










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML
 Enviar este artigo por email
Enviar este artigo por emailCompartilhar

 Permalink
PermalinkRevista Brasileira de Educação Médica
versão impressa ISSN 0100-5502versão On-line ISSN 1981-5271
Rev. Bras. Educ. Med. vol.46 no.3 Rio de Janeiro 2022 Epub 03-Ago-2022
https://doi.org/10.1590/1981-5271v46.3-20220005
EXPERIENCE REPORT
Medical education in Cardiopulmonary Resuscitation: Didactic transposition from traditional-presential to remote-interactive with simulation
1
 http://orcid.org/0000-0001-9151-7032
http://orcid.org/0000-0001-9151-7032
1
http://orcid.org/0000-0003-3625-1525
1
http://orcid.org/0000-0002-1788-4653
1
http://orcid.org/0000-0003-4043-6442
1
http://orcid.org/0000-0001-8095-6560
2
http://orcid.org/0000-0002-7688-2674
1Faculdade de Medicina de Jundiaí, Jundiaí, São Paulo, Brazil.
2Escola Paulista de Enfermagem, São Paulo, São Paulo, Brazil.
Introduction:
The didactic transposition of the traditional in-person teaching-learning process to the remote-interactive one with simulation in cardiopulmonary resuscitation was a strategy implemented by teachers to promote cognitive, psychomotor, and reflective education on the ethical aspects of first-year medical students in times of pandemic.
Experience report:
This is an experience report with a descriptive and reflective approach, which is a multiprofessional and multidisciplinary collaborative result of eight teachers, aiming to achieve educational goals. It took place in 2021, at the School of Medicine of Jundiaí (FMJ), in the disciplines of Basic Care and First Aid Notions and Bioethics and Medical Humanities. The activities were planned to be carried out with the 120 enrolled students, through the Google Classroom platform, linked to the institutional account, synchronously and asynchronously. Different teaching strategies, materials, media, and languages were combined with online hypermedia and offline multimedia teaching materials, consisting of different types/formats.
Discussion:
The transposition was unique and challenging for teachers and students. The collaborative interprofessional teaching work was fundamental for the integration of the two disciplines and the materialization of education in the simulated theoretical and practical dimensions. It is believed that the approach used, combining some technological means, craft simulators, allowed the teaching and learning in basic life support in the cardiopulmonary resuscitation topic in the context of the restrictions imposed by the ongoing pandemic. The students had the opportunity to develop cognitive, technical, and behavioral skills, as well as assess their progress, performing and receiving immediate feedback, as well as through formative assessment without grade assignment. Conclusion: The didactic transposition of the teaching and learning process mediated by technologies allowed students to approach the theoretical content and safely participate in clinical simulations in their homes. However, there is no comparative study that shows that the development was similar to in-person teaching. Consequently, it will be necessary for the pedagogical advisory board to evaluate the possible learning gaps and how they can be overcome throughout the course.
Keywords: Education, Medical, Undergraduate; Education, Distance; Simulation Training; Bioethics; Cardiopulmonary Resuscitation
Introdução:
A transposição didática do processo de ensino-aprendizagem presencial-tradicional para o remoto-interativo com simulação em reanimação cardiopulmonar foi uma estratégia implementada por docentes para promover a educação cognitiva, psicomotora e reflexiva sobre aspectos éticos de estudantes de Medicina primeiranistas em tempos de pandemia.
Relato de experiência:
Trata-se de um relato de experiência de abordagem descritiva e reflexiva, resultado colaborativo multiprofissional e multidisciplinar de oito docentes, visando atingir objetivos educacionais. Ocorreu em 2021, na Faculdade de Medicina de Jundiaí (FMJ), nas disciplinas de Fundamentos Assistenciais e Noções de Primeiros Socorros, e Bioética e Humanidades Médicas. As atividades foram planejadas para serem realizadas com os 120 estudantes matriculados, por meio da plataforma Google Sala de Aula, vinculada à conta institucional, de maneira síncrona e assíncrona. Combinaram-se diferentes estratégias de ensino, materiais, mídias e linguagens com materiais didáticos on-line hipermidiáticos e off-line multimidiáticos, compostos por diferentes tipos/formatos.
