










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format
 Send this article by e-mail
Send this article by e-mailShare

 Permalink
PermalinkRevista Brasileira de Educação Médica
Print version ISSN 0100-5502On-line version ISSN 1981-5271
Rev. Bras. Educ. Med. vol.47 no.1 Rio de Janeiro Jan./Mar. 2023 Epub Mar 17, 2023
https://doi.org/10.1590/1981-5271v47.1-20220021
ORIGINAL ARTICLE
Meditation for stress and anxiety relief in undergraduate students: a randomized clinical trial
1
, All authors actively contributed to the study design, data collection and analysis, review and approval of the final version of the manuscript http://orcid.org/0000-0001-8774-6339
http://orcid.org/0000-0001-8774-6339
1
, All authors actively contributed to the study design, data collection and analysis, review and approval of the final version of the manuscripthttp://orcid.org/0000-0003-4590-5025
1
, All authors actively contributed to the study design, data collection and analysis, review and approval of the final version of the manuscripthttp://orcid.org/0000-0003-0128-591X
1Centro Universitário Cesmac, Maceió, Alagoas, Brazil.
Introduction:
Stress is a state in which the body homeostasis is threatened, leading to adaptive, physiological and behavioral responses. Anxiety is an unpleasant feeling that occurs whenever a future potential threat is perceived. Whenever these states are prolonged, both lead to metabolic, cardiovascular, neuropsychiatric and immunological consequences. University students are more susceptible to stress and anxiety symptoms than the general population. Mindfulness is a technique that allows its practitioners to become more aware of their emotions, dealing with stress in a more skilled way.
Objective:
To; evaluate the efficacy of a modified mindfulness program in reducing stress and anxiety symptoms in medicine and dentistry undergraduate students.
Methods:
This was a single blinded, randomized, clinical trial. Students from the aforementioned courses enrolled in the 1st to the 8th semesters of a higher education institution, answered Lipp’s Inventory of Stress symptoms for Adults (ISSL) (n=418) and the State-Trace Anxiety Inventory (STAI) (n=369). Those who showed a positive score for symptoms of stress and/or anxiety and accepted to take part in the intervention (n=59), were randomized into one of the two groups - mindfulness (a 2-week modified program), or control. After the intervention, the students were asked to answer the STAI and ISSL tools once again.
Results:
The global prevalence of stress and anxiety symptoms were 67% (n=280) and 76.4% (n=282), respectively. At the end of the second week, symptoms of stress and anxiety decreased 30.8% and 22.2%, respectively. There were no statistically significant differences between the mindfulness and control groups (p>0.05).
Conclusion:
Symptoms of stress and anxiety are highly prevalent among the studied population. Among medicine and dentistry undergraduate students in this higher education institution, a shortened mindfulness program was unable to reduce symptoms of stress and anxiety in a statistically significant way when compared to a control group.
Keywords: Psychological Stress; Anxiety; Mindfulness
Introdução:
O estresse é um estado no qual ocorrem ameaças à homeostase do organismo, com respostas adaptativas fisiológicas e comportamentais. A ansiedade é uma sensação desagradável advinda da percepção de uma ameaça potencial futura. Quando prolongados, ambos levam a repercussões metabólicas, cardiovasculares, imunológicas e neuropsiquiátricas. Os estudantes universitários são mais susceptíveis a sintomas de estresse e ansiedade do que a população em geral. A técnica de mindfulness permite que os seus praticantes se tornem mais conscientes de suas emoções, passando a responder de forma habilidosa ao estresse e à ansiedade
Objetivo:
Este estudo teve como objetivo avaliar a eficácia de um programa de mindfulness na redução de sintomas de estresse e ansiedade em estudantes de Medicina e Odontologia.
Método:
Trata-se de um ensaio clínico, randomizado, simples-cego. Acadêmicos regularmente matriculados do primeiro ao oitavo período desses cursos de uma instituição de ensino superior responderam ao Inventário de Sintomas de Stress para Adultos de Lipp (ISSL) (n = 418) e ao Inventário de Ansiedade Traço-Estado (IDATE) (n = 369). Os participantes que apresentaram sintomas de estresse e/ou ansiedade e aceitaram participar da intervenção (n = 59) foram randomizados em grupos mindfulness (programa modificado de duas semanas) e de controle. Ao final da intervenção, o ISSL e o IDATE foram reaplicados.
