










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format
 Send this article by e-mail
Send this article by e-mailShare

 Permalink
PermalinkRevista Brasileira de Educação Médica
Print version ISSN 0100-5502On-line version ISSN 1981-5271
Rev. Bras. Educ. Med. vol.46 no.3 Rio de Janeiro 2022 Epub Oct 10, 2022
https://doi.org/10.1590/1981-5271v46.3-20220106
ORIGINAL ARTICLE
Distribution of adult semiology in medical schools in Brazil
1
, project design, collection and analysis of data, writing and review of the manuscript http://orcid.org/0000-0001-7706-6380
http://orcid.org/0000-0001-7706-6380
1
, project design, collection and analysis of data, writing of the manuscripthttp://orcid.org/0000-0003-3866-995X
1
, project design, collection and analysis of data, writing of the manuscripthttp://orcid.org/0000-0002-2982-0470
1
, research orientation as advisor to Eliane Teixeira Alfama Moniz, project design, collection and analysis of data, writing and review of the manuscripthttp://orcid.org/0000-0002-2039-9827
1Universidade Federal de Santa Catarina, Santa Catarina, Florianópolis, Brazil.
Introduction:
Semiology is the basis of clinical practice and its teaching is essential in the medical course. This study was developed to fill a gap in the knowledge about its distribution in Brazil.
Method:
Cross-sectional descriptive study with 226 Brazilian medical schools that provided the distribution of semiology on the Internet among the 335 active schools in December 2020 (67.5%) The variables studied were school geographic region, administration and free tuition, time of existence of the course, course load of the regular course, clerkship and semiology, and year(s) or semester(s) in which semiology was offered in the curriculum. Data analysis was descriptive and the associations were analyzed using: Student’s t, Chi-square, Analysis of Variance, Mann-Whitney-U, Kruskal Wallis and Wilcoxon tests. The significance level was set at p < 0.05.
Result:
Semiology was more frequently offered only in the 4th semester (n = 40), followed by its offer in two semesters, the 4th and 5th and 3rd and 4th. Among the 226 schools, 142 integrated semiology into modules or axes (62.8%). Among the 117 schools that provided the semiology course load, its median was 240.0 hours (P25-75 = 165.4 - 338.2), with no statistical difference by geographic region, type of administration and time of existence of the course. The median of the theoretical course load [77.5 hours (P25-75 = 51.7 - 123.5)] was lower than the practical course load [147.0 hours (P25-75 = 64.5 - 180.0)], Z = - 3,99, p < 0,01. The median of the percentage of semiology course load during the course was 2.9% (P25-75 = 2.0 - 4.0).
Conclusion:
Semiology is more frequently offered in the 4th semester and its median course load is similar in Brazilian geographic regions and by school administration type and time of existence of the assessed schools.
Keywords: Semiology; Medical History Taking; Physical Examination; Curriculum; Medical Education
Introdução:
A semiologia é a base da prática clínica e seu ensino é essencial no curso de Medicina. Este estudo foi desenvolvido por haver uma lacuna no conhecimento sobre sua distribuição no Brasil.
Objetivo:
Este estudo teve como objetivo analisar a distribuição da semiologia do adulto nas escolas médicas brasileiras.
Método:
Trata-se de um estudo transversal descritivo realizado com 226 escolas médicas brasileiras que disponibilizavam a distribuição de semiologia na internet entre as 335 ativas, em dezembro de 2020 (67,5%). As variáveis estudadas foram região geográfica, administração, gratuidade e tempo de existência da escola, carga horária do curso, do internato e de semiologia, e ano(s) ou semestre(s) em que a semiologia era ofertada no currículo. A análise dos dados foi descritiva, e analisaram-se as associações com os testes: t de Student, análise de variância, qui-quadrado de Pearson, U de Mann-Whitney, Kruskal-Wallis e Wilcoxon. Admitiu-se um nível de significância de p < 0,05.
Resultado:
A semiologia foi mais frequentemente ofertada apenas no quarto semestre (n = 40), seguida por sua oferta em dois semestres: quarto e quinto e terceiro e quarto. Entre as 226 escolas, 142 integravam os conteúdos em módulos ou eixos (62,8%). Entre 117 escolas que forneciam a carga horária de semiologia, mediana foi de 240,0 horas (P25-75 = 165,4 - 338,2), sem diferença estatística por região geográfica, administração, gratuidade e tempo de existência da escola. A mediana da carga teórica de semiologia [77,5 horas (P25-75 = 51,7 - 123,5)] foi menor do que a carga prática [147,0 horas (P25-75 = 64,5 - 180,0)], Z = -3,99, p < 0,01. A mediana da porcentagem da carga horária de semiologia no curso foi de 2,9% (P25-75 = 2,0 - 4,0).
Conclusão:
A semiologia é mais frequentemente ofertada no quarto semestre, e sua carga horária não difere por características geográficas, de administração e tempo de existência das escolas estudadas.
Palavras-chave: Semiologia; Anamnese; Exame Físico; Currículo; Educação Médica
INTRODUCTION
Medical semiology is the foundation of clinical practice and, despite all advances in technology, the tripod consisting of the doctor-patient relationship, history and clinical evaluation will remain the essence of Medicine1. Therefore, its teaching is part of the first trainings of medical students towards their future practice2),(3.
The word semiology derives from the Greek words semeîon, which means sign, and logos, which means word, discourse, treatise4. In the health area, “sign” refers to something objective, verifiable and explicit, while “symptom” has a more subjective characteristic and depends on the process of illness and the disease expression in the person, which influence how they feel and interpret their suffering5. Semiology, therefore, comprises the evaluation of diseases in the individuals, through their signs and symptoms4. The word semiogenesis is defined as the knowledge of the forms of presentation of the disease signs and symptoms, while the word semiotechniques (i.e., physical examination techniques) is defined as the evaluation of the patient’s physical condition, which, associated with the investigation of signs and symptoms, allows the establishment of a syndromic diagnosis1. The word ‘propaedeutics’ derives from the Greek, propaideutikós, in which ‘pro’ means before and paidein means to teach, that is, preparatory study6.
According to Devine et al., the multiple denominations of semiology and its integration in the curricula make the assessment of its curricular workload challenging7. However, we found some comprehensive international studies on semiology in medical schools. A Cuban study compared the different components of the curriculum in the academic year 1985-1986 with those for the year 2010-20118, after a change in Cuba’s “study schedule” in 2010. In Colombia, a study reviewed information on semiology in the curriculum of five of the six schools in the city of Cali9. In the United States, the Association of American Medical Colleges provides data on the medical course disciplines per academic year10 and there is a study on the teaching of physical examination before clerkship in 106 medical schools of 141 medical schools (75%) accredited by the Liaison Committee on Medical Education in the academic year 2015 - 201611. Two studies carried out in Europe analyzed the curricula of medical schools. One of them assessed 32 medical schools from 18 European countries from 2001 to May 200212 and another assessed 16 medical schools from six southeastern European countries from March to July of 200313. Devine et al. conducted a study on teaching practices in 25 of 35 UK medical schools in the 2014-2015 academic year. However, the authors combined the contents of semiology and physical examination with internal medicine and general practice, not allowing the identification of specific data on semiology7.
