










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format
 Send this article by e-mail
Send this article by e-mailShare

 Permalink
PermalinkRevista Brasileira de Educação Médica
Print version ISSN 0100-5502On-line version ISSN 1981-5271
Rev. Bras. Educ. Med. vol.47 no.1 Rio de Janeiro Jan./Mar. 2023 Epub Feb 16, 2023
https://doi.org/10.1590/1981-5271v47.1-20220206
ORIGINAL ARTICLE
Demographic aspects and access to the pedagogical projects of medical courses in Brazil
1
, study conceptualization, treatment and analysis of data, investigation, methodology, validation, writing and approval of the final version of the manuscript http://orcid.org/0000-0003-3464-0658
http://orcid.org/0000-0003-3464-0658
1
, guiding the study conceptualization, methodology, validation, writing and approval of the final version of the manuscripthttp://orcid.org/0000-0003-2290-4492
1
, study design, analysis and interpretation of data, writing the manuscript, review of the intellectual content, approval of the final version of the manuscripthttp://orcid.org/0000-0003-0841-2985
1Universidade de São Paulo, São Paulo, São Paulo, Brazil.
Introduction:
The expansion of higher education in Brazil is recent. In the medical field, with the advent of the “Mais Médicos” Program, this expansion became feasible and culminated with the publication of new National Curricular Guidelines (DCN, Diretrizes Curriculares Nacionais) for undergraduate medical courses. The Pedagogical Course Project (PCP) translates what is accomplished in the course and works as an instrument of communication between the institution and society. The analysis of the PCPs of Higher Education Institutions provides the identification of elements that point to the convergence or move away from the changes proposed by the DCN 2014.
Objective:
To describe demographically in Brazil the number of public and private medical courses by state and region of the federation, the number of available vacancies, and access to the PCPs of these schools through a systematized methodology.
Method:
A study was carried out in all institutions with medical courses in Brazil by the year 2021. The search for the PCPs was carried out in the institutional website. In case of lack of information, an electronic message was sent to the medical course coordination. When it was not possible to contact the coordinator directly through the institutional website, a message was sent to the coordinator by accessing their curriculum lattes.
Results:
A total of 336 medical schools were identified, 115 (34.2%) of which were public and 226 (65.8%) private ones. A higher concentration of courses was observed in the southeast region (41.3%), followed by the northeast region (24.6%). Of the public institutions, the northeast region has the highest concentration of schools (35.6%), followed by the southeast region (26%). The opposite was observed regarding the private institutions. A total of 134 PCPs were obtained (39.8% of the total), 83% from public schools and 17% from private ones.
Conclusion:
Although the availability of the pedagogical information document on the institution’s website is an obligation, this was not verified in reality, which makes it necessary to implement policies for valuing and monitoring PCP availability, thus facilitating its access by the most interested parties: students, the academic community and researchers in the field of medical education.
Keywords: Undergraduate Medical Education; Public Health Policies; Evaluation of Medical School Course Programs; Schools of Medicine
Introdução:
A ampliação da educação superior no Brasil é recente. Na área médica, com o advento do Programa Mais Médicos, essa expansão tornou-se viável e culminou com a publicação de novas Diretrizes Curriculares Nacionais (DCN) para o curso de graduação em Medicina. O projeto pedagógico do curso (PPC) traduz o que se realiza no curso e funciona como instrumento de comunicação entre a instituição e a sociedade. A análise dos PPC das instituições de ensino superior propicia a identificação de elementos que apontam para convergência ou se afastam do preconizado nas mudanças pretendidas pelas DCN de 2014.
Objetivo:
Este estudo descreve demograficamente no Brasil o número de cursos de Medicina públicos e privados por estado e região da Federação, o número de vagas disponíveis e o acesso aos PPC dessas escolas por meio de metodologia sistematizada.
Método:
Realizou-se um levantamento de todas as faculdades com curso de Medicina no Brasil, no ano de 2021. A procura dos PPC foi realizada no site institucional. Em caso de ausência da informação, encaminhamos mensagem eletrônica à coordenação do curso de Medicina. Na indisponibilidade de contato direto com a coordenação pelo site institucional, encaminhamos mensagem ao coordenador por meio do acesso ao seu Currículo Lattes.