Resultado:
As prevalências globais de estresse e ansiedade foram de 67% (n = 280) e 76,4% (n = 282), respectivamente. Ao final da segunda semana, a redução dos sintomas de estresse e ansiedade foi de 30,8% e 22,2%, respectivamente. Não houve diferença estatisticamente significativa entre os grupos mindfulness e de controle (p > 0,05).
Conclusão:
Percebe-se uma alta prevalência de sintomas de estresse e ansiedade na população estudada. Um programa de mindfulness em formato reduzido não foi capaz de diminuir significativamente os sintomas de estresse e ansiedade em comparação ao grupo de controle, em acadêmicos de Medicina e Odontologia dessa instituição.
Palavras-chave: Estresse Emocional; Ansiedade; Atenção Plena
INTRODUCTION
Stress can be defined as a state in which threats to the body homeostasis occur, generating physiological and behavioral adaptive responses that result in functional alterations of several areas of the Central Nervous System (CNS), organs and tissues1. Prolonged exposure to stress-triggering factors causes functional and structural changes in the CNS, (mainly in the limbic system), in the Autonomic Nervous System and in the hypothalamic-pituitary-adrenal axis, with a consequent exaggerated release of catecholamines, glucocorticoids, and pro-inflammatory cytokines, which will be the final mediators of several metabolic, cardiovascular, immunological and neuropsychiatric disorders1)-(4.
Anxiety, on the other hand, is defined as an unpleasant, temporary, generalized feeling, which arises from the perception of a potential threat, whose probability of happening is low or uncertain5),(6. Anxiety can be subdivided into state-anxiety and trait-anxiety. The first occurs acutely due to a possible threat; the second indicates an individual’s personality trait, whose tendency is to respond anxiously to adversities5.
University students are more susceptible to stress and anxiety symptoms than the overall population7. Health students in high-demand courses, such as medicine and dentistry, are more susceptible to symptoms of stress and anxiety8),(9, with prevalence rates ranging from less than 50%10 to more than 70% of stressed and/or anxious students8. Factors associated with high rates of stress and anxiety during undergraduate school are: first years of the course9, female gender, low family income, dissatisfaction with the course10, negative thinking, dissatisfaction with the study environment11 and lack of emotional support from the institution12. Therefore, measures to reduce stress and anxiety in the teaching environment should be implemented at the beginning of academic life9),(13.
One of the measures used to reduce stress and anxiety is mindfulness, defined as a meditation technique that allows greater awareness of emotions, allowing practitioners to respond to stressors in a more skilled manner14),(15. It has a neuroplastic action on CNS structures related to attention (prefrontal cortex, anterior cingulate cortex and striatum), emotional regulation and self-awareness (insula, amygdala, PFC and anterior cingulate cortex)16)-(18, as well as a regulatory action on biochemical stress markers, such as serum cortisol, C-reactive protein (CRP) and alpha tumor necrosis factor (TNF-α)19.
Classic mindfulness programs lasting eight weeks have identified adherence difficulties for students of courses with an intense academic load20),(21. In this sense, attempts to adapt mindfulness programs to the reality of each institution, to achieve greater adherence, use and effectiveness of this technique have been increasingly described in the literature16),(21),(22.
Based on the above, this study aimed to evaluate the effectiveness of a modified mindfulness program in reducing symptoms of stress and anxiety in students of from the Medicine and Dentistry courses. To date, in Brazil, there have been no studies published in ith national or international journals that used the approach proposed by the authors of this study.
METHODS
Study design and location
This is a randomized, single-blind, parallel clinical trial, carried out in a Higher Education Institution (HEI), located in the northeast of Brazil, which consisted of three phases: (1) application of stress and anxiety questionnaires; (2) randomization of participants into two groups (mindfulness and control); and performance of the intervention and; (3) Reapplication of phase 1 questionnaires.
The study was approved by the Research Ethics Committee (REC) under approval number 3.762.414 and was carried out in accordance with the items of the Consolidated Standards of Reporting Trials - CONSORT 201023.
Data collection instruments
Lipp’s Inventory of Stress symptoms for Adults (ISSL) evaluates the presence of stress in the individual, indicating at which stage of stress the individual is: alertness, resistance, near exhaustion or exhaustion. The inventory is divided into 3 charts with psychological or physical manifestations in the last 24 hours (15 items); in the last week (23 items); and in the last month (15 items). The first chart is related to the alertness phase; the second with the resistance and near-exhaustion phases; and the third chart evaluates the exhaustion phase. The presence of stress is considered when the individual ticks 6 items in the first step; or 3 items in the second step; or 8 items in the third step. The diagnosis of the stress phase is made by applying the formulas and tables available in its application manual24.