In Brazil, we found one study on the teaching of semiology in 14 medical schools in Rio de Janeiro in 2006. At the time, Brazil had a total of 119 medical schools, with 57 of them located in the Southeast region, of which 15 were located in the state of Rio de Janeiro1. We also found a study carried out in Universidade Federal de Minas Gerais, which described the two semiology modules they offered and analyzed the perception of 157 third-year undergraduate medical students who had completed their training about semiology3. The study found that 56.1% of the students considered the workload to be insufficient, 54.1% considered that they knew how to collect the patient’s history, and 65% thought that, despite being able to perform the patient’s physical examination, they did not master the necessary skills to perform a more extensive physical examination3.
The National Curriculum Guidelines (DCN, Diretrizes Curriculares Nacionais) for the undergraduate medical course in Brazil address semiology in the key action of “identification of health needs” of its subsection I (“of attention to individual health needs”) and establish that, when carrying out the clinical history, the student must have an ethical relationship, favor the construction of the bond with the patient, consider the biopsychosocial and cultural aspects related to the health-disease process and organize and guide the anamnesis using “clinical-epidemiological reasoning and semiological technique”; and that, when performing the physical examination, the student must look after “the safety, privacy and comfort” of the patient and maintain an “ethical posture and technical dexterity”, while considering the “clinical history, ethnic-racial singularity, gender, sexual orientation and linguistic-cultural and gender identity”14. All these aspects must be permeated by adequate communication and other components of professionalism, including humanistic ones such as empathy7. The DCN also define the minimum limit of the medical course workload at 7,200 hours and that 35% of this workload is destined for clerkship14. However, they do not define limits or percentages of the specific workload of the contents taught before the clerkship, nor do they suggest when each content should be included in the curriculum. If, on the one hand, the non-definition of limits provides greater autonomy in curriculum planning, on the other hand, as this is permeated by discussions between teachers and managers and is influenced by the power of each teaching area, there is a risk of a greater workload of non-essential contents and a lower workload of others that are essential15, including semiology.
Taking into account the importance of semiology for medical practice, the non-definition of workload limits and the time of inclusion of curricular contents of the medical course before the clerkship, as well as the non-identification of a study in Brazil with a national scope that addressed these aspects of adult semiology in medical school curricula, the aim of our study was to analyze the distribution of adult semiology in Brazilian medical schools.
METHOD
Study design and ethical principles
This study had a cross-sectional and descriptive design. The research project was not submitted to the Ethics Committee for Research on Human Beings because the data were available on the internet and were of public domain.
Study universe and sample
The study universe consisted of 335 medical schools that existed in Brazil on December 31, 2020, according to the website of the Ministry of Education (e-MEC)16. According to the e-MEC, 24 schools were extinct or in the process of being extinct and, therefore, were not considered.
The schools’ inclusion criteria were: making the Political Project of the Course or Pedagogical Project of the Course (PPC) available on the internet, as well as the curricular matrix or, the program or teaching plans with information on the semester(s) or year(s) in which adult semiology was taught.
The schools’ exclusion criterion was not having started its academic activities until December 31, 2020.
Data collection
The data were collected between September and December 2020. Initially, we searched the date of inception of the schools and the beginning of the course on the e-MEC16 website and the Medical Schools’ websites17. Subsequently, the following Google search keys were used to locate the school, its pedagogical project or curricular matrix: ((“school name”) AND (“Policy Project of the Course” OR “Pedagogical Project of the Course” OR “curricular matrix” OR course syllabus OR curriculum OR “teaching plan”)). The most recent documents that could be found were used.
In the programs, we searched for the following terms regarding adult semiology: semiology, anamnesis, clinical history, study of signs and symptoms, physical examination, medical interview, semiotics and propaedeutics.
The following variables were collected: course inception date, geographic region and type of school administration, type of course curriculum, total course workload, total medical clerkship and adult semiology, both theoretical and practical, name of the discipline, of the module or axis that contained semiology and semester(s) and year(s) in which adult semiology was taught.
To calculate the workload, we considered only the disciplines, modules or axes that provided the specific workload of adult semiology, including signs, symptoms and examination by devices and systems, as well as clinical reasoning, when this was part of its content. We did not include the workloads related to pediatric semiology, gynecology and obstetrics, oncology and elderly health, due to their specificity regarding the age group and/or contexts that went beyond the scope of general adult semiology and would deserve their own study. However, when these were offered in modules and axes that contained adult semiology, they were mentioned, but without the workload.
The workload was standardized in clock hours, converting the provided hours into 45 and 50 minutes and the credits of 12 or 15 hours to the 60-minute hour. We consider the loads labeled as standard time as theoretical and those labeled as laboratory time as practical hours.
Data analysis
The data were entered into Microsoft Excel 2013 software and analyzed.
Descriptive statistics was used, analyzing the absolute and relative frequency for categorical variables and measures of central tendency for continuous variables. The normality of the distribution of continuous variables was analyzed using the Kolmogorov-Smirnov (K-S) test. In the results, we provide the mean and the Standard Deviation (SD) values, the 95% confidence interval (95%CI), the median and the 25th and 75th percentiles (P25 - 75) to provide comparisons with other studies; however, we indicated whether the distribution was normal or not.
The types of school administration were combined as ‘free tuition’ for federal and state schools and ‘not free tuition’ for municipal/community and private schools.
The association of two groups in continuous variables with normal distribution was analyzed with Student’s t test for independent samples and the association between more than two groups using One-Way Analysis of Variance (ANOVA), whereas the association of two groups of continuous non-parametric variables was analyzed with the Mann-Whitney-U test and between more than two groups with the Kruskal-Wallis test. Pearson’s chi-square test (chi2) was used to analyze the association of categorical variables and Wilcoxon’s test for two related samples to analyze the association between the median of the theoretical and practical workloads.
As some of the identified studies only contained the workload values of each assessed school1,12,13, based on the provided workloads, the means and median values were calculated, depending on the normality of their distribution, aiming to compare them with the findings of the present study.
The level significance was set at p < 0.05.
RESULTS
A total of 226 of the 335 medical schools active in Brazil in December 2020 (67.5%) were included in the present study, representing 103 of the 113 federal or state schools (91.1%) and 123 of the 222 municipal or private schools (55.4%).
The proportion of schools included in the study was similar by geographic region, chi2(4) = 4.30, p = 0.367. However, Brazil had more private schools in 2020 than federal and state schools, chi2(3) = 20.60, p < 0.01, and, consequently, non-free-tuition schools, chi2(1) = 14.13 , p < 0.01.
The time of existence of the medical course among the included schools was:
up to three years in 27 (11.9%);
between 4 and 6 years in 41 (18.1%)
between 7 and 19 years in 72 (31.9%)
between 20 and 40 years in 20 (8.8%);
between 41 and 60 in 42 (18.6%);
between 61 and 100 years in 16 (7.1%);
between 101 and 200 years in 6 (2.7%); and,
more than 200 years in two (0.9%).
