










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por emailCompartilhar

 Permalink
PermalinkRevista Brasileira de Educação Médica
versão impressa ISSN 0100-5502versão On-line ISSN 1981-5271
Rev. Bras. Educ. Med. vol.46 no.3 Rio de Janeiro 2022 Epub 29-Ago-2022
https://doi.org/10.1590/1981-5271v46.3-20210471
ORIGINAL ARTICLE
Adherence of the Medical Course PPCs to the parameters of the Brazilian medical education policy

1Universidade Federal de Goiás, Goiânia, Goiás, Brazil.
2Nova School of Business and Economics, Lisbon, Portugal.
Introduction:
Recent studies have been dedicated to analyzing the PPCs of the medical course and their degree of alignment with what is determined by the Brazilian legislation for the opening and operation of the course in the country. However, there are no nationwide studies that have investigated whether the pedagogical projects for the medical courses are in compliance with current Brazilian legislation.
Objective:
In this study, we analyzed the adherence of the Pedagogical Course Projects (PPCs) of medical schools in Brazil based on the National Curriculum Guidelines (DCNs, Diretrizes Curriculares Nacionais) of medical education and the “Mais Médicos” Program (PMM, Programa Mais Médicos) for Brazil.
Method:
To achieve this objective, we collected 157 PPCs from medical courses in Brazil and categorized them in a Likert Scale of adherence, ranging from non-adherent (1) to strongly adherent (5), based on three dimensions of analysis: guiding aspects of training, curricular aspects, teaching-service aspects. Subsequently, using the Principal Component Analysis, we created the PPC Adherence Synthetic Index. After the database was created, descriptive statistics and relational graphs were applied to describe the situation in Brazil.
Results:
The results show that: I) the Midwest region is the one with the best performance in the three analyzed dimensions; II) public institutions (39% of the total) have greater adherence of PPCs to the analyzed normative parameters; and III) the teaching-service dimension shows greater variation between the types of institution administration, with less adherence by private institutions.
Conclusions:
Therefore, ultimately, this study raises an alert regarding the adequacy of medical courses in private institutions to the normative and legal parameters required for medical training in Brazil. In addition, it contributes to the literature by presenting an evaluation model for pedagogical course projects through the Synthetic Index of Adherence of PPCs as a suggestion for future studies.
Keywords: Health Education; Educational Assessment; Medicine; Medical Education
Introdução:
Pesquisas recentes têm se dedicado a analisar os projetos pedagógicos dos cursos (PPC) de Medicina e o grau de alinhamento deles ao que determina a legislação brasileira para abertura e funcionamento dos cursos no país. No entanto, não há estudos de abrangência nacional que tenham investigado se os PPC de Medicina estão em conformidade com a legislação brasileira vigente.
Objetivo:
Neste estudo, buscou-se analisar a aderência dos PPC de Medicina no Brasil às Diretrizes Curriculares Nacionais (DCN) do ensino médico e ao Programa Mais Médicos para o Brasil (PMM).
Método:
Para alcançar esse objetivo, coletaram-se 157 PPC de Medicina no Brasil que foram categorizados em uma escala Likert de aderência, que varia de não aderente (1) a fortemente aderente (5), a partir de três dimensões de análise: aspectos norteadores de formação, aspectos curriculares, aspectos ensino-serviço. Posteriormente, por meio da análise de componentes principais, criou-se o Índice Sintético de Aderência dos PPC. Com o banco de dados criado, aplicaram-se estatísticas descritivas e gráficos relacionais para descrever a situação no Brasil.
Resultado:
Os resultados demonstram o seguinte: 1. a Região Centro-Oeste obteve a melhor performance nas três dimensões analisadas; 2. as instituições públicas (39% do total) têm maior aderência dos PPC aos parâmetros normativos analisados; e 3. a dimensão ensino-serviço aponta maior variação entre os tipos de administração das instituições, com menor aderência das instituições privadas.
Conclusão:
Este trabalho acende um alerta em relação à adequação dos cursos de Medicina das instituições privadas aos parâmetros normativos e legais exigidos para a formação médica no Brasil. Além disso, contribui para a literatura ao apresentar um modelo de avaliação de PPC por meio do Índice Sintético de Aderência dos PPC como sugestão para trabalhos futuros.