The State-Trait Anxiety Inventory (STAI) has two distinct scales that are used to identify trait and state anxiety. Trait anxiety is related to the individual’s personality, and the state anxiety with a transient character of the feeling of anxiety. Each scale consists of 20 questions, of which answers must be scored from 1 to 4, where: 1 = almost never; 2 = sometimes; 3 = frequently; and 4 = almost always. According to the manual, some items have their scores inverted to calculate the final score, since they have the opposite response direction. The sum of the scores obtained for each answer can vary from 20 to 80 points, with 20 to 40 points meaning a low level of anxiety; 41 to 60 points n average level of anxiety; and 60 to 80 points a high level of anxiety25. In this study, we considered that a score of 41 points or more indicated that the participant had clinical symptoms of anxiety26.
Additionally, the authors developed a personal and sociodemographic data sheet that assesses data such as marital status, ethnicity, type of housing, psychological or psychiatric treatment, previous exposure to a violent episode and social class.
Sample and eligibility criteria
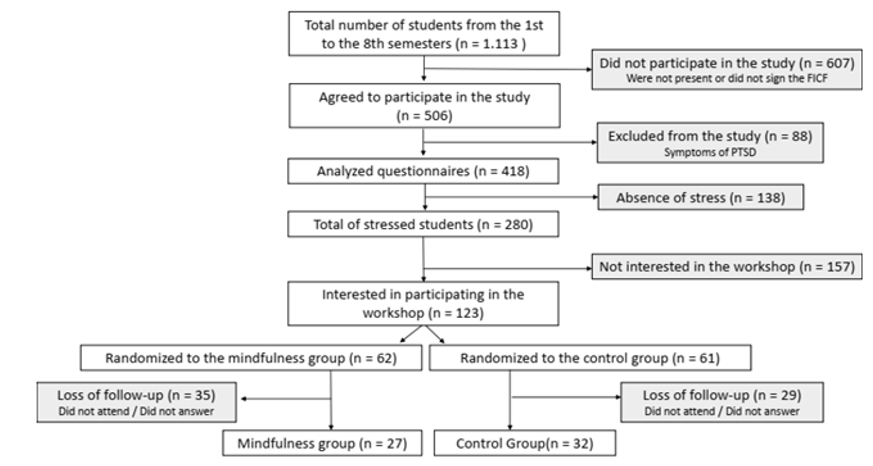
For phase 1 of the study, all 1,113 students from the 1st to the 8th years regularly enrolled in the medicine and dentistry courses at an HEI, aged 18 years or older, of both genders, were invited to participate. Of these, 506 agreed to participate in the study. Those who attended more than one undergraduate course simultaneously were excluded; who were not present on the day of data collection; who had been diagnosed with or were being treated for psychotic or dissociative disorders; and those who had been directly exposed to an emotionally traumatic event, such as serious accidents, physical or sexual violence and/or death threats in the previous year, which were considered as likely to develop signs of post-traumatic stress disorder (PTSD).
For phases 2 and 3, the sample consisted of 123 medicine and dentistry students, randomly selected and who agreed to participate in the mindfulness program. All students selected for phases 2 and 3 had symptoms of stress, which did not happen with anxiety. The exclusion criteria comprised the same as in phase 1, plus not attending the scheduled weekly meetings.
Procedures
In September 2019, the researcher informed the participants about the importance and nature of the research by reading the Free and Informed Consent Form (FICF). Consent was given by 506 participants, who were asked to answer the ISSL and STAI questionnaires in the classroom. To test the logistics of applying the instruments and the understanding of the individuals answering them, a team from the Psychology course and another from the Medicine course carried out a previous application with a pilot sample (n=18), which corresponds to 4.3% of the total sample of this study (n=418).
In the second phase, 123 participants who accepted the invitation were randomized into two groups: mindfulness and control groups. For the randomization process, the Microsoft Excel® program was used: the participants were listed in a spreadsheet, and random numbers were assigned to each participant to avoid identifying them. Then, the participants were randomized between the two groups. The sample distribution flow is shown in figure 1.