As for the curriculum design, 84 of the 226 schools had a traditional curriculum, which concentrated the basic sciences in the first two years of the course (37.2%) and 142 schools integrated the curricular contents (62.8%) by modules or axes and called their curricula as:
Problem-Based Learning (PBL);
PBL and problematization;
PBL and Team-based learning (TBL);
TBL, PBL and problematization;
PBL, PjBL and problematization;
PBL, TBL, Project-based learning (PjBL);
Peer learning and problematization;
PBL, TBL and Case-based learning (CBL);
TBL, problematization and CBL;
PBL, TBL and PjBL; and,
Active methodologies (not otherwise specified).
The distribution of the time of inclusion of semiology in the curriculum of the 226 schools is shown in Figure 1. As depicted, it is most frequently inserted only in the 4th semester of the course. It can also be observed that while some schools teach semiology in just one or two semesters, others teach it throughout the first four years of the course.
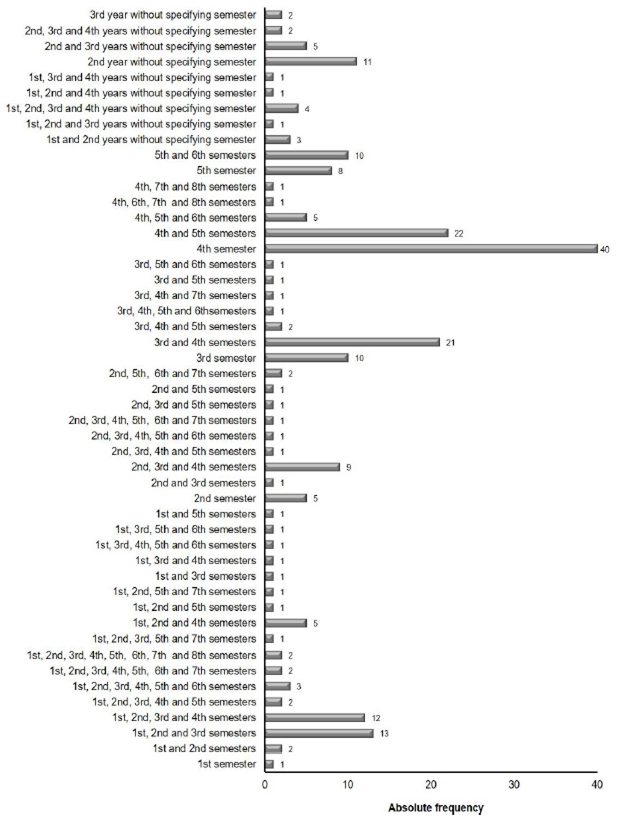
Source: the authors.
Figure 1 Distribution of the time of inclusion of adult semiology in the curriculum of the 226 active Brazilian medical schools in December 2020 that made this information available on the internet, per semester in schools with semester admission or per year in schools with annual admission.
Table 1 shows the distribution of semiology contents in the 226 analyzed schools. It can be observed that, in some schools, general semiology and clinical reasoning are offered in the 1st semester. Therefore, we remind readers that reasoning was only included as content when the school incorporated it into the semiology discipline. In schools that offered it as a separate discipline, it was not included in the semiology discipline. Therefore, it appears both in semiology and in the contents integrated into the axes and modules.
Table 1 Absolute frequency of distribution of adult semiology content among the 226 of the 335 active Brazilian medical schools in December 2020 that made it available on the internet, per semester or year, according to semester or annual school admission
| Course period | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Semiology contentsy | 1sts n | 2nds n | 1st yrb n | 3rds n | 4ths n | 2ndyr n | 5th n | 6th n | 3rdyr n | 7th n | 8th n | 4thyr n |
| General semiology | 47 | 46 | 10 | 48 | 84 | 21 | 40 | 16 | 10 | 4 | 2 | 2 |
| Anamnesis and doctor-patient relationship | 35 | 30 | 9 | 23 | 36 | 16 | 15 | 7 | 6 | 3 | - | 2 |
| Skin and adnexa | 4 | 5 | - | 1 | 10 | - | 2 | 1 | - | - | - | - |
| Head and neck | - | 2 | - | 5 | 9 | 1 | 4 | 1 | 1 | - | - | - |
| Lymph nodes | 1 | - | - | - | - | - | - | - | - | - | - | - |
| Abdomen | - | 5 | - | - | 27 | - | - | - | - | - | - | 1 |
| Signs and symptoms | 2 | 1 | - | - | 2 | 1 | 2 | 1 | - | - | - | - |
| Hemolymphopoietic system | 1 | - | - | - | - | - | 2 | 6 | - | - | - | - |
| Hematological semiology | - | 5 | - | - | 3 | - | - | - | - | 3 | - | - |
| Cardiovascular system | 2 | 14 | - | 19 | 24 | 4 | 17 | 4 | 2 | 3 | 1 | 5 |
| Locomotor system c | 3 | 7 | - | 11 | 19 | 2 | 9 | 5 | 1 | 5 | 2 | 5 |
| Rheumatological semiology | - | - | - | 1 | - | - | 3 | - | - | - | - | |
| Digestive system | 2 | 4 | - | 17 | - | 5 | 18 | 8 | 4 | - | - | - |
| Neurological semiology | 4 | 3 | - | 17 | 29 | 2 | 8 | 8 | 2 | 5 | 2 | 2 |
| Respiratory system | 1 | 18 | - | 19 | 20 | 5 | 16 | 4 | - | 7 | 2 | 6 |
| Endocrine system | 1 | - | - | 4 | 11 | - | 6 | 5 | - | 1 | - | 2 |
| Renal system d | - | 7 | - | 5 | 13 | 4 | 11 | 5 | 2 | 3 | - | 1 |
| Reproductive system | - | - | - | 5 | - | - | - | - | - | - | - | - |
| Genital semiology | - | - | - | - | 8 | - | - | - | - | - | - | - |
| Otorhinolaryngological semiology | - | - | - | - | 3 | - | - | 2 | - | - | - | - |
| Ophthalmological semiology | - | - | - | - | 2 | - | 1 | 4 | 1 | - | - | |
| Dermatological semiology | - | - | - | - | - | - | 1 | 1 | - | - | 1 | |
| Clinical reasoning | 4 | 1 | 2 | 13 | 17 | 8 | 9 | 4 | 4 | 2 | 1 | 4 |
Source: The authors.
Abbreviations: s - semester; yr - year; n - absolute frequency.
a. Offered in disciplines, modules or axes.
b. Schools with annual admission.
c. Also known as osteoarticular, orthopedic, osteomuscular and musculoskeletal semiology.
d. Also called urinary system and nephrological semiology.
It was only possible to identify the workload of 117 of the 226 medical schools (51.8%) and, among them, 44 were tuition-free (37.6) and 73 were not tuition-free (62.5%).
Table 2 shows the mean and median workload hours of the course, clerkship and semiology, showing that the workload of practical semiology classes was greater than the theoretical one. Table 3 shows the distribution of the semiology workload by region, type of administration, tuition-free/non-tuition free characteristic, and time of existence of the school. As shown, there was no statistical difference regarding any of these variables.