Palavras-chave: Educação em Saúde; Avaliação Educacional; Medicina; Educação Médica
INTRODUCTION
In Brazil, the medical course is regulated by the Mais Médicos Program law (2013) and by the National Curriculum Guidelines (DCNs, Diretrizes Curriculares Nacionais) of 2001, later updated in 2014. These regulations show the importance of some elements discussed at the first World Conference of Medical Education in Edinburgh, in 1988, about the need for a radical change in medical education so it could accompany changes at a global level, including health care models.
Deep discussions and adjustments characterized the curriculum development of medical courses in Brazil, especially in this century1. The National Curriculum Guidelines (DCNs, Diretrizes Curriculares Nacionais) of 2001 were an important milestone in the reorientation of professional training2. The DCNs were constructed based on organized society, organizations representing physicians and educators, popular pressure and the National Health Council, and supported changes in the medical curriculum towards a graduate with a more generalist profile. Another important milestone was the review and publication of the new medical course DCNs in 2014, which highlighted Primary Health Care (PHC) in the training of medical professionals, as well as the need for a more generalist orientation in medical education in the Brazil3.
The ‘More Doctors Program’ for Brazil (PMM, Programa Mais Médicos) started with the decision to deal with the problem arising from the insufficient number and unequal distribution of physicians in the country, which has worsened over the years with the expansion of the Brazilian Unified Health System (SUS, Sistema Único de Saúde) and supplemental health services. In 2011, the federal government defined the problem of the deficit in the provision of health professionals as a necessary and priority confrontation to guarantee the population’s access to good quality health services3. Among the government’s first actions to face this challenge, the Program for Valuing Primary Care Professionals (PROVAB, Programa de Valorização dos Profissionais da Atenção Básica) was launched by the Ministry of Health, with the objective of qualifying the training of medical school graduates, as a way of valuing the teams that work in PHC and, at the same time, motivate and attract physicians to work in areas with greater need. Therefore, it was expected that PROVAB would contribute to the continuity of learning after medical graduation4, which should have been carried out in accordance with the DCNs of the medical course5.
Although it contributes to provide doctors for Primary Care, initiatives such as PROVAB in 2011 were not enough to meet the population’s growing demand. Additionally, due to the fact that the demand was not adequately met, the More Doctors Program (PMM) in Brazil was created, regulated by Law N. 12,871/20136. The PMM was structured to act on three axes: allocation of doctors in regions where there is a shortage or lack of these professionals (emergency provision axis); investments for the construction, renovation and expansion of Basic Health Units (infrastructure axis); and creation of new undergraduate and medical residency vacancies for the training and qualification of these professionals (education axis)7. Regarding the latter, the PMM determined significant changes towards the reorientation of medical training, which resulted in the creation and publication of new DCNs for the medical course.
Studies have shown the importance of acquiring knowledge consistent with the context and health needs of the population, both for maintaining medical professionals in Primary Care and for medical training5),(8. In this sense, with the implementation of the new DCNs, educational institutions had to adapt the pedagogical projects of the medical course, aiming to reflect the necessary changes in the training of new professionals, thus allowing them to be trained for the challenges that their practice requires. Such changes range from the creation of mechanisms by educational institutions to benefit from the knowledge acquired by the student to the promotion of the participation of the Health Network professionals in a permanent training and development program, aiming to improve the teaching-learning process in SUS practice environments and the quality of care provided to the population3.
Recent studies have dedicated to analyzing the PPCs of the medical course and their degree of alignment to what is determined by the Brazilian legislation for the opening and operation of medical courses in the country 9), (10. The researchers and public managers’ attention in the area is focused on trying to understand the real needs of medical training in Brazil and how institutions are following the legal and regulatory requirements, as well as the efforts of the Ministries of Health and Education 11),(12.