To obtain the sample design, the statistical calculation program GPower was used, with the following parameters: significance level with p<0.05, test power of 95%, and effect size of 0.4, obtaining a total sample of 57 participants. The authors chose to allocate a larger number of participants per group to prevent the loss of follow-up bias.
The mindfulness group participated in one weekly meeting for two weeks, in the workshop format, which lasted three hours per meeting. Each session was supervised by a facilitator with experience in the method. The first session consisted of a didactic moment on the neurophysiological effects of stress, the history of mindfulness and the different ways of applying the technique in stress control and mental health development. The discussions were intermingled with four moments of mindfulness meditation for 10 to 15 minutes, while maintaining attention on breathing and body sensations. The second session consisted of discussions on the difficulties in maintaining the practice of mindfulness throughout the week and how to overcome these barriers; followed by a class on the influence of positive mental attitudes (forgiveness, empathy and compassion) on the human body and how to associate them with the practice of mindfulness, interspersed with four moments of mindfulness meditation for 10 to 15 minutes. The participants were instructed to maintain the meditation practice for 12 minutes daily at home, guided by audio files, and were also instructed to record it in the meditation practice diary.
After the intervention period, the ISSL and STAI were reapplied in both groups by an interviewer blinded to the allocation of participants, and their scores were compared with pre-intervention levels. At the end of the study, the meditation program was also offered to the control group. The IBM SPSS Statistics® software, version 25.0.0.0, was used for the statistical analysis. In phase 1, the descriptive analysis was performed and in phase 2, inferential statistics were carried out between the mindfulness and control groups, using the Chi-square test, McNemar test and t test for independent samples, with a significance level of 5%.
RESULTS
A Mindfulness program was selected to be used with university students because it is a scientifically proven intervention in reducing stress and anxiety symptoms, with improvement in biochemical markers19, attention, emotional regulation, as well as self-awareness 14)-(18. In this study, the overall prevalence of stress symptoms was 67% (n=280). The prevalence of stress per course was 66.7% (n=172) for medicine and 67.5% (n=108) for dentistry. No significant differences were observed between the courses (x2=0.31; p>0.05).
State and trait anxiety were present in 76.4% (n=282) of students in both courses. Dentistry students had a prevalence of trait anxiety of 86.7% (n=98); significantly higher (p< 0.05) than that of medical students, whose prevalence was 72.4% (n=184). The prevalence of state anxiety was 75.4% (n=86) for dentistry, and 76.4% (n=196) for medicine. There was no significant difference between the courses.
One hundred and twenty-three students with stress and/or anxiety accepted to participate in the intervention and were randomized between the mindfulness (n=62) and control (n=61) groups. Thirty-five participants in the mindfulness group and 29 in the control group were excluded for missing at least one of the workshop meetings. Therefore, the mildness group consisted of 26 participants with a mean age of 23.4 years (standard deviation 4.23); mostly female (70%); studying medicine (76%); single (84%); of brown ethnicity (38%); only studied (96%); lived with family members (53%), social class A (42%), and, finally, half (50%) of the participants had already undergone psychological or psychiatric treatment. The control group consisted of 31 participants with a mean age of 22.1 years (standard deviation 3.21); mostly female (87%); studying medicine (77%); single (100%); of brown ethnicity (41%); only studied (87%); lived with family members (54%); social class A (36%), and, finally, 48% of the participants had already undergone psychological or psychiatric treatment. After the intervention, participants from both groups who did not want to answer the questionnaires were excluded, and the statistical analysis in the pre- and post-workshop moments for the studied variables is depicted in Tables 1 and 2.
Table 1 Pre and post-workshop stress and anxiety prevalence in mindfulness group.
| Variables | Pre-workshop | Post-workshop | x2 | p | ||
|---|---|---|---|---|---|---|
| Sim n (%) | Não n (%) | Sim n (%) | Não n (%) | |||
| Stress (n=26) | 26(100) | 0 | 18(69.2) | 8(30.8) | 6.12 | 0.00* |
| Trait-anxiety (n=21) | 16(76.2) | 5(23.8) | 12(57.2) | 9(47.8) | 1.5 | 0.22 |
| State-anxiety (n=21) | 19(90.5) | 2(9.5) | 12(57.2) | 9(47.8) | 4.0 | 0.04* |
Source: the author.