Discussão:
A transposição foi singular e desafiadora para docentes e discentes. Fundamentou-se o trabalho colaborativo interprofissional docente na integração das duas disciplinas e na materialização da educação nas dimensões teóricas e práticas simuladas. Acredita-se que a abordagem utilizada, combinando alguns meios tecnológicos, simuladores artesanais, possibilitou, no contexto das restrições impostas pela pandemia em curso, o ensino e a aprendizagem em suporte básico de vida, na temática reanimação cardiopulmonar. Os estudantes tiveram a oportunidade de desenvolver competências cognitivas, técnicas e comportamentais, e avaliar o seu progresso, realizando e recebendo feedbacks imediatos, bem como por meio de avaliação formativa sem atribuição de nota.
Conclusão:
A transposição didática do processo de ensino e aprendizagem mediada por tecnologias possibilitou que os estudantes se aproximassem do conteúdo teórico e participassem de simulações clínicas em seus lares com segurança. Porém, não há um estudo comparativo que mostre que o desenvolvimento foi semelhante ao presencial. Consequentemente, será necessário que a assessoria pedagógica avalie as possíveis lacunas de aprendizagem e como poderão ser superadas ao longo do curso.
Palavras-chave: Educação de Graduação em Medicina; Educação a Distância; Treinamento por Simulação; Bioética; Reanimação Cardiopulmonar
INTRODUCTION
Brazilian medical education began in Bahia, in 1808, with the arrival of the Portuguese imperial family in Brazil1. The curriculum has undergone transformations, the most recent one being the establishment of the National Curriculum Guidelines (NCG) in 20142. There have been several changes, but it is worth noting that the medical course remains with a six-year duration, in-person format and, classically, the curricular matrix is structured into three cycles: basic, clinical and internship. However, since the notification of the first case of infection with the severe acute respiratory syndrome coronavirus 2 (SARS CoV-2), biosecurity and safety measures have been adopted, which led the Ministry of Education and Culture (MEC), on March 19, 2020, to authorize, on an exceptional basis, the replacement of the in-person course disciplines by classes that used remote information and communication means and technologies, except for the internship3.
The Brazilian Association of Medical Education (ABEM, Associação Brasileira de Educação Médica) recommends that there must be a discipline focused on first aid or basic life support (BLS) in the first two years of undergraduate school. Among the 17 topics suggested by ABEM, ten are covered in the first year of undergraduate school at Faculdade de Medicina de Jundiaí (FMJ), in the disciplines of Basic Care and First Aid, with theoretical and practical activities4.
In the teaching plan of the discipline of Basic Care, until 2019, the manual skills training in BLS was based on theoretical teaching and practical in-person activities, carried out in safe and controlled environments, with simulators.
Faced with the situation of concern caused by the pandemic scenario, it became challenging to teach subjects that demand psychomotor development in a non-in-person manner to students who have started medical school. This unexpected change from in-person to emergency remote teaching in a virtual learning environment (VLE) has led the professors of the discipline to adapt to the new reality with strategies used in distance learning (DL), taking into account the moment, the topic and the available infrastructure5.
Regarding the BLS related to the care of a person suffering from cardiorespiratory arrest (CRA), it was necessary not only to transpose the theoretical-cognitive activities, but also the psychomotor ones.
Aiming to achieve educational goals in cardiopulmonary resuscitation (CPR) in the virtual environment, we sought to readjust the traditional in-class theoretical-practical teaching to remote-interactive teaching with simulation, including the discussion of the ethical aspects involved in caring for individuals in CRA. Thus, the general objective of this experience report is to describe didactic-andragogical strategic actions adopted to transpose in-person medical education with simulation in CPR to the remote-interactive type.
EXPERIENCE REPORT
This is an experience report of a descriptive and reflective approach by eight teachers. The experience of remote-interactive teaching with simulation in BLS in the CPR topic took place in the first half of 2021 and added the setting of the disciplines of Basic Care and First Aid notions (D1) and Bioethics and Medical Humanities (D2), from the Department of Public Health. Both are taught to students enrolled in the first year of the undergraduate medical course at Faculdade de Medicina de Jundiaí (FMJ), located in the city of Jundiaí, state of São Paulo, Brazil.
The discipline of Basic Care, taught by four nursing professors, has a workload of 72 hours. Specifically for the object-class of this report, entitled “First Aid: Basic Life Support for a person in cardiorespiratory arrest outside the hospital environment”, two hours of theory and three hours of practice were planned, with time being defined under the expectation of:
Developing scientific knowledge (cognitive competence), technical skills (cognitive and procedural competence) and ethical and humanized attitudes (personal and social competence), based on clinical protocols and guidelines using the best scientific evidence in urgencies and emergencies;
Integrating personal and collaborative learning into the multiple spaces of everyday life, and the physical world into the digital one;
Combining activities that enable students to face situations in which they may experience clinical and traumatic emergencies in the cardiorespiratory arrest topic.