Nonetheless, there are no national studies that have investigated whether pedagogical projects in medical courses are in compliance with current Brazilian legislation. It is also observed that this topic is rarely addressed in the field of research involving curricula and medical training13. Based on this picture, the following question can be raised: to what extent are the PPCs of medical courses in Brazil in compliance with the current legislation? To answer this question, the general objective of this study was to analyze the adherence of the PPCs of the medical courses in Brazil to the National Curriculum Guidelines (DCNs) of medical education and to the guidelines of the More Doctors Program (PMM) in Brazil. As specific objectives, we proposed creating an index of compliance of the PPCs of Brazilian medical courses regarding the legislation and training guidelines currently in force, and to identify the main differences in the compliance of medical courses by Brazilian macro-regions and type of institutions.
MATERIALS AND METHODS
To achieve the objective of this research, an analytical-descriptive study was carried out based on collected secondary material. As proposed in the studies by Bardin14, Triviños15 and Minayo16, the documental analysis can be carried out in three stages:
pre-analysis - in which the choice is made of which documents should be collected, the organization of the material and its reading. In this phase, the following were collected: Ministry of Education (MEC) Ordinances; DCNs of the medical course; the More Doctors Program regulations in Brazil; PPCs of medical courses in Brazil; Documents and publications on the official websites of the Ministry of Health (MOH) and Ministry of Education. After the collection, the data were organized by the researchers in an Excel spreadsheet.
analytical description and evaluation of the material - at this stage, the researchers defined the classification, coding and categorization of the data. The categorization of the normative material comprised: 1) General information (information on the region, state, institution profile, workload, etc.) and; 2) Three dimensions of analysis:
Guiding aspects of training (principles and values established in the National Curriculum Guidelines of the course)
Curricular aspects (criteria established by the National Curricular Guidelines of the course for the creation of the PPC curricular matrix)
Teaching-Service Aspects (these are criteria established by the More Doctors Program regulation in Brazil that must constitute the PPCs of the course).
Data processing and interpretation - at this stage, the material is analyzed in depth, which increases knowledge about the study object and the necessary judgments are applied in order to describe the processed data. The careful analysis of the PPCs was based on the assumption of the judgement of the items through a Likert Scale, consisting of five points, with an increasing, ordinal, two-dimensional disposition - non-adherent to strongly adherent - and without the option of using the neutral point, since the study objective requires a judgment decision, as recommended by the literature 17-19. Thus, these were the scale points: 1. Non-adherent; 2. Weakly adherent; 3. Regular adherence; 4. Moderately adherent; 5. Strongly adherent. The explanation for each point is described below:
Non-adherent: It means that the PPC does not have information about the item.
Weakly adherent: It means that the PPC has information that is cited, without description or detailing of actions.
Regular adherence: It means that the PPC has information that is cited, with a description, but without information on the action.
Moderately adherent: It means that the PPC has information that is cited, with a description, but with insufficient information to understand the action.
Strongly adherent: It means that the PPC has information that is cited, with a description and sufficient information to understand the action.
The search for PPCs started on the official websites of the 280 institutions that offer the medical course in Brazil, considering that in some institutions the course is offered on more than one campus, resulting in 339 fully operational medical courses 20. Of the 339 active courses, only 148 PPCs were available for download from their respective official websites. The second search took place by telephone and e-mail. Nine institutions sent the documents, thus totaling 157 collected PPCs.
All PPCs were stored in a shared folder to which the researchers had access. The reading and categorization of normative documents were organized in an Excel spreadsheet. The choice of categories was due to the content of the documental analysis of the Pedagogical Course Projects (PPCs) of medical schools to the detriment of what determines the normative part of the course: the PMM law and the DCNs of 2001 and 2014.
The study was carried out from September to December 2020. For the judgements to be as standardized as possible, the researchers underwent a pilot training two weeks before the analysis of the PPCs. Additionally, the team worked together, so that every time there was doubt in the interpretation of a document, the entire team analyzed the PPCs, aiming to reach a consensus on the judgment.
After the database was built, it was time to think about creating the three dimensions: Guiding Aspects of Training - (ANF, Aspectos Norteadores de Formação) comprising the DCNs; Curricular Aspects (AC, Aspectos Curriculares) comprising the DCNs; and Teaching-Service Aspects - (AES, Aspectos Ensino-Serviço) comprising the PMM articles. Table 1 shows in detail the construction process of the three dimensions adopted in the present study.