Note: McNemar test (gl=1; *p< 0.05).(title)
Table 2 Pre and post-workshop stress and anxiety prevalence in control group.
| Variables | Pre-workshop | Post-workshop | x2 | p | ||
|---|---|---|---|---|---|---|
| Sim n (%) | Não n (%) | Sim n (%) | Não n (%) | |||
| Stress (n=31) | 31(100) | 0 | 19(61.3) | 12(38.7) | 10.08 | 0.00* |
| Trait-anxiety (n=28) | 19(67.9) | 9(32.1) | 17(60.7) | 11(39.3) | 0.16 | 0.68 |
| State-anxiety (n=28) | 20(71.5) | 8(28.5) | 18(64.3) | 10(35.7) | 0.1 | 0.75 |
Source: the author.
Note: McNemar test (gl=1; *p< 0.05).(title)
As both groups demonstrated a significant reduction in the percentage of students who had symptoms of stress, the chi-square test was used to assess the differences between the control group and the mindfulness group after the intervention. No significant differences were observed (x²=0.1; gl=1; p>0.72).
The mindfulness group demonstrated a significant reduction in state-anxiety between the beginning and the end of the experiment. The chi-square test showed that there were no statistically significant differences between the groups after the workshop (x2=0.04; p=0.83). There were no differences between the scores of the control and mindfulness groups after the workshop for the trait-anxiety, state-anxiety and stress variables (Table 3).
Table 3 Mean of post-workshop scores in the mindfulness and control groups.
| Means | t test | ||||
|---|---|---|---|---|---|
| Variables | Post-workshop Control | Post-workshop Mindfulness | t | p | 95%CI |
| State-anxiety | 45.79 | 45.70 | 0.03 | 0.973 | -5.43 | 5.62 |
| Trait-anxiety | 45.27 | 45.61 | -0.12 | 0.902 | -5.71 | 5.05 |
| Stress | 80.87 | 117.66 | -1.52 | 0.13 | -85.05 | 11.69 |
Source: the author.
Note: t test for independent samples (*p < 0.05)
The time of informal mindfulness practice (at home) could not be measured, as only two participants delivered the meditation practice diary, making any statistical analysis of this variable impossible.
DISCUSSION
Although the high prevalence of stress (67%) found by the authors represents a higher value than what is described in most of the current literature 9),(10),(27, some studies have described an even higher prevalence of stress8),(28. There is evidence that indicates a higher prevalence of stress among medicine in comparison with dentistry students 10),(29. In this study, no significant differences were found between the courses.
The association between stress and a negative impact on health results in ineffective coping strategies such as substance abuse, eating disorders and avoidance behaviors30. In students of health courses with high physical and emotional demand, such as Medicine and Dentistry, in addition to the aforementioned behaviors, stress is correlated with the worsening of academic performance31, thus creating a perpetual vicious cycle. In the long term, stress can contribute to the development of depression, anxiety and exhaustion32, affecting not only one’s health, but also the professional future.
After the intervention, the authors observed that 30.8% of the participants in the mindfulness group and 38.7% of participants in the control group did not show any scores for stress symptoms. The lack of statistical significance between the groups identified in this study differs from what is found in the literature for the studied population, since even with reduced formats, the mindfulness technique demonstrates significant results when compared with a passive control group or waiting list-type group33),(34.
A classic mindfulness training program takes place over eight weeks, with weekly meetings for formal practice of the technique, in addition to daily practices carried out at home (or in another environment of their choice) by the participants. Some authors suggest that a classic format could show a greater statistical difference between the groups34. However, in long-term studies, the average adherence can reach only 2.5 weeks22.
In the present study, a low adherence rate was observed for both the mindfulness (43.54%) and the control groups (54%). Even the participants who attended the formal sessions did not hand in the meditation practice diary, making it impossible to analyze the time spent in informal practice. Although loss of follow-up and low adherence are frequently reported problems in studies using mindfulness21),(35),(36, it is known that the frequency of daily practice is more important than the formal practice (in courses) for a beneficial effect of mindfulness36),(37. This fact had been predicted by the authors of this study, and measures to minimize this bias were taken, such as a reduced format of the course, carrying out the formal intervention right after classes, planning dates outside the test period, and daily reminders through social media to meditation practice.
Cultural differences may also have influenced the low adherence to mindfulness practice. As it is a meditation practice derived from eastern philosophies, the cultural shock with a population in northeastern Brazil may have contributed to the lack of participants’ engagement. In an American study, Macinko et al.38 concluded that people of Latin and African descent were the ones who least used meditation as a therapeutic method.
