training profile and practice of health professionals9.
The consolidation of the National Curriculum Guidelines (NCG) presupposes that the medical school progresses in the reorientation of the training process, integrating itself with health services, aiming at training generalist medical professionals who are determined and aimed at problem-solving, able to meet the needs of the Brazilian population and the operationalization of SUS9)-(10. According to item V of Article 29, the structure of the Undergraduate Medical Course must create learning opportunities, from the beginning of the course and throughout the entire undergraduate school process, with the Human and Social Sciences as a cross-sectional axis in the training of professional with a generalist profile11)-(12. Thus, Generalist Medicine must be the priority of medical training.
In line with the new NCG, the students interviewed in this study have dealt, since the first semesters of undergraduate school, with professionals and users of health services and, in general, they perceive that the curriculum includes generalist training. Regarding the pedagogical models, it was observed that respondents contemplate curriculums that show different types of models, including: traditional, mixed and PBL (Problem-Based Learning), and most of them are studying medicine using the full PBL model.
When analyzing the pedagogical models currently used in the medical course, there was a linear increase in the student’s perception of generalist training as the traditional pedagogical methods were replaced by active methodologies. The latter, such as the PBL, are anchored in critical pedagogy, working with problems for the development of teaching-learning processes and value the act of learning to learn13. They also meet two main requirements and changes in the NCG: increase in medical practices and the training of a physician who meets the SUS and Primary Care Policies, that is, a generalist physician13. Item II of Art. 29 of the NCG states that the structure of the Undergraduate Medical Course must use methodologies that favor the active participation of the student in the construction of knowledge and the integration between the contents, ensuring the inseparability of teaching, research and extension12. Therefore, active teaching and learning methodologies corroborate the profile required by the NCG for medical students.
When asked about specialization, almost all students had the intention to obtain a specialist title, although the vast majority has not yet decided on the area of specialization, while others have already chosen it even before starting medical school. These data were also described by Costa et al.14 who, when interviewing medical students about the influence of the new curricular model on their “professional trajectory”, found that it was like asking them whether or not there was any doubt about the specialty they were thinking about acquiring, rather than asking about their training as a generalist physician. To justify these findings, it is necessary to understand the view of medical students regarding the values prioritized during the training phase and the relationship between graduation and the beginning of professional practice.
Vocation remains the determining factor in choosing a medical career, in the same way as the desire to contribute to society is associated to working as a generalist, with half of them bringing reports of medical models within the family. Previous studies have highlighted the family values of young generalist physicians, such as: focus on studies, honesty, personal autonomy and altruism. Almost all young generalist physicians reported an altruistic family history, whether due to political engagement, religious or humanitarian convictions.15
In a way, the interviewed medical students demonstrated humanitarian values and a sociopolitical view of the professional career when they expressed their belief in the Guidelines that guide the SUS and the desire to contribute to society’s needs. For this reason, they want to become generalists after medical training. According to Matta et al.16, one must take into account the fact that it difficult to clearly define the difference between the SUS principles and guidelines. Apparently, it is a simple task, were it not for the difficulty displayed by lawmakers when formulating the constitutional text and the Organic Health Law. These difficulties are also found among students, teachers and, mainly, SUS users. Considering this possibility, it is understood that, when they claim to “believe in the SUS Guidelines”, there is a broader view of the principles and guidelines that guide the SUS and historically denote the popular struggle for the universal, egalitarian and comprehensive right to health.
The values prioritized during the undergraduate course are anchor points to understand the relationship between medical education and the decision regarding professional practice. However, previous studies have shown that medical students’ values can change during their training.17)-(18 Nevertheless, the present study data showed that the interest in specialization remained unchanged, being similar between students attending the first three years and the last three years of the course.