Table 1 Dimensions, indicators and normative basis.
| Dimensions | Indicators | Normative basis |
|---|---|---|
| Guiding Aspects of Training (ANF) | Profile of the graduate/professional; Competencies and skills; General Competencies; Specific Knowledge, Competencies and Skills. | • DCNs 2001 (Resolution CNE/CES N. 4, of November 7, 2001). • DCNs 2014 (Resolution CNE/CES N. 3, of June 20, 2014). |
| Curricular Aspects (AC) | Curricular Contents; Course Organization; Internships and Complementary Activities; Monitoring and Evaluation. | |
| Teaching-Service Aspects (AES) | Structure and competences of the institution regarding the teaching-service practice. | • More Doctors Program regulation n. 12.871, of October 22, 2013. • More Doctors Program for Brazil MP/890, of 2019. |
Source: prepared by the authors, 2021.
To create the three dimensions and aiming at not assigning different weights to the indicators, the Mean Central Tendency measure21 was used, applied to the indicators that comprise each of the dimensions, as shown below:
After the creation of the three dimensions (ANF, AC and AES), the Synthetic Index of Adherence of the PPCs (Medicine Case), ISAPPC-MED, was created. For its creation, we used the same previous approach of the dimensions, the Mean Central Tendency measure 21:
Thus, with the implementation of the three dimensions and the synthetic index, the final database for the analysis was established: general information, ANF, AC, AES and ISAPPC-MED.
The quantitative analysis of the data was divided into 4 stages. Initially, the number of PPCs collected by type of location (website or e-mail) and by type of administration of the institution (private, federal, state or municipal) was analyzed. Subsequently, the second stage sought to evaluate the performance of institutions in the three dimensions and in the synthetic index by dividing them into types of administration and macro-regions. During this process, descriptive statistics, mean and standard deviation were used, as well as the separation by quartiles 21),(22.
Subsequently, aiming to observe a possible relationship with the course workload or their longevity with performance, the mean descriptive statistics were used, with the division again by quartiles22. Finally, in the last stage, hierarchical cluster analysis was applied to all observations in the sample using the three dimensions created 21),(22. When the clusters are created, the analyses can be carried out regarding the macro-regions in which they are located.
In all the above mentioned stages, the results were presented graphically and in a simplified way, aiming at making the analysis understandable and easily replicable.
RESULTS AND DISCUSSION
In this section, the research data are presented and discussed, according to the perspective of the analytical proposal discussed in the method.
Aspects of collection
Graph 1 shows the degree of adherence of institutions to MEC Ordinance Number 23 of 2017, Art. 99, item 1, which establishes the obligation for the institution to maintain on its own website and at the academic secretariat, for consultation by students or interested parties, the duly updated official record of information on the courses offered, including the PPC. Of the 339 active medical courses on the eMEC portal, only 148 PPCs were available for download on the official websites of their respective institutions. There was a second search for contact by telephone and email, with the return of 9 PPCs provided by the institutions, which totaled 157 collected PPCs.
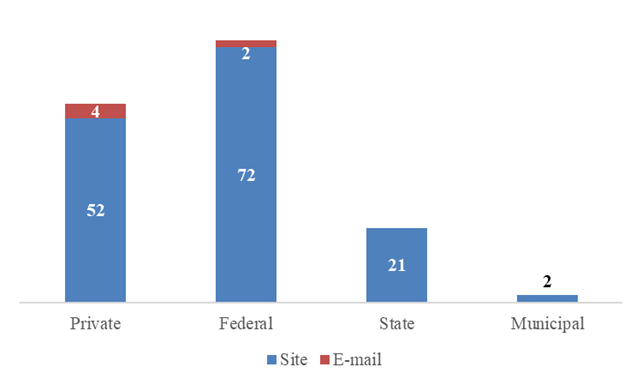
Considering the performed search, only 46% of the institutions that offer the medical course comply with MEC Ordinance number 23 of 2017, Art. 99, item 1, by making available on their official websites or providing the PPC of the course through their secretariats. Of this percentage, the majority that comply with the legal system are federal public educational institutions. This finding shows the importance of studies focused on analyzing the adherence of educational institutions to the Brazilian normative basis.