The discipline of Bioethics and Medical Humanities is also taught in the first semester of the FMJ undergraduate medical course, with a workload of 72 hours. The teacher in charge of the course is a social scientist with a background in public health. One of the objectives of the discipline is to develop decision-making skills regarding the ethical issues involved in the care process. In this sense, it aims to help students to also relate these skills to the Code of Medical Ethics and the laws related to professional practice6. The discussion of the ethical aspects involved in caring for people in cardiopulmonary arrest was included in the broader discussion on bioethics and the end of life.
For the didactic transposition, a task force was implemented, which involved, in addition to the teachers of the two aforementioned disciplines, also the collaborative work of a statistician and a physician who teach, respectively, the disciplines of Research in Health and Propaedeutics at FMJ; and a nurse, a teacher of the discipline of Nursing and Emergencies and Intensive Care and Introduction to Basic Techniques, in the Nursing and Medical course, respectively, at Universidade Federal de São Paulo. Based on this multi-professional and multi-disciplinary collaborative work, adjustments were made in the teaching-learning process to adapt what was planned to be taught in-person with simulation to the new remote approach.
Interactive remote education in VLE is understood as a teaching-learning modality in a virtual classroom, with andragogical activities mediated by technologies and digital platforms, where the communication between people occurs through the interconnection of computers at the internet5),(7)-(8. Communication in this cyberspace occurs asynchronously and synchronously. In the first way, teachers and students do not need to be simultaneously connected online, in the same virtual space, for communication to occur between them. As for the second, that is necessary7.
Simulation, in turn, is an active and participatory teaching methodology, whose controlled environment can be adapted to the needs of the moment and the hypothetical situation of reality 9)-(11). The student integrates theory and practice, experiences situations of mistakes and successes through the repetition of procedures until they are successful, improves their actions through feedback, evaluation and reflection, so they can develop the competence to care without the risk of causing harm to the patient 9)-(12. Traditionally, it is practiced as an in-person activity.
Alternatively, the simulation can be applied remotely. Therefore, telesimulation emerges as a teaching-learning modality that allows people to remotely participate in this process based on clinical simulation13.
Based on these concepts, plans were developed for interactive remote teaching with simulation involving both disciplines, with the integration of active methodologies and Digital Information and Communication Technologies (DICT).
The educational objectives of the lesson plans of the two disciplines and of the scenario template with different techniques were based on Bloom’s taxonomy13)-(17. The 2014 NCG and the American Heart Association protocols were also used to define the theoretical and practical content related to BLS in CPR2),(18)-(24. To support the discussion of the bioethical aspects of CPR, we used the so-called Principlism Theory, the Code of Medical Ethics and Resolutions 1805/2006, 1995/2012 of the Federal Council of Medicine 6),(24)-(26.
The activities were planned to be carried out on the Google Classroom platform, linked to the institutional account, where all the content used to mediate education was hosted. Different teaching strategies, materials, media and languages were combined with hypermedia online and multimedia offline teaching materials, consisting of different types/formats (Table 1).
Table 1 Teaching strategy, media elements and didactic materials. Jundiai, São Paulo, Brazil, 2021.
| Teaching and learning strategies | Media elements | Didactic materials |
|---|---|---|
| Integrative lecture: (D1 and D2) | Virtual classroom | Slide projection through a computer program |
| Texts | ||
| Recorded classes | ||
| Videos | ||
| Audios | ||
| Chats | ||
| Staging/Dramatization (D1) | Virtual classroom | Simulation Scenario and Handcrafted Simulators |
| Group Simulation Training (D1) | ||
| RCDP (D1) | ||
| Training by Individual Simulation (D1) | Videos | |
| Discussions by class separately (D1) | Virtual classroom Chats | Checklist |
| Discussions with all classes (D2) | ||
| Discussions in groups of 15 students |
Abbreviations: Discipline 1: Basic Care and First Aid notions (D1); Discipline 2: Bioethics and Medical Humanities (D2); Rapid-Cycle Deliberate Practice (RCDP)
Source: The authors
Therefore, it was possible to present the content on CPR using diversified language with strategies and materials organized in three different moments, called Student Preparation for interactive remote teaching with simulation, learning activities and self-assessment.