The reduction in state-anxiety in the mindfulness group between the pre- and post-workshop moments indicate a tendency that even a brief intervention in mindfulness may be able to attenuate the most acute effects of anxiety. The reduction of anxiety symptoms through mindfulness right after the intervention is in line with what has been reported by other studies34),(39. It is noteworthy that despite the randomization of participants, the Mindfulness Group (MG) was more anxious (state-anxiety) in the pre-intervention assessments, when compared to the Control Group (CG) (90.5% MG and 71.5% CG). It is believed that this fact may have impacted the intervention results, as there was a significant reduction in the state-anxiety levels in the MG (p=0.04) and a non-significant one in the CG (p=0.75). Therefore, we can assume that if the groups had been matched by state-anxiety level, the intervention result, specifically in the comparison of state-anxiety between the two groups, could have been different.
The absence of a significant effect for trait-anxiety (a personality characteristic) may be related to the duration of the intervention. A more extensive program may allow more time for participants to engage in the daily practice of the technique39)-(41. On the other hand, longer interventions can be seen as more of an obligation, becoming a burden, which results in more emotional suffering and lack of adherence to the research and the practice of mindfulness22),(40. However, it should be noted that since this is a personality trait assessment, there is also the assumption that the scores would not change.
The authors tried to quantify the daily practice of mindfulness by recording it in a meditation practice diary. However, less than 10% of the diaries were returned to the researchers, which prevented their analysis. A similar situation occurred in the study by Damião Neto et al.40, suggesting that sociocultural barriers may contribute to the difficulty related to mindfulness interventions in a population of Brazilian university students.
The present study has some limitations that must be mentioned. First, participants were evaluated only after the intervention, not after a longer period of follow-up. A more distant evaluation moment could allow more time for participants to develop a methodology of meditation practice at home, with better results. Second, there was probably a low level of engagement in daily practices, but it was not possible to quantify the informal practice period, since participants did not return the diary of meditation practices. Third, the data from the present study refer to only one educational institution in the northeast of Brazil, therefore requiring caution regarding generalizations. Fourth, as blinding is impossible in a study with mindfulness, it is impossible to know whether there was an exchange of information between the control and mindfulness groups, causing a contamination that may have influenced the results obtained herein. Fifth, psychotic or dissociative disorders and students likely to develop signs of PTSD, considered as exclusion factors from the study, were assessed through self-reporting. And, finally, we emphasize that STAI has an unfavorable opinion on Satepsi (https://satepsi.cfp.org.br/); however, Satepsi is a system for standardizing psychological tests for clinical use and not for use in scientific research.
CONCLUSION
A meditation program based on the mindfulness technique, lasting two weeks, was not able to significantly reduce the symptoms of stress and anxiety in medicine and dentistry students at a higher education institution in northeastern Brazil.
The high prevalence of stress and anxiety symptoms in the assessed population demonstrates the need for early actions capable of minimizing the health problems caused by these conditions. Due to the evident low level of engagement and possible cultural shocks, future studies should seek designs that allow greater adherence by the participants, with a consequent increase in the benefits that the technique brings. They should highlight the meditation practice records, as there is evidence that daily meditation practice lasting 10 to 20 minutes becomes more important than the workshops offered on the technique.