Considering that today, of the 339 active medical courses20, 134 are offered in public institutions (representing 39%) and yet, as shown in Graph 1, most courses that have PPC accessible to students and interested parties belong to public educational institutions, we can deduce that: despite being a minority regarding the offer of medical courses, public institutions show greater adherence to the availability of PPCs on their official websites and secretariats.
National performance, by type of institution and by macro-regions.
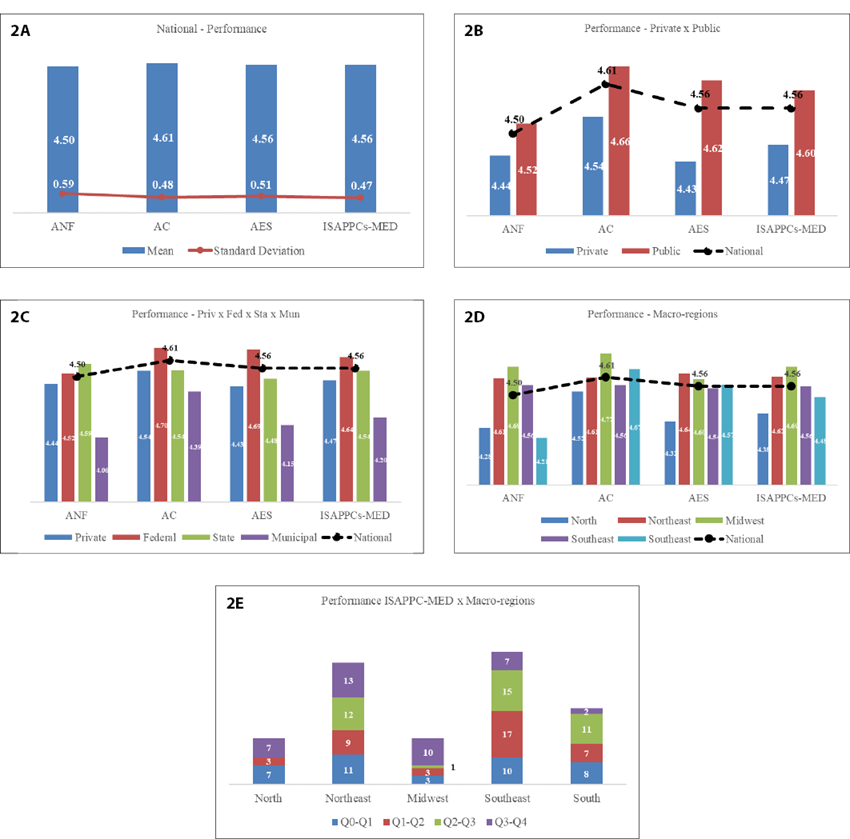
Graph 2A shows that there are no major variations in the national perspective, with a higher standard deviation value in the ANF and AES dimensions. Therefore, it is understood that the Curricular Aspects are mostly adherent to the DCNs and PMM. In relation to the ISAPPC-MED synthetic index, the AC dimension obtained the highest result, showing to be above average in relation to the others.
Source: Prepared by the authors, 2021.
Graph 2 National performance by type of institution and by macro-regions.
Graph 2B depicts a greater variation between the three dimensions. The performance in the three dimensions ANF, AC, AES and also in the synthetic index (ISAPPC-MED) shows to be higher in public institutions. Although there are more private institutions offering the medical course (61% of the institutions), public institutions show greater adherence of their PPCs to the current legislation. It is noteworthy that the AES dimension was the one that showed the greatest variation between the types of administration of the institutions.
Rezende et al.10 shows, in their qualitative study, that the lack of support from municipal management, lack of internship areas and qualified instructors are among the main obstacles for the institution to adhere to what the PMM establishes on the teaching-service practice in the institutions. Another complicating point observed in the literature is the lack of teachers with specific training in the area 9),(10. It is necessary to analyze, in future studies, the reality of private institutions in relation to the lower adherence of PPCs regarding this dimension.