Student Preparation: The student was asked to create two handcrafted simulators, a PET bottle torso and an Automatic External Defibrillator (AED) (Figure 1). They were asked to build them a week before the scheduled date for the theoretical-practical class, according to the guidelines of the teachers and a video posted27 on the wall of the virtual classroom. The validation of the simulators was carried out by the D1 teachers before the simulated practices. Functionality and similarities with a human thorax and an AED were verified.
Source: Prepared by the authors based on the photos received from students and teachers
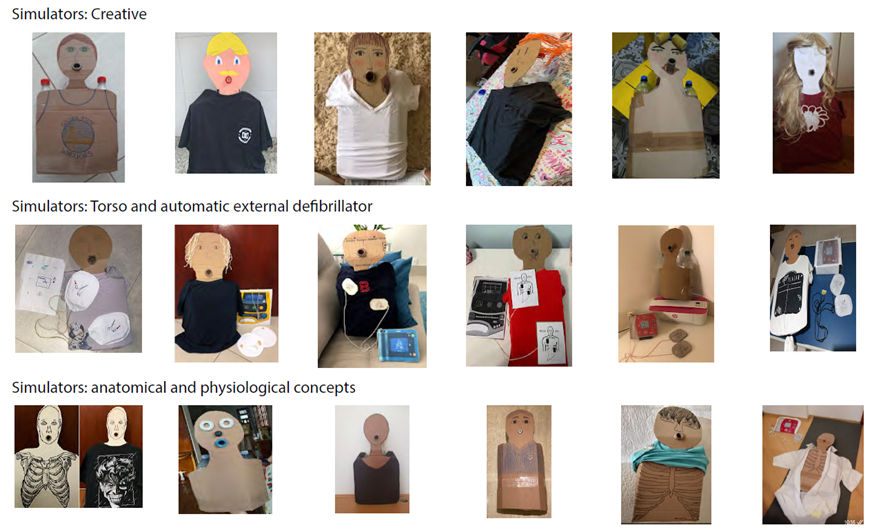
Figure 1 Sample of handcrafted cardiopulmonary resuscitation simulators built by medical students. Jundiai, São Paulo, Brazil, 2021.
In this phase, a survey of previous knowledge was also carried out, and the educational objectives and the competences to be developed were presented to the students.
Learning activities: The 120 students enrolled in the first year of the medical course were divided into two groups of 60 students, according to the day scheduled for the interactive remote theoretical-practical classes in VLE. All of them had the opportunity to participate in the planned activities, as shown in Table 2.
Table 2 Learning activities, assessment and student adherence. Jundiai, São Paulo, Brazil, 2021.
| Learning activity | Type of communication | Interaction | Grade assignment | Presence | Adherence N (%) |
|---|---|---|---|---|---|
| Construction of the torso | Asynchronous | Individual | No | No | 104 ( 87) |
| Construction of the AED | Asynchronous | Individual | No | No | 09 (7.5) |
| Video Production | Asynchronous | Individual | No | No | 02 (1.7) |
| Class 1 - Basics BLS - CRA _CPR | Synchronous | T/S Group | No | Yes | 120 (100) |
| Dramatization | Synchronous | T/S Group | No | Yes | 120 (100) |
| Class 2 - Bioethics | Synchronous | T/S Group | No | Yes | 120 (100) |
| Discussion - Bioethics | Synchronous | T/S Group | No | Yes | 120 (100) |
| Training of competences | Synchronous | T/S Group | No | Yes | 120 (100) |
| Rapid-cycle deliberate practice | Synchronous | T/S Group | No | Yes | 120 (100) |
| Training of competences | Asynchronous | Individual | No | No | 02 (1.7) |
| Student’s self-evaluation | |||||
| Pre-test: Theoretical knowledge (FQ) | Synchronous | Individual | No | No | 26 (21.7) |
| Post-test: Theoretical knowledge (FQ) | Synchronous | Individual | No | No | 21 (17.5) |
| Bioethics (FQ) | Synchronous | Individual | No | No | 21 (17.5) |
| Satisfaction (FQ) | Asynchronous | Individual | No | No | 11 (9.2) |
| Self-confidence (FQ) | Asynchronous | Individual | No | No | 11 (9.2) |
| Video-recorded images (Checklist) | Asynchronous | Individual | No | No | 02 (1.7) |
Note: Number of participants (N); Percentage (%); Automatic External Defibrillator (AED); Basic Life Support (BLS); Cardiopulmonary Arrest (CPA); Cardiopulmonary Resuscitation (CPR); Teacher and Student (T/S); Forms-type questionnaire (QF).