Table 2 Distribution of total workload and clerkship and adult semiology workload per year (including schools with semester and annual admission) in 117 of 335 medical schools active in Brazil in December 2020 that made the information available on the internet.
| Hours | |||
|---|---|---|---|
| Workload (in hours)a | Mean (SD) | 95%CI min - max | Median (P25 - 75) |
| Total semiology in the first year (n = 23) b | 120.3 (11.7) | 96.1 - 144.5 | 102.0 (75.0 - 160.0) |
| Theoretical semiology in the first year (n = 6) b | 37.2 (7.7) | 17.4 - 57.1 | 33.3 (26.2 - 48.0) |
| Practical semiology in the first year (n = 6) c | 76.7 (27.0) | 7.2 - 146.2 | 55.0 (45.0 - 97.5) |
| Without discriminating theoretical and practical semiology in the first year (n = 16) b | 117.7 (14.8) | 86.3 - 149.1 | 110.0 (60.0 - 175.0) |
| Total semiology in the second year (n = 96) c | 185.7 (10.1) | 165.7 - 205.7 | 180.0 (111.0 - 232.7) |
| Theoretical semiology in the second year (n = 36) c | 85.3 (12.0) | 60.8 - 109.8 | 73.5 (40.0 - 80.0) |
| Practical semiology in the second year (n = 36) c | 113.6 (12.1) | 88.9 - 138.2 | 85.0 (61.5 - 157.5) |
| Without discriminating theoretical and practical semiology in the second year (n = 57) c | 182.6 (12.9) | 156.9 - 208.4 | 180.0 (120.0 - 222.5) |
| Total semiology in the third year (n = 48) c | 210.3 (22.0) | 166.2 - 254.6 | 162.5 (120.0 - 281.5) |
| Theoretical semiology in the third year (n = 18) b | 75.8 (11.2) | 52.3 - 99.4 | 75.0 (38.3 - 100.0) |
| Practical semiology in the third year (n = 18) b | 118.5 (18.4) | 79.8 - 157.3 | 90.0 (47.9 - 180.0) |
| Without discriminating theoretical and practical semiology in the third year (29) c | 220.0 (32.9) | 152.6 - 287.5 | 166.7 (120.0 - 255.0) |
| Total semiology in the fourth year (n = 3) d | 66.7 (18.6) | -13.2 - 146.5 | 80.0 (55.0 - 85.0) |
| Total theoretical semiology (n = 50) c , e | 98.9 (10.3) | 78.2 - 119.7 | 77.5 (51.7 - 123.5) |
| Total practical semiology (n = 50) c , e | 141.4 (13.6) | 114.1 - 168.8 | 147.0 (64.5 - 180.0) |
| Total semiology without discriminating theoretical and practical contents (n = 68) c | 277.6 (21.5) | 234.7 - 320.4 | 240.0 (161.7 - 355.5) |
| Total semiology workload (n = 117) c | 266.3 (14.4) | 237.9 - 294.8 | 240.0 (165.4 - 338.2) |
| Total course workload c | 8,365.8 (80.9) | 8,205.5 - 8,526.1 | 8,223.0 (7,451.2 - 8,817.5) |
| Total clerkship workload c | 3,466.8 (75.3) | 3,317.7 - 3,615.8 | 3,398.0 (3,016.2 - 3,750.0) |
Source: The authors.
Abbreviations - SD: Standard Deviation; 95%CI: 95% confidence interval; min - max: minimum and maximum values; P25 - 75: 25th and 75th percentiles.
a. The total workload for each year includes the workload of the semesters in schools with semester admission and workload of the year in those with annual admission.
b. Normal distribution.
c. Non-normal distribution.
d. In the fourth year, only schools that did not discriminate the theoretical from the practical workload were identified.
e. Wilcoxon’s test comparing total theoretical with practical semiology workload: Z = - 3.99, p < 0.01.
Table 3 Total course load of adult semiology in 117 schools of 335 active medical schools in Brazil in December 2020 that made the information available on the Internet, per region, type of administration, tuition-free /non-free, and time of existence.
| Total semiology workload | |||
|---|---|---|---|
| Variable | Median (P25 - 75) | Statistical test and result | p |
| Region | |||
| North | 200.0 (180.0 - 340.0) | K-W, Chi 2(4) = 5.08 | 0.279 |
| Northeast | 222.5 (145.5 - 300.0) | ||
| Midwest | 315.0 (208.7 - 409.5) | ||
| Southeast | 284.2 (168.7 - 375.0) | ||
| South | 240.0 (160.0 - 300.0) | ||
| Type of administration | |||
| Federal | 210.0 (150.0 - 300.0) | K-W, Chi 2 (3) = 2.69 | 0.442 |
| State | 292.5 (180.0 - 366.5) | ||
| Municipal or community | 283.3 (177.5 -380.0) | ||
| Private | 240.0 (160.0 - 360.0) | ||
| Tuition-free | |||
| Yes | 240.0 (167.5 - 300.0) | Mann-Whitney U = 1672.5 | 0.614 |
| No | 240.0 (161.7 - 360.0) | ||
| Time of existence | |||
| up to 3 years | 160.0 (83.3 - 264.0) | K-W, Chi 2 (7) = 10.8 | 0.148 |
| 4 to 6 years | 230.0 (160.0 - 400.0) | ||
| 7 to 19 years | 200.0 (160.0 - 340.0) | ||
| 20 to 40 years | 270.0 (137.4 - 385.0) | ||
| 41 to 60 years | 291.7 (240.0 - 360.0) | ||
| 61 to 100 years | 240.0 (175.0 - 300.0) | ||
| 101 to 200 years | 325.0 (192.5 - 1.050.0) | ||
| More than 200 yearsa | 204.0 | ||
Source: The authors.
Abbreviations - P25-75: 25th and 75th percentiles; p: significance level; K-W: Kruskal-Wallis, chi2: chi-square.
a. Only one school included in the study was more than 200 years old
The percentage of the semiology workload in relation to the total course workload had a non-parametric distribution, with a median of 2.9% (P25-75 = 2.0 - 4.0) and a mean of 3.2% (SD = 0 .2; 95%CI = 2.8 - 3.5).
Frame 1 shows the names of the disciplines, modules and axes that contain semiology and the contents integrated to it in 142 schools of the 226 analyzed ones, per semester or year of inclusion in the course, according to the type of semester or annual admission of the school. It also shows that several contents provide opportunities for the learning of semiology, such as anatomy, pre-hospital care and fractures integrated with osteoarticular semiology.