Resultado:
Foram identificadas 336 escolas médicas, 115 (34,2%) públicas e 226 (65,8%) privadas. Observamos a maior concentração de cursos na Região Sudeste (41,3%), seguida da Região Nordeste (24,6%). Das instituições públicas, o Nordeste é a região que mais concentra as escolas (35,6%), seguida da Região Sudeste (26%). Quanto às instituições privadas, ocorre o inverso. Obteve-se um total de 134 PPC (39,8%), sendo 111 (83%) das escolas públicas e 23 (17%) das privadas.
Conclusão:
Embora a disponibilização do documento de informação pedagógica no site da instituição seja obrigatória, isso não foi verificado em realidade, o que corrobora a necessidade de políticas de valorização e fiscalização da disponibilidade do PPC para facilitar o seu acesso pelos maiores interessados: alunos, comunidade acadêmica e pesquisadores da área da educação médica.
Palavras-chave: Educação de graduação em Medicina; Políticas em saúde pública; Avaliação dos programas de curso das escolas de Medicina; Faculdades de Medicina
INTRODUCTION
Medical education in Brazil is influenced by political decisions and situations, economic models, social intervention proposals and the management of different public policies. All of these elements characterized the expansion and distribution of medical courses in the country1. Also, the expansion of higher education in Brazil is recent and was made possible by the National Education Plan of 2014-2024, with policies to increase vacancies and support the interiorization of the institutions2.
In the medical field, this expansion became viable with the advent of the “More Doctors” Program (PMM, Programa Mais Médicos). Best known for the emergency axis of the program, whose aim was the immediate call for doctors to work in priority regions of the Brazilian Unified Health System (SUS, Sistema Único de Saúde), the program also aims at the improvement of infrastructure and equipment for health, the increase in the number of vacancies for graduation in medicine and specialization/medical residency, in addition to the improvement of medical training in Brazil, whose proposals culminated in the publication of new National Curriculum Guidelines (DCNs, Diretrizes Curriculares Nacionais), which are now mandatory3, for the undergraduate medical course4. The new DCNs for medical school intend to promote a more generalist, humanistic and critical medical training, with physicians that have the ability to work at different levels of health care, with social responsibility and commitment to the defense of citizenship, human dignity and comprehensive health care for the population5.
Regarding the creation of medical schools in Brazil, we experienced a significant change in the last century. The first medical schools in Brazil were created in 1808 and there were only three of these institutions until the first decade of the 20th century. The 60s were characterized by an intense process of expansion. In just five years, 35 schools were created and, after slowing down due to the warnings of the great deterioration in the quality of medical education in the following decades, a new phase of school creation was triggered in the 90s, reaching a total of 113 institutions by the end of the century. Recently, at the end of 2010, the number of active courses comprised 179, reaching a total number of 356 in 20211),(6),(7.
Many studies have been carried out on the practical effects of DCNs and their own conception, but few are related to the consequences on the pedagogical course projects (PCPs) in the new medical schools8. The PCP is the instrument that guides the course actions and aims at the quality of teaching and the student professional training. This document also details the disciplines and syllabi, teaching strategies, differentiated pedagogical practices, research and extension activities, faculty and student body profiles and all other activities developed to meet the course objective and professional profile. The PCP translates what is carried out in the course and works as a communication tool between the institution and society. Therefore, it must be available to the public on the course website and at the coordinating office.
Knowing how to access such documents will allow us to assess the limitations of studies aiming to evaluate related topics and understand how Higher Education Institutions (HEIs) describe their documents.
The aim of this study is to describe a methodology for accessing the PCP of medical courses in Brazil and the difficulties in obtaining them. An outline of the scenario of medical courses and their vacancies in Brazil in the year 2021 was also carried out.
METHOD
This is a descriptive study, with a quantitative and qualitative approach, whose methodological procedure consisted of document analysis. The data collection involved medical schools from all over Brazil.
In February 2021, a survey was carried out about all medical schools in Brazil through the website of the Ministry of Education and Culture (MEC)9, searching for the PCPs, while also identifying the course coordinators.
Initially, the search was carried out on each institutional website, identifying the availability of information.
In the absence of the information, an electronic message was sent to the medical course coordination email, available on the institutional website, requesting the document to be sent by the coordinators in charge. When the coordination email was not available, we tried, as an alternative, to send a message through the contact form, which is sometimes the only means of communication available. In the absence of contact with the coordination, either through email or the available form, a message was sent to the coordinator through access to their lattes curriculum, using the option of sending a message to the author. Therefore, we intended to reach those responsible for making the information available.