Graph 2C shows that there is a variation between the three dimensions regarding the type of administration (Private, Federal public, State public, Municipal public), showing that PPCs of federal institutions tend to have a better performance. On the other hand, the ISAPPC-MED synthetic index indicates that municipal public institutions show less adherence in relation to other types of administration. This finding is in contrast with the result of the study by Oliveira et al.23, which compared the PPCs of medical courses in public institutions at the municipal and federal levels, showing that there were no differences between them. Because this study has a national scope, innovation of data is observed, as well as relevant information for future studies.
Cyrino et al.11 indicate in their study that the legislation flexibilization regarding the construction of medical training models consistent with local characteristics and the requirements of the Brazilian Unified Health System (SUS) concerning its role of organizing the training of health professionals can contribute to the reduction of health inequalities.
Graph 2D shows the performance of the macro-regions regarding the three analyzed dimensions and the synthetic index. Institutions in the Midwest region stand out for being the ones with the highest rate of adherence to current legislation, while the northern region is where the institutions have the lowest adherence. In the analysis by dimensions, the Northeast region stands out where institutions have greater adherence in relation to the Teaching-Service aspect. Considering previous studies, which showed that institutions have some difficulty to fully adhere to the structure and competence aspect regarding the teaching-service practice11,23, this is an important finding for future studies.
In relation to the performance of the ISAPPC-MED synthetic index regarding the macro-regions structured by quartiles, Graph 2E shows that in the Southeast and Northeast macro-regions there is a higher number of institutions with average adherence between the dimensions constituted by the index. The graph also shows that the Midwest macro-region is where the institutions have a lower average adherence.
Performance by workload and by year of course accreditation
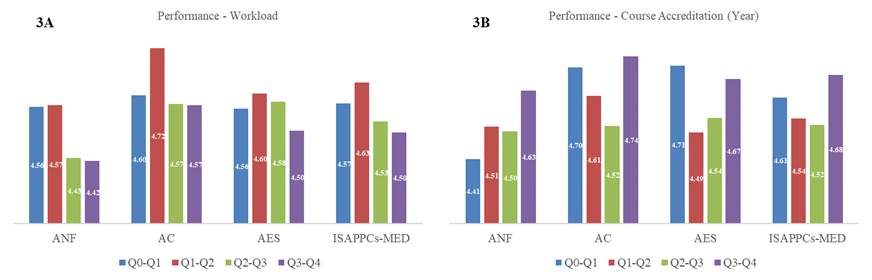
Graph 3A shows through quartiles (Q0-Q1; Q1-Q2; Q2-Q3; Q3-Q4) separated by workload, from the lowest to the highest in terms of adherence to the PPCs, relative to the ANF, AC, AES dimensions and by the ISAPPC-MED index. The results show that courses with less workload tend to have higher performance.
Graph 3B depicts the quartiles (Q0-Q1; Q1-Q2; Q2-Q3; Q3-Q4) separated by year of course accreditation at the institutions, organized from the lowest to highest. The results show that there is no tendency for newer or older courses to have higher or lower performance, that is, the year of course accreditation does not influence the adherence of PPCs to the current legislation.
Performance of clusters
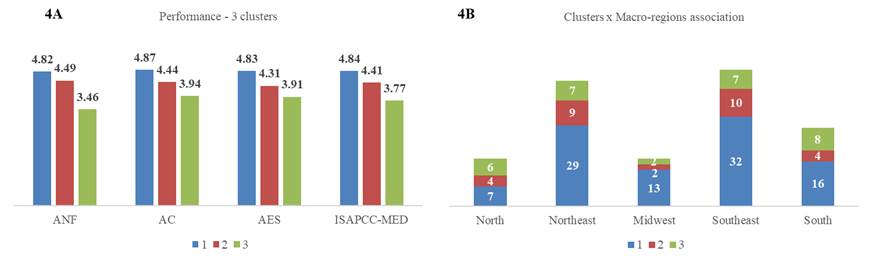
As shown in Graph 4A, cluster 1 consists of the medical courses with the highest performance in all dimensions and in the ISAPPC-MED, while cluster 2 consists of the courses with average performance, and finally, cluster 3 consists of the courses with the lowest performance.