REFERENCES
1. Chrousos GP. Stress and disorders of the stress system. Nat Rev Endocrinol. 2009;5(7):374-81. [ Links ]
2. Daskalakis NP, Bagot RC, Parker KJ, Vinkers CH, Kloet ER de. The three-hit concept of vulnerability and resilience: toward understanding adaptation to early-life adversity outcome. Psychoneuroendocrinology. 2013 Sep;38(9):1858-73. [ Links ]
3. Lucassen PJ, Pruessner J, Sousa N, Almeida OFX, Van Dam AM, Rajkowska G, et al. Neuropathology of stress. Acta Neuropathol. 2014;127(1):109-35. [ Links ]
4. Godoy LD, Rossignoli MT, Delfino-Pereira P, Garcia-Cairasco N, Lima Umeoka EH de. A comprehensive overview on stress neurobiology: basic concepts and clinical implications. Front Behav Neurosci. 2018;12:1-23. [ Links ]
5. Takagi Y, Sakai Y, Abe Y, Nishida S, Harrison BJ, Martínez-Zalacaín I, et al. A common brain network among state, trait, and pathological anxiety from whole-brain functional connectivity. Neuroimage. 2018 May;172:506-16. [ Links ]
6. Daviu N, Bruchas MR, Moghaddam B, Sandi C, Beyeler A. Neurobiological links between stress and anxiety. Neurobiol Stress. 2019 Nov;11:100191. [ Links ]
7. Lovell GP, Nash K, Sharman R, Lane BR. A cross-sectional investigation of depressive, anxiety, and stress symptoms and health-behavior participation in Australian university students. Nurs Heal Sci. 2015;17(1):134-42. [ Links ]
8. Aboalshamat K, Hou X-Y, Strodl E. Psychological well-being status among medical and dental students in Makkah, Saudi Arabia: a cross-sectional study. Med Teach. 2015;37(Supp 1):S75-81. [ Links ]
9. Bassols AMS, Carneiro BB, Guimarães GC, Okabayashi LMS, Carvalho FG, Silva AB da, et al. Stress and coping in a sample of medical students in Brazil. Arch Clin Psychiatry (São Paulo). 2015 Feb;42(1):1-5. [ Links ]
10. Pacheco JP, Giacomin HT, Tam WW, Ribeiro TB, Arab C, Bezerra IM, et al. Mental health problems among medical students in Brazil: a systematic review and meta-analysis. Rev Bras Psiquiatr. 2017;(0):369-78. [ Links ]
11. Santos Boni RA dos, Paiva CE, Oliveira MA de, Lucchetti G, Fregnani JHTG, Paiva BSR. Burnout among medical students during the first years of undergraduate school: prevalence and associated factors. PLoS One. 2018;13(3):1-15. [ Links ]
12. McLuckie A, Matheson KM, Landers AL, Landine J, Novick J, Barrett T, et al. The relationship between psychological distress and perception of emotional support in medical students and residents and implications for educational institutions. Acad Psychiatry. 2018;42(1):41-7. [ Links ]
13. Zvauya R, Oyebode F, Day EJ, Thomas CP, Jones LA. A comparison of stress levels, coping styles and psychological morbidity between graduate-entry and traditional undergraduate medical students during the first 2 years at a UK medical school. BMC Res Notes. 2017;10(1):1-10. [ Links ]
14. Bishop SR, Lau M, Shapiro S, Carlson L, Anderson ND, Carmody J, et al. Mindfulness: a proposed operational definition. Clin Psychol Sci Pract. 2004;11(3):230-41. [ Links ]
15. Kabat-Zinn J. Mindfulness-based interventions in context: past, present, and future. Clinical Psychology: Science and Practice. 2003. [ Links ]
16. Tang Y-Y, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Nat Rev Neurosci. 2015 Apr 18;16(4):213-25. [ Links ]
17. Lutz J, Herwig U, Opialla S, Hittmeyer A, Jäncke L, Rufer M, et al. Mindfulness and emotion regulation: an fMRI study. Soc Cogn Affect Neurosci. 2014 June;9(6):776-85. [ Links ]
18. Yang C-C, Barrós-Loscertales A, Pinazo D, Ventura-Campos N, Borchardt V, Bustamante J-C, et al. State and training effects of mindfulness meditation on brain networks reflect neuronal mechanisms of its antidepressant effect. Neural Plast. 2016;2016:1-14. [ Links ]
19. Pascoe MC, Thompson DR, Jenkins ZM, Ski CF. Mindfulness mediates the physiological markers of stress: systematic review and meta-analysis. J Psychiatr Res. 2017 Dec;95:156-78. [ Links ]
20. Galante J, Dufour G, Vainre M, Wagner AP, Stochl J, Benton A, et al. A mindfulness-based intervention to increase resilience to stress in university students (the Mindful Student Study): a pragmatic randomised controlled trial. Lancet Public Health. 2018 Feb;3(2):e72-81. [ Links ]