The obtained information was grouped in a table containing the data using the Microsoft Excel 2010 software. After a first analysis, the extinct/terminated courses and the ones that had not yet been started were excluded from the sample.
During the analysis of the information, the descriptive statistics of absolute and relative frequencies was adopted, which was presented as charts and tables.
Because this is a study that involved the use of publicly accessible information, there was no need to apply the Free and Informed Consent Form, in accordance with Resolution number 510/2016 of the National Health Council (CNS, Conselho Nacional de Saúde). The project was approved by the Research Ethics Committee of HCFMUSP under number 3.406.777.
RESULTS
A total of 356 higher education institutions (HEIs) were assessed through the MEC website, of which 122 were public and 234 private. Of the public ones, 07 HEIs were removed from the analysis because they had not started the course yet. Of the private ones, 11 were excluded for not having started the course and 02 for having terminated the course. Thus, 336 medical schools were selected for the study, of which 115 were public and 221 private.
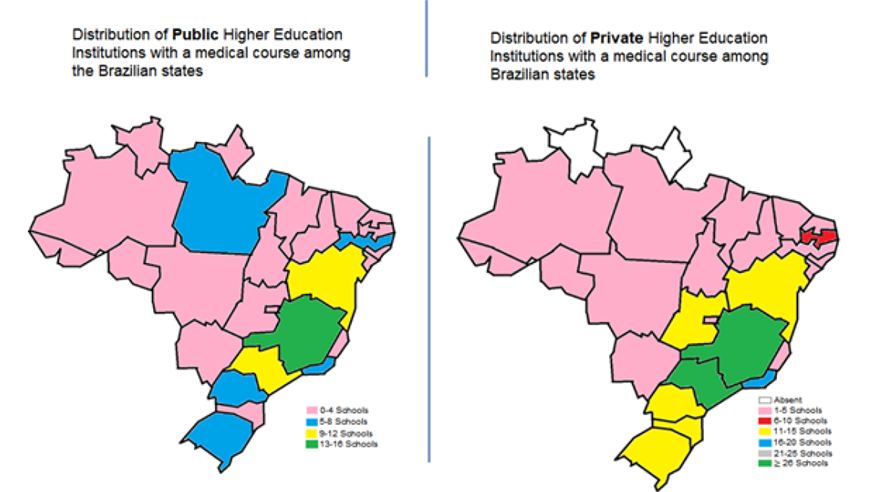
The 336 medical schools were then classified by state and region, and into the public and private categories (Table 1). The highest concentration of courses was observed in the Southeast region, followed by the Northeast region. When considering only the public institutions, the northeast region is the one that concentrates the highest number of schools, followed by the southeast region. When considering only the private institutions, the situation was the opposite. Figure 1 shows the distribution of medical school by Federation state.
Table 1 Distribution of medical courses, public X private, among the five regions of the country.
| Region | Public | Private | Total n (%) |
|---|---|---|---|
| South | 18 | 39 | 57 (16,7%) |
| Southeast | 30 | 111 | 141 (41,3%) |
| Midwest | 14 | 19 | 33 (9,7%) |
| Northeast | 41 | 43 | 84 (24,6%) |
| North | 12 | 14 | 26 (7,7%) |
| Total | 115 | 226 | 341 |
Source: Elaborated by the authors.
Source: Elaborated by the authors.
Figure 1 Distribution of public and private Higher Education Institutions with medical courses among the Brazilian states.
We analyzed the total number of vacancies offered in the country. In 2021, there was a total of 37,209 vacancies offered in medical courses that had already started. The distribution by state and region is shown in Table 2.
Table 2 Distribution of vacancies offered in public and private medical courses among the five regions of the country.