Fonte: Prepared by the authors.
After providing the theoretical background and discussions on the ethical aspects, the training was carried out, which took place in a VLE, at home, with handcrafted simulators built by the students themselves, alone or with the participation of the family or housemates.
In the distance skills training, two teachers synchronously dramatized CPR care for a person in CPA in a home simulation scenario. They dramatized the stages of care, according to the literature, demonstrated the student’s correct body positioning to perform CPR and solved doubts.
After this stage, the students performed chest compressions, using the handcrafted torso, to the rhythm of the song “Stayin Alive”. The four teachers followed three cycles in the virtual classroom and gave immediate feedback. They paid attention to body positioning between the students and handcrafted simulators and the automation of regular compression skills of descending and ascending thoracic movements.
Subsequently, the Rapid-cycle Deliberate Practice (RCDP) was carried out, also remotely and synchronously, in groups consisting of a maximum of 15 students, virtually monitored by a teacher14. Scenarios were created that reproduced CPA situations at home. Each of the students performed the CPR technique and four clinical cases were simulated with a progressive cycle of complexity. Time varied from student to student. Although the complexity of the first two cases was lower, the practice required more time, due to the greater number of interventions and feedbacks. The mistakes made by the students and scored by the teachers were overcome in the next cycle and in the subsequent scenario. In each scenario, the knowledge and skills were added to the entire group. The teachers used a guiding checklist.
It was also proposed to the students to be an active actor in their learning process. They were asked to produce a video in which they carried out the hypothetical care of a person in CRA and evaluated the recorded images of the CPR using a checklist provided by the teachers. This asynchronous clinical simulation was another alternative to assign meaning from theory to practice, as it is believed that, driven to use imagery resources, students can have more diversified and non-linear actual and sensory practical experiences, and that, in the face of situations of coping and discoveries, they are led to reflect, identify their weaknesses and stimulated to learn7)-(8.
Formative assessment was performed by the faculty during competence training and RCDP and by students themselves who agreed to self-assess. Instruments were created to measure theoretical, technical-scientific and ethical-legal knowledge, procedural skills (psychomotor skills): semi-structured questionnaires using Google Forms (FQ) and checklist; and the Student Satisfaction and Self-Confidence in Learning Scale, validated in Brazil28, was also used.
DISCUSSION
The reported experience confirms that the transposition of the traditional model to remote-interactive teaching with simulation, consisting of theoretical-practical activities, was unique and challenging for teachers and students, as also observed in other contexts in this pandemic situation29.
The urgency with which this transposition had to be carried out, the lack of prior training for teachers and the lack of available technological infrastructure constituted the most evident obstacles in this process. However, the interprofessional and collaborative practice between professors allowed the integration of each one’s individual skills into the planning and implementation of emergency remote teaching with clinical simulation. This integration between teachers with different backgrounds added a diversity of values to the process in its different stages. It was also a challenging situation for the students, as, in addition to andragogical activities, they had to handcraft simulators and set up scenarios for clinical simulation in their homes. However, it was observed that for some, it was a moment of pleasure, creativity, association with other disciplines and socialization with the family. It is believed that the making of handcrafted simulators, by the students themselves for clinical simulation,
(...) stimulates creativity, problem-solving, teamwork, multidisciplinary work and communication between peers and other agents. These are some of the necessary skills for the training of health professionals, usually with few opportunities to be worked during undergraduate school and residency courses (p.122)30.
The integration of approaches from the two disciplines - Basic Care and Bioethics - also contributed to expanding the inclusion of students into the CPR topic, as the discussion of the proposed clinical cases, also carried out from the bioethical viewpoint, took the debate beyond the technical aspects and stimulated the reflection on the role of future doctors as those who will take care of people and their families, and not just clinical cases. In this sense, the reported experience is in line with what the NCG describe as characteristics of the training of graduates in medicine: “general, humanistic, critical, reflective and ethical...”2.