A fact that must be taken into account is the influence of educators in valuing, encouraging the training and the practice of general medicine. When students were asked about the contribution of educators in their choice of professional practice, they perceived that some professors were indifferent or valued the medical specialization to the detriment of general practice, demonstrating that the roots of the Flexnerian model are still very firm in current medicine. The influence of the traditional teaching method, centered on the teacher and the contents, is still strongly verified in the daily lives of those who propose to be educators in the health area. The technicist thinking also persists, with a mechanistic pedagogical practice, controlled and directed by the teacher. In this concept, the teacher is a mere specialist in the application of manuals, which goes against the fragmented, biologist and super-specialized care model, making professional training disconnected from the social and political context14. Therefore, medical schools, as a matter of urgency, need to be updated regarding their structure and their teachers, with the latter being mostly physicians trained at institutions using the traditional model. According to Sá15, teachers are seen as professional models. Knowing who the role model is for the student helps to understand the values favored by the professional in training. A pedagogically qualified faculty is required to open up possibilities and expand reflections, in addition to serving as an example with an ethical, critical and reflective posture.
Data suggested by Meireles et al.19, when questioning students from an institution in the state of Minas Gerais using the PBL method, revealed that the course was more humanized and that some disciplines had been introduced, as well as the fact that they were receptive to discussion about cultural diversities in Brazil. However, they complained about the need for structural improvements, about teachers without didactics and the extensive workload.
Another fact revealed in our study was that, although most respondents belong to a private institution and study with their own resources, belonging to a public school influenced the decision to work as a generalist. Considering that the individuals with less financial resources are found in the public universities, according to Maheux and Béland20, students from more modest social origins often seek more social and generalist careers. Traditional public universities are perhaps institutions with better social orientation in their approach to medical education and, thus, exert sociopolitical changes in the students’ attitudes, in the same way they differ in the structural model when compared to private institutions, especially the most recent ones. In 2015, a survey by the Federal Council of Medicine (CFM, Conselho Federal de Medicina)21 disclosed that half of the municipalities with medical schools do not have the structure to adequately train the professionals, which is translated by the insufficiency of public hospital beds, primary care teams and teaching hospitals in cities that have medical courses.22
One can see that, in the field of professional practice, the desire to work as a generalist persists among the medical students, but this decision is only temporary. To definitely work as a generalist, in the student’s view, is to go against the tide. As generalists, they consider the labor market to be scarcer, perceive themselves as having little social status, lack of credibility with their medical colleagues and society, and with lower remuneration when compared to specialists.
Furthermore, in our study, women were the majority of the students, which corroborates the growing feminization of the medical career, as shown by the most recent surveys of the study ‘Medical Demography in Brazil’. Also, being a woman did not influence the desire to be a generalist professional, which is in line with current data regarding the distribution according to gender of physicians with a title in general and specialists in each specialty, considering that among men, 62 .9% are specialists and among women, 59.5% have a specialist title. These data suggest that women have been building, over time, a professional identity similar to that of men, based on a more competitive behavior imposed by the current labor market. Therefore, the specialization has become an imposed condition to enter the labor market and to result in greater service qualification, with better employment relationships and better remuneration.23
Added to this, the labor market does not facilitate the improvement of health in Brazil, as they favor specialists, who are concentrated in the private sectors and in large urban centers, while generalists and beginners tend to occupy jobs in the geographical areas with the highest health needs (and most of the time, of other sectors as well) and in public sectors. It is known that generalist physicians work in Primary Care, which is not synonymous with working only in the family health unit, as they can also occupy positions in emergency care units and outpatient clinics. However, the BHU is usually the workplace where they will be found in greater numbers, as it does not require specialization from the physicians and is not attractive to most specialists, unlike those who have recently graduated and want to be employed as soon as possible.
However, we must also take into account the perception of students in relation to the national scenario of the Brazilian public health system, the main place where newly graduated doctors work, regarding the management of health work. The Career, Position and Salary Plan (PCCS, Plano de Carreira, Cargos e Salários) can be defined as a work management tool that aims to implement the career process in the institutions. The implementation of a PCCS does not only mean gains in terms of remuneration. It can be a powerful instrument for improving working conditions, professional training and, more than that, for worker’s value. In this context, when asked about the lack of PCCS in the public health sector, it is understood that it is perceived by students as an instrument of professional valorization24. Thus, when most of them state that there is a lack of adequate PCCS in the public health sector, it is understood that, from the students’ point of view, the generalist is not valued by their managers either.