| Public | Private | Total n (%) | |
|---|---|---|---|
| South | 1.438 | 4.022 | 5.460 (14,7%) |
| PR | 550 | 1.619 | |
| RS | 688 | 1.175 | |
| SC | 200 | 1.228 | |
| Southeast | 3.095 | 13.822 | 16.917 (45,5%) |
| ES | 80 | 798 | |
| MG | 1.405 | 3.437 | |
| RJ | 694 | 2.411 | |
| SP | 916 | 7.176 | |
| Midwest | 908 | 2.243 | 3.151 (8,4%) |
| DF | 156 | 470 | |
| GO | 244 | 1.462 | |
| MS | 268 | 120 | |
| MT | 240 | 191 | |
| Northeast | 3.074 | 5.792 | 8.866 (23,8%) |
| AL | 210 | 285 | |
| BA | 694 | 1.792 | |
| CE | 400 | 743 | |
| MA | 410 | 299 | |
| PB | 250 | 817 | |
| PE | 510 | 980 | |
| PI | 240 | 361 | |
| RN | 280 | 305 | |
| SE | 160 | 210 | |
| North | 972 | 1.843 | 2.815 (7,6%) |
| AC | 80 | 81 | |
| AM | 242 | 295 | |
| AP | 60 | 0 | |
| PA | 370 | 540 | |
| North | 972 | 1.843 | 2.815 (7,6%) |
| RO | 40 | 487 | |
| RR | 80 | 0 | |
| TO | 100 | 440 |
Legend: AC = Acre; AL = Alagoas; AP = Amapá; AM = Amazonas; BA = Bahia; CE = Ceará; DF = Distrito Federal; ES = Espírito Santo; GO = Goiás; MA = Maranhão; MT = Mato Grosso; MS = Mato Grosso do Sul; MG = Minas Gerais; PA = Pará; PB = Paraíba; PR = Paraná; PE = Pernambuco; PI = Piauí; RJ = Rio de Janeiro; RN = Rio Grande do Norte; RS = Rio Grande do Sul; RO = Rondônia; RR = Roraima; SC = Santa Catarina; SP = São Paulo; SE = Sergipe; TO = Tocantins.
Source: Elaborated by the authors.
After carrying out all the steps to search for the documents, we obtained the PCP of 134 schools, or 40% of the total number of institutions. Of these, 95 were from public schools, representing 83% in their category and 39 from private schools, 17% in their category. (Figure 2).
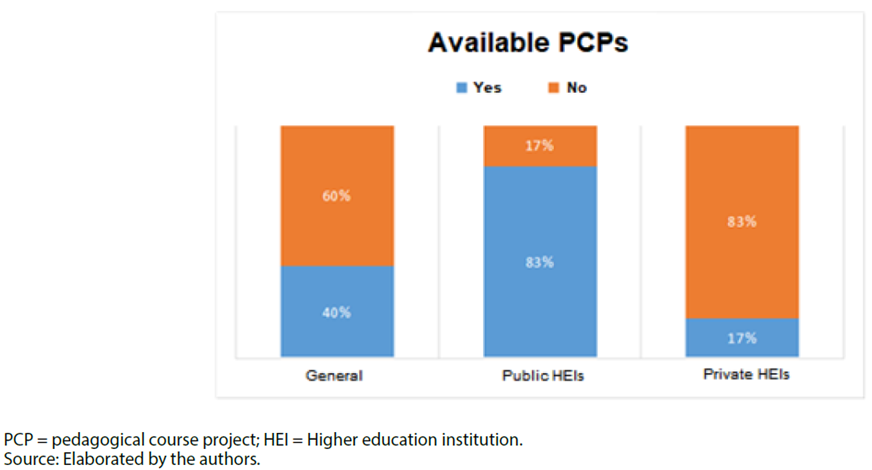
Figure 2 Percentage of pedagogical projects for medical courses provided by public and private higher education institutions in Brazil after a systematic survey.
All coordinators were contacted, regardless of the availability of the PCP on the institution's website and, therefore, we received 26 PCPs, of which 15 were not available on the institution's website.
Thus, of the obtained PCPs, 129 (96.3%) were obtained from the institution's website and 15 (3.7%) were obtained from the course coordinator through direct contact. Table 3 shows the percentage of PCPs available from public and private schools.
Having the 2014 DCNs as reference, we observed that 81% of the schools' PCPs were created after 2014, 13% before 2014 and in 3% of them the date of creation was not available.