Frame 1 Contents integrated into adult semiology in modules or axes, per semester in schools with semester admission and per year in schools with annual admission, in 142 of 226 schools that made this information available on the internet and were active in December 2020.
| Names of disciplines, modules, and axes that contain semiology Patient approach and pathophysiological and therapeutic bases of the main signs and symptoms; Bases: of diagnosis and therapy I, II, / human or pathophysiological diagnosis and propaedeutics of maturity and aging I to III; Internal Medicine: I and II / and clerkship; Diagnosis and therapy I, II; Health-Disease-Care Process II (1st and 2nd parts) / Disease II; Elements of general propaedeutics; Study of medicine I, II; Physiology and applied semiology I, II; Pathophysiology and propaedeutics; Fundamentals of: clinical I, II / practice and medical care I to IV / medical practice I, II and IV / semiology and medical propaedeutics; Major clinical syndromes signs and symptoms; Development of medical skills and attitudes I to III; Skills: I to IV / medical / medical I to VIII / clinical / clinics I, II and IV / clinics and attitudes I to III or I to V / clinics and attitudes in medicine I to III or I to IV / clinics, attitudes and bioethics / communication, techniques and humanistic skills I to IV / and humanities I to VI / specific II to IV / and community, medical and attitudes I, II, medical and communication I, II / and practices I, II / professionals I to VII / clinical professionals I, II / semiological I to VI; Introduction: to clinic I, III / to internal medicine / medical practice / medical propaedeutics / medical study / clinical examination and doctor-patient relationship / to semiology / medical semiology / medical semiology I, II; Initiation: to clinical examination / semiology; Laboratory skills II to V; Integrated Medicine I, III, IV and V; Clinical method I to IV; Clinical modules: circulation and gas exchange (I and II), Vital balance (III), Illness (IV), Doctor-patient relationship (V), Elementary health care and prevalent diseases (VI), Prevalent diseases and common complaints (VII); The clinical examination method; The patient and the bases of medicine: semiology, anatomophysiopathology and clinical pharmacology; The human being and their aggressors: introduction to semiology and medical propaedeutics; Perception, awareness and Emotion (Skills and Community axis); Practice: integrative II / interdisciplinary of teaching, service and community II / medical, professional and health work I to III; Practices: expanded III/ comprehensiveness to clinical method I, III and IV / medical I to V / of community health / Interdisciplinary; Propaedeutics: basic / medical / medical I to III / clinical / clinical I to III / general / of basic health care and care / health problems in adulthood / and imaging I and II / and semiology / advanced medical / by life cycle(s / segmental l I, II, III / anamnesis / clinical syndromes / semiotechniques; Clinical and epidemiological reasoning: normal semiology I, II / altered I to III; Adult Health I and II; Semiology: A and B / general, Adult / Adult I and II / medical / medical I to VII /general medical / of systems, and technical procedures / and propaedeutics/ and propaedeutics I to II/ and propaedeutics of adult/ medical I, II / and doctor-patient relationship I, II) / and semiotechniques/ and semiotechniques I to III / in internal medicine I to IV / special / specialized / specialties / altered II / and general outpatient clinic / integrated / integrated I, II / of adults and elderly I and II / anamnesis and propaedeutic systems and apparatus, cardiovascular, digestive, endocrine, Hemolymphopoietic, locomotor, nervous / neurological, reproductive; respiratory or urinary; Semiotechniques of clinical observation; Signs and Symptoms I, II; Curricular Unit Simulation of Professional Practice I to IV; e,- Health Surveillance and Integrated Semiology. |
| Content taught in modules or axes that integrate semiology 1stsemester History of medicine; anthropology and sociology in health; medical education in Brazil and worldwide; constitution of society; reason, science and faith; medical professionalism; education in human rights, the environment and the health system; bioethics and medical ethics; psychological, social and environmental aspects in health situations; family study; health surveillance, biosecurity; communication skills and relationship with the patient; Narrative-based medicine (NBM); Person-Centered Medicine (PCM); relationship between a healthy human body in community and society; care and caregiver in the medical area; Evidence-Based Medicine (EBM); Brazilian Unified Health System (SUS), primary health care (PHC); clinics and activities in PHC; health prevention and promotion in communities; multidisciplinary team in patient care; disease, diagnosis, therapy, prognosis; medications; laboratory; basic procedures to medical practice; clinical reasoning; basic life support; first aid; technique for removal of polytraumatized patients; fracture; surgical technique and surgical skills; relationships of the different organic, mental and relational systems; integration of anatomy and physiology knowledge; microscopy and cytology; morphophysiology of the digestive system and attached glands; growth and development; nutrition; risk for cardiovascular disease (CV); imaging exams; undergraduate research (UR) skills; informatics, telemedicine; medical decision support and geographic information systems; electronic patient file and medical prescription, Picture Archiving and Communication System (PACS). |
| 2ndsemester Sociology of health and main stages of the life cycle; ethnicities; medical training; care and caregiver in the medical area; bioethics and academic and medical ethics in family and community health care; environmental and health education; principles of health policy and management of the SUS; social control in the management of health services; the community and the Basic Health Units (BHUs); PHC II; social, environmental, behavioral and psychosomatic factors of the syndromes; medical records; understand the patient in their social, cultural and family context and in their ethnic-racial aspects; health communication; understand, inform and educate patients, family members and communities regarding health promotion, prevention, treatment and rehabilitation of diseases; basic preventive actions in pediatrics; regional infectious diseases; biosecurity; drug administration routes; infusion velocity; collection and storage of biological materials for laboratory; basic surgical techniques; first aid in drowning victims, burns and accidents with venomous animals; pre-hospital approach to trauma; basic life support; organization of urgency and emergency health services; hospital infection commission and control service; semiology of the elderly; death declaration and certificate and related legislation; morphophysiology and pathophysiology related to semiology; clinical reasoning; undergraduate research; computer skills; information technology applied to health; EBM. |
| 1st year Ethics; biosecurity; biological, social, psychological phenomena; care and educational process; problems of people, family and community; public health policies, SUS and Family Health Program (FHP); expanded clinic; medical procedures and complementary examinations; medicines and routes of administration, vaccines, dressings and injections; pre-hospital care; basic life support; laboratory and imaging tests; electrocardiogram (ECG); clinical reasoning; library; social communication; access to contemporary means of medical information and training for critical reading; EBM. |
| 3rdsemester History of Medicine; ethical, humanistic, social and psychological values; spirituality and religion; ethics and bioethics; medical professionalism and communication with patients; National Patient Safety Program; medical files, records and rights of the patient and the physician; International Classification of Diseases (ICD); health and work; person-centered medicine; psychosocial aspects of medical practice; aging; mourning and stages of acceptance of death; clinical reasoning; semiology of children and adolescents; semiology of the elderly; technical language in medicine and sign language; approach to patients and their families; medium and high complexity health care and system; PHC programs and policies for patients with mental illnesses; biosecurity; nutritional, environmental, sanitary and epidemiological surveillance; clinical epidemiology; pharmacology/pharmacology; medicalization and health; nursing; anesthesiology; medical procedures, immunization; asepsis and antisepsis principles and procedures; histology, physiology, general pathology, pathophysiology of the circulatory, locomotor, nervous, respiratory, renal and male reproductive system; laboratory and imaging tests of the urinary system and digestive tract; medical psychology in the doctor-patient relationship (DPR); cultural, psychological, gender and affective aspects related to pain and pain scales; pathophysiology of the main signs and symptoms; social, environmental, behavioral and psychosomatic factors of digestive, endocrine and reproductive syndromes; integration between anatomy, histology, physiology, general pathology, psychology, parasitology, microbiology, immunology, semiology, health, family and society and imaging; diagnosis and laboratory tests of regional infectious diseases; family and community medicine; outpatient and infirmary practices, activities in the BHUs and community health centers; research and academic work; internet use/informatics skills. |