The generalist’s lack of credibility is another fact considered relevant for professional specialization, according to the interviewees. For them, society does not understand the role of the generalist, as the majority also believe that society does not trust the generalist’s role. They state, in their entirety, that the search for a generalist physician only occurs when a specialist is not available. This belief is due to the sociocultural view that non-specialized physicians have little knowledge, in which the well-trained generalist is not seen as someone who has undergone special training or acquired competencies and skills in exercise, capable of developing critical thinking and solving problems, even though medical school has the highest workload, with its six long years of duration, of which two include 100% practice in all main areas. On the other hand, when students are asked about their competencies and skills, they believe they are able to solve the main health problems when they graduate but perceive medical residency as an important complement to their training.
Remuneration was in the background as a type of encouragement for generalist physicians, although most of them perceive the specialist as being better paid, data also observed in the study by Antônio et al.2. These findings can be explained by the lack of immediate economic concerns among most students, who would still be under the protection of their families, with a favorable socioeconomic standard8, since most respondents study in a private institution, do not have a paid job and Medicine is their first degree; additionally, only a small portion depends on student funding and this fact did not influence the choice of working as a generalist. These data also justify the small number of participants who chose remuneration as the main motivation to start the medical course and improving the remuneration would not change the choice of working as a generalist physician.
An economic transition is seen in the job market for physicians, according to França25, who have become salaried professionals, dependent on the guidelines of health insurance plans and work teams. This economic hierarchy has not changed their moral and legal responsibilities regarding medical conduct; however, it has put some distance between patients and physicians. The doctor who was the family’s friend, who accompanied people since birth, starts to be seen as a service provider without emotional interaction with the patient, and the latter becomes a client, a situation that routinely causes conflicts.
Thus, we can say that the main motivation for seeking specialization is professional accomplishment, associated to acquired credibility and social prestige. Therefore, we can conclude that working at the gateway to the health system is still seen as a type of temporary work. The desire for specialization prevails, and even at a very early stage, which demonstrates a divergence between agreeing with government changes, realizing their influence on professional training and the personal decisions of each student. Much still needs to be done to change this scenario, starting with the consolidation and valorization of expanded, humanist and generalist medical training, with the creation of practical training scenarios that train critical-reflective individuals. Also, pedagogical methodological changes, which have already been suggested, should be established in favor of building critical medical thinking in decision-making, especially when the student begins to work in the field, that is, since the first years of the course. Also, science and research must walk in parallel with medical practice, without neglecting individualized and community care, while it is essential to train medical educators regarding teaching-learning innovations and curricular organization. It is necessary that, together with all this, the promotion of competencies and skills to deal with real problems and formulate original and creative actions capable of transforming social reality be carried out.
What is wanted is to develop a generalist medical practice in which the physician shares their knowledge with their patient, making the latter an active subject in their treatment process with decision-making. Although this attitude does not seem to have the same socioeconomic credibility that other specialties do, it confirms the urgent need to change the educational institutions, due to the importance of their role for those who already bring with them strong solidarity values and are focused on reducing inequities and facing social determinants and to open new possibilities for those who do not have the characteristics identified as relevant in primary socialization.
However, far beyond the need to consolidate changes in the curricular bases of the institutions and faculty, it is essential to change the cultural paradigm of society and even of the medical class itself, so that it is possible to implement the practice of Medicine in Primary Care. Social transformation is inherent to the generalist medical practice, so that it can be appreciated and recognized as having the competencies and skills to solve most problems in health care.
CONCLUSION
The students realize that the curriculum includes the generalist training; however, it did not influence their interest in professional practice. The desire to work as a generalist is found in a significant number of the students, driven by altruism and the desire to contribute to society, supported by the Organic Laws that underlie the SUS Guidelines and Principles, whereas not feeling valued and having their credibility questioned by society, encourage their professional practice as generalists as a temporary activity.