Table 3 Percentage of available pedagogical course projects of medical schools, by state of the federation and region of Brazil.
| Public | Private | Total n (%) | |
|---|---|---|---|
| South | 15 (83%) | 9 (23%) | 24 (17.9%) |
| PR | 5 (63%) | 0 (0%) | |
| RS | 7 (100%) | 4 (31%) | |
| SC | 3 (100%) | 5 (36%) | |
| Southeast | 25 (83%) | 14 (13%) | 39 (29.1%) |
| ES | 1 (100%) | 0 (0%) | |
| MG | 15 (100%) | 4 (13%) | |
| RJ | 3 (60%) | 2 (14%) | |
| SP | 6 (67%) | 8 (14%) | |
| Midwest | 13 (93%) | 5 (26%) | 18 (13.5%) |
| DF | 2 (100%) | 1 (25%) | |
| GO | 3 (75%) | 3 (25%) | |
| MS | 4 (100%) | 0 (0%) | |
| MT | 4 (100%) | 1 (50%) | |
| Northeast | 33 (80%) | 8 (18%) | 41 (30.6%) |
| AL | 3 (100%) | 1 (50%) | |
| BA | 11 (100%) | 3 (20%) | |
| CE | 3 (75%) | 1 (20%) | |
| MA | 3 (75%) | 0 (0%) | |
| PB | 2 (67%) | 0 (0%) | |
| PE | 5 (83%) | 1 (20%) | |
| PI | 2 (50%) | 1 (33%) | |
| RN | 3 (75%) | 1 (50%) | |
| SE | 1 (50%) | 0 (0%) | |
| North | 9 (75%) | 3 (21%) | 12 (8.9%) |
| AC | 1 (100%) | 0 (0%) | |
| AM | 1 (50%) | 0 (0%) | |
| AP | 1 (100%) | -- | |
| PA | 4 (80%) | 1 (25%) | |
| RO | 1 (100%) | 0 (0%) | |
| RR | 0 (0%) | -- | |
| TO | 1 (100%) | 2 (100%) |
Legend: AC = Acre; AL = Alagoas; AP = Amapá; AM = Amazonas; BA = Bahia; CE = Ceará; DF = Distrito Federal; ES = Espírito Santo; GO = Goiás; MA = Maranhão; MT = Mato Grosso; MS = Mato Grosso do Sul; MG = Minas Gerais; PA = Pará; PB = Paraíba; PR = Paraná; PE = Pernambuco; PI = Piauí; RJ = Rio de Janeiro; RN = Rio Grande do Norte; RS = Rio Grande do Sul; RO = Rondônia; RR = Roraima; SC = Santa Catarina; SP = São Paulo; SE = Sergipe; TO = Tocantins.
Source: Elaborated by the authors.
DISCUSSION
Initially, we were able to confirm the observation made by previous studies regarding the regions where medical courses are concentrated. It was verified that the courses were concentrated in the southeast and northeast regions, as demonstrated by Santos Junior et al. in 201810. Another survey carried out in 2018 demonstrated that capital cities in the southeast region had more vacancies in medical schools (4,537) than entire regions, such as the North (2,469) and the Midwest (2,663) and, together, these two regions had fewer medical schools than the entire state of São Paulo1. The distribution and permanence of physicians among the regions is influenced by the distribution of medical schools, but the increase in vacancies in the most underserved regions does not directly guarantee the permanence of physicians in the region1.
Medical education has been concentrated in large urban centers, with most courses held in tertiary or quaternary institutions. This medical training model failed to adequately meet the needs of the population in smaller cities and communities11. Placing students in decentralized locations requires effort and resources by the government, the educational institution, the health services, the training site, the community in which the students are located, the physicians who are responsible for the training, and even the presence of multidisciplinary teams on site. (12 In a recent literature review, it was identified that the experience of preceptors and teachers, particularly in Primary Health Care, Family Medicine and Rural Medicine, as well as the local infrastructure, were also determinant factors13. Thus, all these are possible strategies to support the permanence of general practitioners in the most remote regions14),(15.
The number of private schools was higher than the number of public ones in all regions, and the same occurred with the number of vacancies. According to information on the federal government’s “Mais Médicos” program website, during the first two years of the program, a total of 5,300 new undergraduate vacancies were created, 1,700 of which in public universities and 3,600 in private institutions in all regions of the country16. The number of vacancies in private medical schools increased from 3.2% until 1962 to 15.1% in the early 2000s, reaching 45.7% in 2018, corresponding, at the time, to 65.8% of all vacancies in the country1. Over time, an increase in the ratio between the number of private/public vacancies was observed, reaching 9.1 between the years 2003 and 20101. In the present study, we found a ratio of private/public vacancies of 3.4 in 2021.