At the same time, however, there was a low adherence of students to the proposal of self-assessment during the experience, which made it impossible to accurately diagnose learning, satisfaction with the remote teaching methodology with simulation and self-confidence to perform the CPR maneuvers. It is possible that this low adherence was related, on the one hand, to a certain disappointment by the students - first-year medical students - in the face of the limitations imposed by the pandemic to the possibility of carrying out the activities in person. On the other hand, it is also possible to think that, even though they were informed about the purpose of this self-assessment, they did not understand the heuristic significance of this experience to promote the learning of CPR, even remotely. The resistance in adhering to the set of proposed activities may be due, in part, to the greater affinity and feeling of security related to the traditional learning style.
Studies on learning styles can shed some light on this behavior31)-(34. There are four “psychological profiles of learning” based on the ways of grasping and transforming the “new”: concrete experience, active experimentation, abstract conceptualization and reflective observation. Each learning style adapts to certain teaching modalities. As an example, the styles “active experimentation” and “concrete experience” would have greater affinity with clinical simulation than the styles “reflective observation” and “abstract conceptualization”. In this report, the “inventory of learning styles” was not carried out, which limits the possibility of making more concrete inferences in this regard.
The interactive remote environment and the low-fidelity simulation are sufficient; the initiative took place at the beginning of the course and, therefore, the learning objectives were specific to this phase. However, there is no comparative study that shows that the development was similar to the in-person one. Consequently, it will be necessary for the pedagogical advisory board to assess possible learning gaps and how they can be overcome throughout the course.
Even considering the aforementioned limitations, it is believed that the approach used, combining different technological means, made it possible to teach and learn CPR by first-year medical students in the context of the restrictions imposed by the ongoing pandemic. The students had the opportunity to develop cognitive, technical and behavioral skills, as well as to assess their progress, giving and receiving immediate feedback, as well as through formative assessment without grading assignment.
FINAL CONSIDERATIONS
The didactic transposition of the teaching and learning process mediated by technologies made it possible for first-year medical students to safely approach the theoretical content and participate in synchronous and asynchronous clinical simulations in their homes. However, it was observed that the students had difficulty in adopting a more active and self-assessment attitude.
REFERENCES
1. Machado CDB, WuoI A, HeinzleI M. Educação médica no Brasil: uma análise histórica so-bre a formação acadêmica e pedagógica. Rev Bras Educ Med. 2018;42(4):66-73. doi: 10.1590/1981-52712015v42n4RB20180065. [ Links ]
2. Brasil. Resolução CNE/CES nº 3, de 20 de junho de 2014. Institui Diretrizes Curriculares Nacionais do curso de graduação em Medicina. Brasília: Ministério da Educação, Conselho Nacio-nal de Educação, Câmara de Educação Superior; 2014 [acesso em 20 fev 2021]. Disponível em: Disponível em: http://portal.mec.gov.br/index.php?option=com_docman&view=download&alias=15874-rces003-14&category_slug=junho-2014-pdf&Itemid=30192 . [ Links ]
3. Brasil. Portaria nº 345, de 19 de março de 2020. Altera a Portaria MEC nº 343, de 17 de março de 2020. Brasília: Ministério da Educação; 2020 [acesso em 20 abr 2020]. Disponível em: Disponível em: https://pesquisa.in.gov.br/imprensa/jsp/visualiza/index.jsp ?jornal=603&pagina=1&data =19/03/2020 &totalArquivos=1 . [ Links ]
4. Pereira Júnior GA. Projeto de ensino de urgência e emergência da Abem [diapositivo]. Sim-pósio de Urgência e Emergência Núcleo RBCE; 17 nov 2016; Ribeirão Preto, SP. [ Links ]