| 4thsemester Humanities; environment and sustainability; health psychology; bioethics and medical ethics; patient rights; student behavior; interdisciplinarity and multidisciplinary practices; health, family and society; care in PHC in communities; public health policies and programs aimed at specific LGBT and rural populations; health promotion and quaternary prevention; environmental, epidemiological and health surveillance; information system and health indicators; communication and informatics skills training; cultural differences, patients with difficult interaction, communication of bad news in sensitive situations; clinical reasoning; obstetric and pediatric semiology; semiology of the elderly; mental health; basic nursing techniques/ practice; principles of asepsis and antisepsis; microbiology, parasitology, virology and immunology; infectious and parasitic diseases; medical registration tools and medication prescription (prescriptions); medical certificate, medical leave, medical expertise; pharmacology/drugs; diagnosis and conduct in prevalent diseases; SUS; laboratory tests; parasitological stool examination; radiographies (X-rays), Ultrasonography (USG), computed tomography (CT), arteriography, endoscopy, colonoscopy, manometry, pH-metry, cholangiopancreatography, cholangioresonance and related laboratory tests; study of anatomical parts of pathologies of the main human body systems; study of autopsies; semiology, thanatology and medical accountability; the terminal patient and the dying process; horizontal integrations; anatomopropaedeutic correlation using knowledge of histology, physiology, general pathology, pathophysiology and semiology; research and academic work. |
| 2ndyear Ethics; care and educational process; teamwork; health education; communication, leadership and management skills; reports; foreign language; ethics; medical procedures; EBM; pediatric semiology; monitoring; venous puncture; basic laboratory equipment; gynecological and obstetric physical examination; semiology of the elderly; oncologic semiology; laboratory; ECG; imaging diagnosis of arthrosis, osteoporosis, Chronic Obstructive Pulmonary Disease; calcifications in atheromatous plaques, cerebral atrophy; ECG in overloads and blocks; surgical techniques; pre-scientific work project (ECW). |
| 5thsemester Human rights education; medical psychology; development of reflective thinking; health communication; biosecurity; interdisciplinarity and multidisciplinary practices; nasogastric probing technique; obstructions of the digestive and urinary tract and taking sanitary measures; infectious and parasitic diseases; lumbar puncture; pregnancy and childbirth, neonatal period, childhood, adolescence; semiology of the elderly; laboratory diagnostic instruments for urethritis and cervicitis; laboratory and imaging tests; medical prescription; pathogenesis and pathophysiology of major clinical signs and symptoms; pathological anatomy and clinical pathology; clinical reasoning; diagnostic and therapeutic management of the most frequent disorders in adults; pathophysiology, clinical manifestations, complementary examinations, radiology and clinical and surgical approach of the main diseases of the respiratory, CV and digestive systems; interpretation of ECG. |
| 6thsemester Medicine and Humanities; environmental education; medical psychology; health communication; health and society; interdisciplinarity and multidisciplinary practices; physician performance in the SUS; practices in internal medicine; person-centered clinical method; development of the expanded medical diagnosis; rational use of medications; horizontal integrations; clinical and pathophysiological study of prevalent diseases in the region; pathological anatomy and clinical pathology of prevalent diseases of the region; introduction to drug therapy; theoretical-practical activities of pediatric and gynecological semiology and propaedeutics/child and adolescent health; semiology of the elderly; oncologic semiology; special medical semiology and surgical techniques; physical examination techniques in abnormal situations with emphasis on patients with a history of trauma and chronic and acute blood loss and mental and behavioral disorders; rational request skills for the performance and interpretation of complementary exams; study of laboratory diagnostic instruments of urethritis, cervicitis; bladder catheterization; obstructions of the digestive and urinary tract and taking sanitary measures; presuppositions of renal replacement therapy; organ transplant; method. |
| 3rdyear Medical ethics and bioethics; EBM; care and educational process; psychosomatic medicine; leadership, management and communication skills in relation to the different patterns of patient behavior; foreign language; role of the physician in the interdisciplinary team; expanded clinic; biological, social, psychological phenomena; problems of people, family and community, related to adulthood, reproduction, sexuality, aging; semiology of children, of adolescents and women; semiology of the elderly; psychiatric anamnesis; complementary methods; clinical correlation of simpler cases; clinical reasoning; handling and knowledge of the basic surgical instruments; techniques/collection of biological material for examinations; containment; anterior nasal packing (otorhinolaryngology); drainage of abscesses; advanced life support; emergency management. |
| 7thsemester Medicine and humanities; health and society; medical skills; horizontal integrations; anatomy, histology and pathology, applied to the study of propaedeutics; pathophysiology of diseases and their relationship with signs and symptoms; clinical reasoning; medical prescription; rational request and interpretation of complementary exams; performance and interpretation of complementary exams; basic surgical techniques; method; death certificate. |
| 8thsemester SUS; person-centered clinical method; psychiatric semiology; horizontal integrations; anatomy, histology and pathology, applied to adult propaedeutics; clinical reasoning; urgencies and emergencies; advanced life support in children and adults; method. |
| 4thyear Care and educational process; biological, social, psychological phenomena; problems of people, family and community; expanded clinic; communication, leadership and management skills; management of patients and families in difficult situations; informed consent; palliative care; thanatology; EBM; techniques for collecting biological material for laboratory tests; low-complexity surgical procedures; obstetrics; clinical correlation with more complex clinical cases; care in medical specialties in prevalent and / or life-threatening pathologies; advanced life support in children and adults; diagnosis of arthritis and arthrosis, fractures and dislocation, pyogenic arthrosis, ischemic and hemorrhagic stroke, cardiomegaly, pneumothorax and pleural effusion; diagnosis of electrocardiographic alterations of myocardial ischemia and some arrhythmias. |
Source: The authors.
DISCUSSION
In our study, tuition-free medical schools made their curricula available on the internet more often than non-tuition-free medical schools. Perhaps, this fact is due to the more recent increase in the number of private schools, which had not yet included their curricula on their websites. Also, as some of these schools already existed and were incorporated into business groups, usually, their names had changed and, when we could not find the data related to a school belonging to a business group, this also happened with all their other schools.
We found eight names related to semiology, without considering the name of modules or axes that integrated it or their qualification and association with other terms. These were: semiotechniques, propaedeutics, semiology, semiology and propaedeutics, signs and symptoms, initiation to clinical examination, introduction to internal medicine and introduction to medical practice. The modules and axes that integrated it had specific logics in the integrated contents in each school and a certain creativity regarding the denominations.