According to the DCNs, the undergraduate medical course must have a collectively constructed pedagogical project, centered on the student as the subject of learning and supported by the teacher as a facilitator and mediator of the teaching-learning process17. This pedagogical project should seek the full and adequate training of the student through the articulation between teaching, research and extension/assistance. Regardless of the PCP and the ongoing pedagogical practices, there is a legal demand to follow the DCN18 recommendations. In this scenario, with new medical courses emerging, and vacancies being expanded, an easy access to the PCP would encourage the analysis and study of how medical courses have been adapting, seeking pathways grounded on the culture of each institution and different regional realities, adopting critical, innovative proposals, as reflected by its community18.
From this perspective, we consider the 40% return rate of PCPs across the country to be a matter of concern, largely as a result of the low success rate regarding the acquisition of private HEI projects, where only 17% were obtained, versus 83% of public HEIs. This is aggravated by the fact that, although the provision of pedagogical information on the websites of the HEIs is an obligation established by the Law of Guidelines and Bases of National Education, this demand has not been met19. Moreover, access to this document should be facilitated.
Studies that aim to determine how specific contents are taught, the curricular design, the pedagogical plan and its compliance with the current DCNs, describe the lack of access as a limiting factor20)-(22. The present study confirms this fact, due to the low return rate of contact with course coordinators, suggesting a lack of engagement with studies that gather information on how medical teaching has been practiced in Brazil. This contrasts with what is already the norm and well defined in several countries worldwide. This is curriculum mapping, a process that designs a multidimensional model of an educational program so that a complete, more transparent and better integrated learning experience can take place23. Hence, many universities around the world are building or expanding their technical infrastructure to manage their curricula23. As these documents become accessible, studies with assessments and learning between schools in different locations, including different countries, can be developed24.
During the search for the documents, the insistent call for new students to enroll through various advertisements on the institutional website was evident, which was often followed by the sending of advertisement mail for enrollment in the entrance exam of that institution, offering amenities regarding the admission and payment of fees.
In line with this aspect, funding policies were offered, most of them involving public money, through student loan programs, among which the Educational Credit Program, the Higher Education Student Financing Fund (Fies) and ProUni1 stand out.
Finally, the documents made available by the institutions are expected to be aligned with the 2014 DCNs, given that more than 80% of them were written or updated after that date. Alignment with the DCNs is one of the outstanding items in the evaluation process of courses in Brazil, supported by instruments required by the National Institute of Evaluation18, and should be seen as work instructions bearing in mind the construction of projects aimed at medical education committed to the changes required by society. Studies have already described the difficulty in updating pedagogical projects, considering the new guidelines and mention financial, administrative and political obstacles as factors that can prevent or make the implementation of these changes and the alignments between the PCP and the DCNs unfeasible25.
The study has the limitation of not having made telephone contact between the study stages; however, we used a methodology that allowed reaching 100% of the course coordinators and the results showed the need to improve how these documents can be more easily made available.
Another aspect is related to the fact that, despite the requirement that there be a PCP for the formatting of the courses, unfortunately, one cannot guarantee that the defined content will, in fact, be necessarily addressed. In addition, contents present in the “occult curriculum” can contribute to the student’s training, even if it is not explicitly part of the PCP. Finally, given that this is a new topic related to the training of health professionals, the eventual lack of specific training in PC, for teachers and preceptors of medical courses, can negatively influence the actual fulfillment of the pedagogical objectives proposed for this topic.
We expect that the results produced by this study can contribute to the demographic knowledge of medical courses and the awareness regarding the importance of the availability of mandatory and indispensable documents for the knowledge of the courses.
CONCLUSION
The study allowed identifying the distribution of undergraduate medical courses and vacancies in the five regions of the country. The current distribution is in line with the findings of recent studies, showing the persistence of the trend towards the concentration of courses in the southeast and northeast regions of the country.
Additionally, it was observed that, although mandatory, the availability of the PCP is not a reality. This is particularly more evident in private higher education institutions, in which the engagement in feedback by those in charge of these documents, who were contacted, was insufficient to meet this demand.