5. Brasil. Decreto nº 5.622, de 19 de dezembro de 2005. Regulamenta o art. 80 da Lei nº 9.394, de 20 de dezembro de 1996, que estabelece as diretrizes e bases da educação nacional, que dispõe Educação a Distância (EAD) no Brasil. Brasília: Senado Federal; 2005 [acesso em 20 abr 2020]. Disponível em: Disponível em: https://legis.senado.leg.br/norma/566415/publicacao/15727450 . [ Links ]
6. Conselho Federal de Medicina. Código de Ética Médica: Resolução CFM nº 2.217, de 27 de setembro de 2018, modificada pelas Resoluções CFM nº 2.222/2018 e 2.226/2019. Brasília: CFM; 2019 [acesso em 20 abr 2020]. Disponível em: Disponível em: https://portal.cfm.org.br/images/PDF/cem2019.pdf . [ Links ]
7. Lacerda AL, Silva T. Materiais e estratégias didáticas em ambiente virtual de aprendizagem. Rev Bras Estud Pedagog. 2015;96(243):321-42. doi: 10.1590/S2176-6681/337812844. [ Links ]
8. Silva LV. Tecnologias digitais de informação e comunicação na educação: três perspectivas possíveis. Revista de Estudos Universitários. 2020;46(1):143-59 [acesso em 20 nov 2021]. Disponível em: Disponível em: http://periodicos.uniso.br/ojs/index.php/reu/article/view/3955/3731 . [ Links ]
9. Batista NA. Prefácio. In: Pereira Júnior GA, Guedes HTV, organizadores. Simulação em saúde para ensino e avaliação: conceitos e práticas. São Carlos: Cubo; 2021 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://issuu.com/editoracubo/docs/issuu-abem . [ Links ]
10. Padilla M. Apresentação. In: Pereira Júnior GA, Guedes HTV, organizadores. Simulação em saúde para ensino e avaliação: conceitos e práticas . São Carlos: Cubo , 2021 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://issuu.com/editoracubo/docs/issuu-abem . [ Links ]
11. Pinheiro MIC. Apresentação. In: Pereira Júnior GA, Guedes HTV, organizadores. Simulação em saúde para ensino e avaliação: conceitos e práticas . São Carlos: Cubo , 2021 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://issuu.com/editoracubo/docs/issuu-abem . [ Links ]
12. Pereira Júnior GA. As Diretrizes Curriculares Nacionais (DCNs) e a evolução do conceito de competências para marcos de competências e “Entrustable Professional Activities” (EPAS): um entendimento necessário para adequações da formação médica”. In: Pereira Júnior GA, Guedes HTV, organizadores. Simulação em saúde para ensino e avaliação: conceitos e práticas . São Carlos: Cubo , 2021 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://issuu.com/editoracubo/docs/issuu-abem . [ Links ]
13. Lima SF, D’Eça Junior A, Silva RAR, Pereira Júnior GA. Conhecimentos básicos para estruturação do treinamento de habilidades e da elaboração das estações simuladas. In: Pereira Júnior GA, Guedes HTV, organizadores. Simulação em saúde para ensino e avaliação: conceitos e práticas . São Carlos: Cubo , 2021 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://issuu.com/editoracubo/docs/issuu-abem . [ Links ]
14. Castro LD, Couto TB. Prática Deliberada em Ciclos Rápidos: uma estratégia moderna de simulação. Sci Med. 2018;28(1): 1-6. doi: 10.15448/1980-6108.2018.1.28849. [ Links ]
15. Bloom BS, Hastings JT, Madaus GF. Handbook on formative and summative evaluation of student learning. New York: McGraw-Hill; 1971. [ Links ]
16. Ferraz APCM, Belhot RV. Taxonomia de Bloom: revisão teórica e apresentação das adequações do instrumento para definição de objetivos instrucionais. Gest Prod. 2010;17(2):421-31. doi: 10.1590/S0104-530X2010000200015. [ Links ]
17. Anderson LW, Krathwohl DR, Bloom BS. A taxonomy for learning, teaching, and assessing: a revision of Bloom’s taxonomy of educational objectives. New York: Longman; 2001. [ Links ]
18. American Heart Association. Destaques das diretrizes de RCP e ACP de 2020 da American Heart Association. Versão em português. Dallas: American Heart Association; 2020 [acesso em 20 abr 2021]. Disponível em: Disponível em: https://cpr.heart.org/-/media/CPR-Files/CPR-Guidelines-Files/Highlights/Hghlghts_2020ECCGuidelines_Portuguese.pdf . [ Links ]
19. American Heart Association. Heart disease and stroke statistics - 2020 Update: a report from the American Heart Association. Circulation. 2020;3:141(9) : e139 - e596. doi: 10.1161/CIR.0000000000000757. [ Links ]