Finally, Graph 4B shows the relationship between the clusters and their division by the Brazilian macro-regions. In this analysis, it is clear that almost all macro-regions have, for the most part, more high-performance courses, with the exception of the North macro-region. In addition, the Northeast and Southeast macro-regions have a number of courses with similar performance in their divisions in the clusters, while the Midwest macro-region stands out, with 76.5% of its courses showing high performance.
FINAL CONSIDERATIONS
This study aimed to analyze the PPCs of the medical course in Brazil to measure the degree of adherence to what is determined by the National Curriculum Guidelines (DCNs) of medical education and the Mais Médicos Program (PMM) for Brazil. Based on the synthetic index created for this purpose, it was possible to identify that the macro-region that showed the highest performance regarding the adherence to PPCs, according to the current legislation, was the Midwest macro-region.
The results showed that despite being a minority in the offer of the medical courses (39% are public institutions), public institutions are the majority regarding the adherence of PPCs to the current legislation. Of the three analyzed dimensions, the one that shows the greatest variation between the type of administration of the institutions is the teaching-service aspect, with lower adherence regarding the PPCs of private institutions.
The results obtained in this study can support the reformulation of policies and norms that guide medical training in Brazil. Based on these results, a decision-making seems necessary by the managers in the areas of regulation and supervision regarding what is required of educational institutions. Moreover, one may ask: are the aspects provided for in the legislation, in fact, relevant to medical training in Brazil? If yes, why do institutions not comply with public policies that guide medical education?
The study was limited to quantitatively analyzing the PPCs of the medical courses regarding the adherence of the PPCs to what is required by current legislation. Another limitation in the present study was the choice of studying only PPCs from the medical courses, and this study could be reproduced in other courses in the health area.
As a way of contributing to the literature on the topic, the evaluation model of pedagogical course projects through the Synthetic Adherence Index of PPCs is proposed as a proposal for future studies. We also suggest the in-depth study of the Teaching-Service aspect, as it is pointed out by the literature that there is some difficulty for the institutions to fully comply with the structure and competence aspect regarding its practice. Additionally, one should analyze whether the current legislation meets the actual local needs for medical training in Brazil.
REFERENCES
1. Bollela V, German IA, Campos H, Amaral E. Síntese final e as perspectivas para o futuro da educação baseada na comunidade no contexto brasileiro. In: Bollela VR, Germani ACC, Campos HH, Amaral E, organizadores. Educação baseada na comunidade para as profissões da saúde: aprendendo com a experiênc. Ribeirão Preto: Funpec; 2014. p. 293-7. [ Links ]
2. Brasil. Diretrizes Curriculares Nacionais dos Cursos de Graduação em Enfermagem, Medicina e Nutrição. Diário Oficial da União; 2001. Disponível em: http://portal.mec.gov.br/dmdocuments/ces1133.pdf. [ Links ]
3. Brasil. Resolução CNE/CES nº 3/2014. Institui Diretrizes Curriculares Nacionais do Curso de Graduação em Medicina e dá outras providências. Diário Oficial da União ; 2014. p. 203. [ Links ]
4. Carvalho MS. Programa de Valorização dos Profissionais da Atenção Básica: um olhar implicado sobre sua implantação [dissertação]. Brasília: Universidade de Brasília; 2013 [acesso em out/2021]. Disponível em: Disponível em: http://repositorio.unb.br/handle/10482/13660 . [ Links ]