REFERENCES
1. de Oliveira BLCA, Lima SF, Pereira MUL, Pereira Júnior GA. Evolução, distribuição e expansão dos cursos de Medicina no Brasil (1808-2018). Trab Educ Saúde. 2019;17(1):1-20 [acesso em 20 jul 2022. Disponível em: Disponível em: http://www.scielo.br/j/tes/a/SGBd4Hbk5ghWD3yg6vqt3Jk/abstract/?lang=pt . [ Links ]
2. Brasil. Lei nº 13.005, de 25 de junho de 2014. Aprova o Plano Nacional de Educação - PNE e dá outras providências. Diário Oficial da União; 2014 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.planalto.gov.br/ccivil_03/_ato2011-2014/2014/lei/l13005.htm . [ Links ]
3. de Oliveira FP, Santos LMP, Shimizu HE. Programa Mais Médicos e Diretrizes Curriculares Nacionais: avanços e fortalecimento do sistema de saúde. Trab Educ Saúde . 2019;17(1):1-19 [acesso em 26 jun 2022]. Disponível em: Disponível em: http://old.scielo.br/scielo.php?script=sci_arttext&pid=S1981-77462019000100514&lng=en&nrm=iso&tlng=pt . [ Links ]
4. Brasil. Lei nº 12.871, de 22 de outubro de 2013. Institui o Programa Mais Médicos, altera as Leis nº 8.745, de 9 de dezembro de 1993, e nº 6.932, de 7 de julho de 1981, e dá outras providências. Diário Oficial da União ; 2013 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.planalto.gov.br/ccivil_03/_ato2011-2014/2013/lei/l12871.htm . [ Links ]
5. Brasil. Programa Mais Médico: o novo currículo. [acesso em 20 jul 2022]. Disponível em: Disponível em: http://maismedicos.gov.br/o-novo-curriculo . [ Links ]
6. da Silva ATC, de Medeiros Junior ME, Fontão PN, Saletti Filho HC, Vital Junior PF, Bourget MMM, et al. Medicina de família do primeiro ao sexto ano da graduação médica: considerações sobre uma proposta educacional de integração curricular escola-serviço. Rev Bras Educ Med. 2017;41(2):336-45 [acesso em 26 jun 2022]. Disponível em: Disponível em: http://www.scielo.br/j/rbem/a/5w46RcDZs9Pf7jhy976LKgf/abstract/?lang=pt . [ Links ]
7. Lampert JB. Dois séculos de escolas médicas no Brasil e a avaliação do ensino médico no panorama atual e perspectivas. Gazeta Médica da Bahia. 2008;78(1):31-37 [acesso em 20 de jul 2022]. Disponível em: Disponível em: http://www.gmbahia.ufba.br/index.php/gmbahia/article/view/255 . [ Links ]
8. Machado C, de Oliveira JM, Malvezzi E. Repercussões das Diretrizes Curriculares Nacionais de 2014 nos projetos pedagógicos das novas escolas médicas. Interface (Botucatu). 2021;25(1):1-15 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.scielo.br/j/icse/a/V3H87bcLY94p5dMFXPqQFKd/abstract/?lang=pt . [ Links ]
9. Ministério da Educação. e-MEC [acesso em 20 de jul 2022]. Disponível em: Disponível em: https://emec.mec.gov.br/ . [ Links ]
10. dos Santos Júnior CJ, Misael JR, Trindade Filho EM, Wyszomirska RMAF, dos Santos AA, de Souza Costa PJM. Expansão de vagas e qualidade dos cursos de Medicina no Brasil: “Em que pé estamos?”. Rev Bras Educ Med . 2021;45(2):1-10 [acesso em 26 jun 2022]. Disponível em: Disponível em: http://www.scielo.br/j/rbem/a/Z6NNNN7t6q9Wr7Zv3HbJBLL/?lang=pt . [ Links ]
11. Burrows AM, Laupland KB. Comprehensiveness of distributed medical education systems: a regional population-based perspective. BMC Med Educ. 2021;21(1):1-7 [acesso em 26 jun 2022]. Disponível em: Disponível em: https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-020-02466-x . [ Links ]
12. de Villiers M, van Schalkwyk S, Blitz J, Couper I, Moodley K, Talib Z, et al. Decentralised training for medical students: a scoping review. BMC Med Educ . 2017;17(196)1-13. doi: https://doi.org/10.1186/s12909-017-1050-9. [ Links ]
13. Maria E, Rocha S, Boiteux PDA, Dantas G, Iii A, Gomes CE, et al. Preditores educacionais para fixação de médicos em áreas remotas e desassistidas: uma revisão narrativa. Rev Bras Educ Med . 2020;44(1):1-8 [acesso em 26 jul 2022]. Disponível em: Disponível em: http://www.scielo.br/j/rbem/a/Z7J6wW9W78hHkdTZkbQ7Bkk/?lang=pt . [ Links ]