21. Vibe M de, Solhaug I, Rosenvinge JH, Tyssen R, Hanley A, Garland E. Six-year positive effects of a mindfulness-based intervention on mindfulness, coping and well-being in medical and psychology students: results from a randomized controlled trial. PLoS One . 2018 Apr 24;13(4):e0196053. [ Links ]
22. Bu CNN, Cotzias E, Panagioti M. Mindfulness intervention for foundation year doctors: a feasibility study. Pilot Feasibility Stud. 2019;5:61. [ Links ]
23. Schulz K. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials (Chinese version). J Chinese Integr Med. 2010 July 15;8(7):604-12. [ Links ]
24. Lipp MN. Manual do Inventário de Sintomas de Stress para Adultos de Lipp (ISSL). São Paulo: Casa do Psicólogo; 2000. [ Links ]
25. Biaggio A, Natalício L, Spielberger C. Desenvolvimento da forma experimental em português do Inventário de Ansiedade Traço-Estado (IDATE). Arquivo Brasileiro de Psicologia Aplicada. 1977;3:31-44. [ Links ]
26. Caumo W, Calvetti P, Henriques A. Inventário de Ansiedade Traço-Estado (IDATE). In: Gorenstein C, Wang Y, Hungerbuhler, I. Instrumentos de avaliação em saúde mental. Porto Algre: Artmed; 2016. p. 156-9. [ Links ]
27. Basudan S, Binanzan N, Alhassan A. Depression, anxiety and stress in dental students. Int J Med Educ. 2017 May 24;8:179-86. [ Links ]
28. Fares J, Al Tabosh H, Saadeddin Z, El Mouhayyar C, Aridi H. Stress, burnout and coping strategies in preclinical medical students. N Am J Med Sci. 2016;8(2):75-81. [ Links ]
29. Stormon N, Ford PJ, Kisely S, Bartle E, Eley DS. Depression, anxiety and stress in a cohort of Australian dentistry students. Eur J Dent Educ. 2019 Nov 20;23(4):507-14. [ Links ]
30. Deasy C, Coughlan B, Pironom J, Jourdan D, Mannix-McNamara P. Psychological distress and coping amongst higher education students: a mixed method enquiry. PLoS One . 2014;9(12):1-23. [ Links ]
31. Iorga M, Dondas C, Zugun-Eloae C. Depressed as freshmen, stressed as seniors: the relationship between depression, perceived stress and academic results among medical students. Behav Sci (Basel). 2018;8(8):70. [ Links ]
32. Romani M, Ashkar K. Burnout among physicians. Libyan J Med. 2014;9:23556. [ Links ]
33. Greeson JM, Toohey MJ, Pearce MJ. An adapted, four-week mind-body skills group for medical students: reducing stress, increasing mindfulness, and enhancing self-care. Explore (NY). 2015;11(3):186-92. [ Links ]
34. Phang CK, Mukhtar F, Ibrahim N, Keng S-L, Sidik SM. Effects of a brief mindfulness-based intervention program for stress management among medical students: the Mindful-Gym randomized controlled study. Adv Heal Sci Educ. 2015 Dec 20;20(5):1115-34. [ Links ]
35. van Dijk I, Lucassen PLBJ, Akkermans RP, van Engelen BGM, van Weel C, Speckens AEM. Effects of mindfulness-based stress reduction on the mental health of clinical clerkship students. Acad Med. 2017 July;92(7):1012-21. [ Links ]
36. Yang E, Schamber E, Meyer RML, Gold JI. Happier healers: randomized controlled trial of mobile mindfulness for stress management. J Altern Complement Med. 2018 May;24(5):505-13. [ Links ]
37. Birtwell K, Williams K, van Marwijk H, Armitage CJ, Sheffield D. An exploration of formal and informal mindfulness practice and associations with wellbeing. Mindfulness (NY). 2019 Jan 21;10(1):89-99. [ Links ]
38. Macinko J, Upchurch DM. Factors associated with the use of meditation, U.S. Adults 2017. J Altern Complement Med . 2019 Sep 1;25(9):920-7. [ Links ]
39. Breedvelt JJF, Amanvermez Y, Harrer M, Karyotaki E, Gilbody S, Bockting CLH, et al. The effects of meditation, yoga, and mindfulness on depression, anxiety, and stress in tertiary education students: a meta-analysis. Front Psychiatry. 2019 Apr 24;10:1-15. [ Links ]
40. Damião Neto A, Lucchetti ALG, Silva Ezequiel O da, Lucchetti G. Effects of a required large-group mindfulness meditation course on first-year medical students’ mental health and quality of life: a randomized controlled trial. J Gen Intern Med. 2020;35(3):672-8. [ Links ]
41. Khoury B, Sharma M, Rush SE, Fournier C. Mindfulness-based stress reduction for healthy individuals: a meta-analysis. J Psychosom Res. 2015 June;78(6):519-28. [ Links ]
Received: January 25, 2022; Accepted: January 21, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