In the Brazilian study in medical schools in Rio de Janeiro1, it was observed that some of them differentiated semiology from propaedeutics, with the first being related to anamnesis and, often, to the physical examination, whereas the second was more specific to the physical examination. The term introduction to internal medicine was mentioned in a European study13 and the term propaedeutics was found in a Cuban study8, a European study12 and a Colombian study9. In the latter, the terms ‘introduction to medical practice and human conduct’ were also found to designate the teaching of semiology.
In our study, we observed that semiology was more frequently included only in the 4th semester of the course, unlike the study carried out in Rio de Janeiro1, in which it was more frequently included in the 5th and 6th semesters; and the Colombian study9, in which it was more frequently included in two semesters or from the 4th to the 7th semesters; and the Cuban study, in which semiology was included in the third year of the course under the name “Clinical Propaedeutics and Pathophysiology” in the academic year of 1985-1986, and “Clinical Propaedeutics and Clinical/Imaging Laboratory” in the academic year of 2010-20118.
Clinical reasoning was the only content included in all semesters of the course before the clerkship among some Brazilian medical schools in our study. In the North American research, its teaching started in the first two semesters of undergraduate medical school and was associated with physical examination in 84 of 116 analyzed schools (79%), although 60% of the time was dedicated to the physical examination11.
Some schools included in our study integrated semiology with other areas of knowledge, such as anthropology and sociology, and with other contents, including biosecurity, ethics and bioethics, narrative-based medicine, concepts and principles of the Brazilian Unified Health System (SUS, Sistema Único de Saúde), communication, first aid, medication application, anatomy, physiology, histology, imaging, collection and analysis of laboratory tests, among others, in accordance with article 29 of the DCN14.
In the Colombian study, semiology was integrated with basic biomedical and clinical disciplines9 and in the North American study, 92 schools associated the teaching of physical examination with the patient’s clinical history (87%), 59 with clinical reasoning (56%), 64 with anatomy (60%) and 56 with physiology or pathophysiology (53%), with these contents being taught in an associated manner in 48 of these schools (45%)11. Neither the study carried out in Colombia9, nor the study carried out in the United States11 mentioned the integration of semiology or physical examination to contents of the Human and Social Sciences, in addition to communication and ethics.
We consider that the student should be seen as a professional in training since the first day of the course and, as semiology is the foundation of clinical practice, its teaching should start in the first semester of the course, integrated with clinical contents and contents of basic, social and human sciences, including communication, ethics and other components of professionalism. This inclusion should be continued throughout the course, showing increasing complexity, so that the future physician can establish a good doctor-patient relationship, perform an anamnesis considering the biopsychosocial, cultural and spiritual aspects related to the health-disease process, carry out a high-quality physical examination and demonstrate comprehensive clinical reasoning.
When comparing the values of the total workload of the course that we found with that of other studies, we observed that it is lower than what appears in the Cuban study plan, which is over 9,000 hours throughout the six-year course8 and similar to the study carried out in Rio de Janeiro, which comprised 8,426.9 hours (SD = 272.1; 95%CI = 7,839.0 - 9,104.7)1. However, it is much higher than the average load of 21 of the 32 European schools, which was 4,497.8 hours (SD = 270.2; 95%CI = 3,934.2 - 5,061.4)12, and of 16 medical schools in Southeast Europe, which was 4,990.8 hours (SD = 113.6; 95%CI = 4,748.2 - 5,233.4)13.
In relation to Europe, the duration of the medical course in many of its countries is of five years12 and the shorter course load is probably a result of the reform movement in higher education that resulted in the Bologna Process18. In medical education, in 1998, this movement generated the declaration of the World Federation for Medical Education, which highlighted the need to change the structure and process of medical education to prepare physicians to meet the needs and expectations of society, deal with the increasing scientific knowledge and technological advances, develop the capacity for lifelong learning and adapt to changes in the context and in the health system. One of its recommendations was the development of a core curriculum with essential contents for medical training, aiming to avoid an overload of contents, which should be supplemented by optional subjects19. These aspects were also highlighted in the Bologna Declaration18.
As for the median workload of semiology among 117 Brazilian medical schools in our study, we observed that it tends to be lower than that of the 14 schools studied in the study performed in Rio de Janeiro, which was 368.7 hours (SD = 42.7; 95%CI = 276.4 - 461.0), equivalent to 4.6% (SD = 0.6; 95%CI = 3.1 - 6.0) of the course load1. However, this trend may have occurred because the study carried out in Rio de Janeiro included only 11.8% of Brazilian schools existing in 2006.
Regarding the studies in Europe, the median of semiology workload hours found in our study is well above that found in medical schools in 18 European countries, which was 135.0 hours (P25 - 75 = 94.0 - 220.5 )12 and in the 16 medical schools located in Southeast Europe, which was 105.0 hours (P25 - 75 = 22.5 - 135.0)13. However, the percentage of semiology workload in relation to the course in the study carried out with 18 European countries was 4.2% (SD = 3.5; 95% CI = 2.6 - 5.8)12, similar to the present study, while that of the study carried out in Southeast Europe was 2.0% (SD = 1.3; 95%CI = 1.2 - 2.7)13, lower than that found in our study.
It was not possible to make comparisons with some studies. The Colombian study provided data that allowed calculating only the workload of semiology in one school, which was 240.0 hours, since in the other four schools, it was provided as credits, without clarifying how many hours these credits were equivalent to9. In the Cuban study, the workload of semiology was 495 hours in the academic year of 1985 - 1986 and 686 hours in the academic year of 2010 - 2011; however, it included other contents with which it was integrated, including pathophysiology, laboratory and imaging8. The study performed in the United States only analyzed the workload of the physical examination content, whose average was 82.0 hours (SD = 71.0), with a minimum value of 10 hours and a maximum of 360 hours. In addition to the fact that physical examination was just a part of the teaching of semiology, it was integrated with other contents in some of these schools11. Moreover, on the website of the Association of American Medical Colleges (AAMC), among its data up to 2013-2014, it was stated that the teaching of “introduction to physical diagnosis” had an average of 30.8 weeks, without informing its contents or what the weekly workload was10.
We did not find any differences in the median of the total workload of semiology per region, tuition-free characteristic, type of administration and time of existence of the school in the 117 schools that specified it. This finding may perhaps indicate that, despite having included only 34.9% of the total of 335 Brazilian schools, the values may represent the rest of the schools, but that cannot be stated with certainty.
The resent study showed that the workload of practical semiology was higher than the theoretical one. This finding was similar to that of the study performed in Rio de Janeiro, whose schools had a mean theoretical workload of 105.5 (SD = 15.9; 95%CI = 71.3 - 140.1) hours and an average of 241.7 practical workload hours (SD = 24.5; IC95% = 167.2 - 316.2)1. However, even though the theoretical workload was similar to that of the present study, the practical workload tends to be higher. Nevertheless, we emphasize that it showed a low representativeness of Brazilian medical schools1.