20. Bernoche C, Timerman S, Polastri TF, Giannetti NS, Siqueira AWS, Piscopo A, et al. Atualização da Diretriz de Ressuscitação Cardiopulmonar e Cuidados de Emergência da Sociedade Brasileira de Cardiologia - 2019. Arq Bras Cardiol. 2019;113(3):449-663. doi: https://doi.org/10.5935/abc.20190203. [ Links ]
21. American Heart Association. Destaques das atualizações direcionadas nas diretrizes de 2019 da American Heart Association para ressuscitação cardiopulmonar e atendimento cardiovascular de emergência [acesso em 20 abr 2021]. Disponível em: Disponível em: https://suportebasicodevida.com.br/wp-content/uploads/2019/11/up-date-2019-aha.pdf . [ Links ]
22. American Heart Association. Destaques da American Heart Association 2015. Atualização das diretrizes de RCP e ACE. Versão em português. [Internet]. Dallas: American Heart Association , 2015 [acesso em 20 abr 2021]. Disponível em: Disponível em: http://cdn.laerdal.com/downloads/f3831/2015-AHA-Guidelines-Highlights-Portuguese.pdf . [ Links ]
23. Bauer AC, Carvalho DFS, Franco GF, Costa JM, Carvalho DFS, Taha Junior K, et al. Suporte básico de vida: atualização das diretrizes da American Heart Association 2017. Revista Científica Multidisciplinar Núcleo do Conhecimento. 2018;3(4):83-98 [acesso em 20 abr 2021]. Disponível em: Disponível em: https://www.nucleodoconhecimento.com.br/saude/suporte-basico-de-vida?pdf=14936 . [ Links ]
24. Beauchamp TL, Childress JF. Principles of biomedical ethics. 4th ed. New York: Oxford University Press; 1994. [ Links ]
25. Conselho Federal de Medicina. Resolução nº 1.805, de 28 de novembro de 2006. Brasília; 2006 [acesso em 26 maio 2021]. Disponível em: Disponível em: https://sistemas.cfm.org.br/normas/visualizar/resolucoes/BR/2006/1805 . [ Links ]
26. Conselho Federal de Medicina. Resolução nº 1.995, de 31 de agosto de 2012. Dispõe sobre as diretivas antecipadas de vontade dos pacientes. Brasília; 2012 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://sistemas.cfm.org.br/normas/visualizar/resolucoes/BR/2012/1995 . [ Links ]
27. Szpilman D. Com fazer um manequim de RCP de forma simples. Vídeo: 3,5 min. [acesso em 23 abr 2021]. Disponível em: Disponível em: https://www.youtube.com/watch?v=DNnyGnovkPo . [ Links ]
28. Almeida RGS, Mazzo A, Martins JCA, Baptista RCN, Girão FB, Mendes IAC. Validation to Portuguese to the scale of students satisfaction and self-confidence in learning. Rev Lat Am Enfermagem 2015; 23(6):1007-13. doi: http://dx.doi.org/10.1590/0104-1169.0472.2643. [ Links ]
29. Bastos RA, Carvalho DRS, Brandão CFS, Bergamasco EC, Sandars J, Cecilio-Fernandes D. Solutions, enablers and barriers to online learning in clinical medical education during the first year of the Covid-19 pandemic: a rapid review. Med Teach. 2021;44(2): 187-95. doi: 10.1080/0142159X.2021.1973979. [ Links ]
30. Knobel R, Costa RRO. Confecção e uso de simuladores de baixo custo: experiência da Medicina e Enfermagem. In: Pereira Júnior GA, Guedes HTV, organizadores. Simulação em saúde para ensino e avaliação: conceitos e práticas . São Carlos: Cubo , 2021 [acesso em 20 nov 2021]. Disponível em: Disponível em: https://issuu.com/editoracubo/docs/issuu-abem . [ Links ]
31. Kolb DA. Experiential learning: experience as the source of learning and development. New Jersey: Prentice-Hall; 1984. [acesso em 20 abr 2021]. Disponível em: Disponível em: https://www.researchgate.net/publication/235701029_Experiential_Learning_Experience_As_The_Source_Of_Learning_And_Development . [ Links ]
32. Caetano C, Luedke R, Antonello ICF. The importance of identifying learning styles in medical education. Rev Bras Educ Med . 2018:42(3):189-93. doi: 10.1590/1981-52712015v42n3RB20170111r1ING. [ Links ]
33. Sobral DT. Estilos de aprendizagem dos estudantes de Medicina e suas implicações. Rev Bras Educ Med . 2005;29(1):5-12. doi: 10.1590/1981-5271v29.1-002. [ Links ]
34. Schmitt CS, Domingues MJCS. Estilos de aprendizagem: um estudo comparativo. Avaliação. 2016:21(2):361-86. doi: 10.1590/S1414-40772016000200004. [ Links ]
Received: March 25, 2022; Accepted: May 18, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