5. Vasconcelos RNC, Ruiz EM. Formação de médicos para o SUS: a integração ensino e saúde da família - revisão integrativa. Rev Bras Educ Med. 2015;39(4):630-8. [ Links ]
6. Brasil. Lei no 12.871, de 22 de outubro de 2013. Institui o Programa Mais Médicos, altera as Leis no 8.745, de 9 de dezembro de 1993, e no 6.932, de 7 de julho de 1981, e dá outras providências. Brasília; 2013. [ Links ]
7. Girardi SN, Van Stralen AC de S, Cella JN, Der Maas LW, Carvalho CL, Faria E de O. Impacto do Programa Mais Médicos na redução da escassez de médicos em atenção primária à saúde. Ciênc Saúde Colet. 2016;21(9):2675-84. [ Links ]
8. Cortez LR, Guerra EC, Da Silveira NJD, Noro LRA. The retention of physicians to primary health care in Brazil: motivation and limitations from a qualitative perspective. BMC Health Serv Res. 2019 Jan 22;19(1). [ Links ]
9. Oliveira CA de, Senger MH, Ezequiel O da S, Amaral E. Alinhamento de diferentes projetos pedagógicos de cursos de Medicina com as Diretrizes Curriculares Nacionais. Rev Bras Educ Med . 2019;43(2):143-51. doi: http://dx.doi.org/10.1590/1981-52712015v43n2RB20180203. [ Links ]
10. Rezende VLM, Rocha BS, Naghettini A, Fernandes MR, Pereira ERS. Percepção discente e docente sobre o desenvolvimento curricular na atenção primária após Diretrizes Curriculares de 2014. Rev Bras Educ Med . 2019;43(3):91-9. doi: https://doi.org/10.1590/1981-52712015v43n2RB20180237 [ Links ]
11. Cyrino EG, de Sordi MRL, Mendes G do SCV, Luna WF, Mendonça CS, Alexandre FLF, et al. Mapeamento das características da implantação de novos cursos de Medicina em universidades federais brasileiras. Rev Panam Salud Publica. 2020;44:67. [ Links ]
12. De Sousa-Muñoz RL. Currículo médico e o novo projeto político-pedagógico. Rev Espaço do Currículo. 2011;3(2):601-8 [acesso em 2 mar 2021]. Disponível em: Disponível em: http://periodicos.ufpb.br/ojs2/index.php/rec . [ Links ]
13. Silva MP, Paraíso MA. Um currículo na integração ensino-serviço do Programa Mais Médicos e possíveis efeitos culturais. Trab Educ Saúde. 2019;17(3). [ Links ]
14. Bardin L. Análise de conteúdo. 3a ed. Lisboa: Edições 70; 2004 [acesso em out/2021]. Disponível em: Disponível em: https://www.scielo.br/scielo.php?script=sci_nlinks&ref=000125&pid=S0103-5150201200010000500004&lng=en . [ Links ]
15. Triviños A. Introdução à pesquisa em ciências sociais: a pesquisa qualitativa em educação. São Paulo: Atlas; 1987. [ Links ]
16. Minayo MC de S. O desafio do conhecimento: pesquisa qualitativa em saúde. 9ª ed. São Paulo: Hucitec; 2006. 406 p. [ Links ]
17. Weathers D, Sharma S, Niedrich RW. The impact of the number of scale points, dispositional factors, and the status quo decision heuristic on scale reliability and response accuracy. J Bus Res. 2005;58(11 spec):1516-24. [ Links ]
18. Viswanathan M, Sudman S, Johnson M. Maximum versus meaningful discrimination in scale response: implications for validity of measurement of consumer perceptions about products. J Bus Res . 2004;57(2):108-24. [ Links ]
19. Collings DP. Selecting a questionnaire response scale for student feedback surveys: a comparison of psychometric properties and student preferences among three alternatives [dissertation]. Perth, Australia: Murdoch University; 2006. [ Links ]
20. Brasil. Portal e-MEC. 2021 [acesso em jul/2021]. Disponível emDisponível em:: https://emec.mec.gov.br/ . [ Links ]
21. Hair Júnior JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. 7th ed. Pearson Prentice Hall, Hoboken, Nova Jersey; 2009. 761 p. [ Links ]
22. Fávero LP, Belfiore P. Manual de análise de dados. Elsevier, São Paulo, SP; 2017. 1219 p. [acesso em jul/2021]. Disponível em: Disponível em: http://dergipark.gov.tr/cumusosbil/issue/4345/59412 . [ Links ]
23. Oliveira NMF, Barreto B, Furlaneto IP, Borges Neto F das C. Conhecimento de alunos de Medicina do Centro Universitário do Estado do Pará sobre a residência médica. Rev Bras Educ Med . 2019;43(1):32-8. [ Links ]
Received: November 23, 2021; Accepted: March 29, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