The limitations of our study included the collection of data available on the internet, which resulted in the inclusion of only 67.5% of Brazilian medical schools, with a predominance of tuition-free schools. The non-inclusion of many non-tuition-free schools was due to the fact that many private schools were incorporated into the same business groups that did not provide details of the curriculum of their schools on the internet. Some of these schools have even changed their names, making it more difficult to find them. Additionally, only 117 schools (51.8% of the 226 included and 34.9% of all existing schools) provide data on their semiology workload. These limitations pose a risk of bias and the results related to this workload should be interpreted with caution. However, as it was similar per region, type of administration and tuition-free characteristic, we believe that, perhaps, the results may have some validity. When searching for comprehensive national and international studies, which included the workload of semiology, we found only a few that allowed comparisons with our study and we could see the difficulty in obtaining a representative number of schools, especially when their number in the country is very large.
The strength of our study was allowing the identification of the time when semiology was introduced in the course and the contents that can be integrated into its teaching, as well as providing national and international comparison with the workload of 117 Brazilian medical schools.
For future studies, we suggest obtaining the pedagogical projects and learning programs directly from each school, so that, in addition to including more schools, the school viewpoint regarding its curriculum, pedagogical approach, including teaching and evaluation, and the practice scenarios used in teaching semiology can be assessed. Additionally, we suggest incorporating interviews with managers, teachers and students, for a better understanding of their perception of this teaching.
CONCLUSIONS
A total of 226 medical schools of the 335 active ones in December 2020 in Brazil were studied.
More than half integrates semiology into modules or axes and most of them offer semiology only in the 4th semester. However, some schools offer it in the 1st semester of the course, and, among them, there are those that offer it from the 1st to the 8th semesters of the course.
Of the 117 schools that make the semiology workload information available on the Internet, the total semiology workload is 240.0 hours (P25-75 = 165.4 - 338.2), with no difference per geographic region, tuition-free characteristic, type of administration and time of existence of the school, and the median of its percentage in the course is 2.9% (P25-75 = 2.0 - 4.0).
REFERENCES
1. Midão CMV. O ensino da semiologia médica no estado do Rio de Janeiro (tese). São Paulo: Escola Paulista de Medicina, Universidade Federal de São Paulo; 2006 [acesso em 5 ago 2020]. Disponível em: Disponível em: http://repositorio.unifesp.br/bitstream/handle/11600/21550/Tese-10178.pdf?sequence=1&isAllowed=y . [ Links ]
2. Silva RMFL, Rezende NA. O ensino de semiologia médica sob a visão dos alunos: implicações para a reforma curricular. Rev Bras Educ Med. 2008;32(1):32-9. [ Links ]
3. Azevedo MH, Paiva AFA, Santiago LD, Silva BNV, Pacheco PV, Silva DF, et al. Iniciação ao exame clínico: primeiras vivências do estudante de Medicina na interação com o paciente hospitalizado. XI Encontro de Iniciação à Docência. João Pessoa: Universidade Federal da Paraíba; 2007 [acesso em 15 out 2020]. Disponível em: Disponível em: http://www.prac.ufpb.br/anais/xenex_xienid/xi_enid/monitoriapet/ANAIS/Area6/6CCMDMIMT03.pdf . [ Links ]
4. Rezende JM. Fundamentos etimológicos da linguagem médica. [acesso em 20 de abril 2022]. Disponível em: Disponível em: http://ibmexporto.com.br/material_suplementar/fundamento_etimologicos_da_linguagem_medica.pdf [ Links ]
5. Silva AC, Rudge AM. Construindo a noção de sintoma: articulações entre psicanálise e pragmática. Psicol USP. 2017;28(2):224-9. [ Links ]
6. Dicionário etimológico: etimologia e origem das palavras. Propedêutica [acesso em 22 jan 2021]. Disponível em: Disponível em: https://www.dicionarioetimologico.com.br/propedeutica/#:~:text=Do%20grego%20Pro%2C%20antes%20e,ao%20ensino%20de%20determinada%20mat%CA9ria . [ Links ]
7. Devine OP, Harborne AC, Horsfall HL, Joseph T, Marshall-Andon T, Samuels R, et al. the analysis of teaching of medical schools (AToMS) survey: an analysis of 47,258 timetabled teaching events in 25 UK medical schools relating to timing, duration, teaching formats, teaching content, and problem-based learning. BMC Med. 2020;18(1):1-22. [ Links ]
8. Aguilera EÁM, Díaz NT, Sacasas JAF, Gómez MP, Figueredo SS, Cobelo JMD. Cronología de los mapas curriculares en la carrera de Medicina. Rev Cuba Educ Medica Super. 2015;29(1):93-107. [ Links ]
9. Pineda CC, García PH, Tehelen J, Ruiz O, Yandi J. Formación en semiología médica: una caracterización desde la práctica. Educ Educ. 2014;17(1):71-90. [ Links ]
10. Association of American Medical Colleges. Curriculum reports. Clerkship requirements by discipline. Percentage of Medical Schools with Separate Required Clerkships by Discipline and Academic Year [acesso em 20 fev 2021]. Disponível em: Disponível em: https://www.aamc.org/data-reports/curriculum-reports/interactive-data/clerkship-requirements-discipline . [ Links ]
11. Uchida T, Park YS, Ovitsh RK, Hojsak J, Gowda D, Farnan JM, et al. Approaches to teaching the physical exam to preclerkship medical students: results of a national survey. Acad Med. 2019;94(1):129-34. [ Links ]
12. Dušek T, Bates T. Analysis of European medical schools’ teaching programs. Croat Med J. 2003;44(1):26-31. [ Links ]
13. Likic R, Dusek T, Horvat D. Analysis and prospects for curricular reform of medical schools in Southeast Europe. Med Educ. 2005;39(8):833-40. [ Links ]
14. Brasil. Resolução nº 3, de 20 de junho de 2014. Institui Diretrizes Curriculares Nacionais do Curso de Graduação em Medicina e dá outras providências. Brasília; 2014 [acesso em 16 mar 2019]. Disponível em: Disponível em: http://portal.mec.gov.br/index.php?option=com_%20docman&view=download&alias=15874-rces003-14&category_%20slug=junho-2014-pdf&Itemid=3019 2. [ Links ]
15. Marcondes E, Lima-Gonçalves E, coordenadores. Educação médica. São Paulo: Sarvier; 1998. [ Links ]
16. Brasil. Instituições de educação superior e cursos cadastrados. Brasília: Ministério da Educação; 2007 [acesso em 12 fev 2020]. Disponível em: Disponível em: http://emec.mec.gov.br . [ Links ]
17. Nassif ACN. Escolas médicas do Brasil. Escolas Médicas; 2014 [acesso em 12 fev 2019]. Disponível em: Disponível em: https://www.escolasmedicas.com.br/escolas-medicas-todas.php . [ Links ]
18. The European Higher Education Area. The Bologna Declaration of 19 June 1999: Joint declaration of the European Ministers of Education; 1999 [acesso em 28 mai 2022]. Disponível em: Disponível em: http://www.bologna-bergen2005.no/Docs/00-Main_doc/990719BOLOGNA_DECLARATION.PDF . [ Links ]
19. The Executive Council of the World Federation for Medical Education. International standards in medical education: assessment and accreditation of medical schools’ educational programs. A WFME position paper. Med Educ . 1998;32:549-58. [ Links ]
Received: April 18, 2022; Accepted: July 17, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