14. Clark TR, Freedman SB, Croft AJ, Dalton HE, Luscombe GM, Brown AM, et al. Medical graduates becoming rural doctors: rural background versus extended rural placement. Med J Aust. 2013;199(11):779-82 [acesso em 20 jul 2022]. Disponível em: Disponível em: https://www.mja.com.au/journal/2013/199/11/medical-graduates-becoming-rural-doctors-rural-background-versus-extended-rural . [ Links ]
15. Chevillard G, Mousques J, Lucas-Gabrielli V, Rican S. Has the diffusion of primary care teams in France improved attraction and retention of general practitioners in rural areas? Health Policy. 2019;123(5):508-515 [acesso em 20 jul 2022]. Disponível em: Disponível em: https://www.sciencedirect.com/science/article/abs/pii/S016885101930048X?via%3Dihub [ Links ]
16. Brasil. Programa Mais Médico: graduação em Medicina [acesso em 20 jul 2022]. Disponível em: Disponível em: http://maismedicos.gov.br/cursos-de-graduacao . [ Links ]
17. Brasil. Resolução CNE/CES nº 4, de 7 de novembro de 2001. Institui Diretrizes Curriculares Nacionais do curso de graduação em Medicina. Diário Oficial da União ; 9 nov 2001. Seção 1, p. 38 [acesso em 28 jun 2022]. Disponível em: Disponível em: http://portal.mec.gov.br/cne/arquivos/pdf/CES04.pdf . [ Links ]
18. de Oliveira CA, Senger MH, Ezequiel OS, Amaral E. Alinhamento de diferentes projetos pedagógicos de cursos de Medicina com as Diretrizes Curriculares Nacionais. Rev Bras Educ Med . 2019;43:143-51 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.scielo.br/j/rbem/a/8gdDCgXCvRcgcdDM69XSxNd/abstract/?lang=pt . [ Links ]
19. Brasil. Lei nº 9.394, de 20 de dezembro de 1996. Estabelece as Diretrizes e Bases da Educação Nacional. Diário Oficial da União , 1996 [cited 2022 Jul 20]. Disponível em: Disponível em: http://www.planalto.gov.br/ccivil_03/LEIS/L9394.htm . [ Links ]
20. Vianna A, Feliz M, Schwanke C. Ensino de geriatria nas faculdades de Medicina brasileiras. Geriatria & Gerontologia. 2010;4:179-85. [ Links ]
21. Pereira GAM, dos Santos AMPV, Lopes PTC. O ensino da radiologia: uma análise dos currículos da área da saúde de instituições de ensino superior na Região Sul do Brasil. Rev Bras Educ Med . 2017;41:251-9 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.scielo.br/j/rbem/a/JVfkwvCDZzGBffQMntJrZGn/?lang=pt&format=html . [ Links ]
22. de Almeida MJ, de Campos JJB, Turini B, Nicoletto SCS, Pereira LA, Rezende LR, et al. Implantação das Diretrizes Curriculares Nacionais na graduação em Medicina no Paraná. Rev Bras Educ Med . 2007;31:156-65 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.scielo.br/j/rbem/a/y8TgnhJvtCyYcVTVB4MLRvn/abstract/?lang=pt . [ Links ]
23. Al-Eyd G, Achike F, Agarwal M, Atamna H, Atapattu DN, Castro L, et al. Curriculum mapping as a tool to facilitate curriculum development: a new school of medicine experience. BMC Med Educ . 2018;18(185):1-8 [acesso em 28 jun 2022]. Disponível em: Disponível em: https://pubmed.ncbi.nlm.nih.gov/30081897/ . [ Links ]
24. Baozhi S, Yuhong Z. Medical curricula in China and the USA: a comparative study. Med Teac. 2003;25(4):422-7 [acesso em 20 jul 2022]. Disponível em: Disponível em: http://www.tandfonline.com/doi/full/10.1080/0142159031000136725 . [ Links ]
25. de Oliveira CA, Amaral EM, Cyrino EG, Gianini RJ. Encontros e desencontros entre projetos pedagógicos de cursos de Medicina e Diretrizes Curriculares Nacionais: percepções de professores. Interface Comun Saúde Educ. 2021;25:1-15 [acesso em 28 jun 2022]. Disponível em: Disponível em: http://www.scielo.br/j/icse/a/MCkxrgP8zBMkFYpYRs7LRBB/?lang=pt . [ Links ]
Received: July 21, 2022; Accepted: November 11, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
