










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML
 Enviar articulo por email
Enviar articulo por emailCompartir

 Permalink
PermalinkRevista Brasileira de História da Educação
versión impresa ISSN 1519-5902versión On-line ISSN 2238-0094
Rev. Bras. Hist. Educ vol.24 Maringá 2024 Epub 06-Nov-2023
https://doi.org/10.4025/rbhe.v24.2024.e302
ORIGINAL ARTICLE
Educational actions as part of trachoma prophylaxis in São Paulo state (1906-1908)

1Universidade Federal do Paraná, Curitiba, PR, Brasil.
In this article, we discuss how health education outside the school environment was highlighted as part of the preventive measures of the Trachoma Prophylaxis and Treatment Commission from 1906 to 1908 in combination with the therapeutic care of trachoma patients. Through evidence found in government reports, news reports, medical articles and state legislation, we seek to show how the government of São Paulo State promoted prophylactic campaigns against trachoma by distributing pamphlets and posters that, combined with the systematic action of government health agents, attempted to promote the dissemination of guidelines on hygiene among the population, pointing out which practices they intended to instill or modify.
Keywords: health education; endemic disease; informal education; public health
Discutimos neste artigo como ações de educação para a saúde fora do espaço escolar ganharam destaque como parte das medidas preventivas da Comissão de Profilaxia e Tratamento do Tracoma entre 1906 e 1908, ao serem conjugadas com os cuidados terapêuticos dos tracomatosos. Procuramos evidenciar, através de indícios encontrados nos relatórios governamentais, nas notícias jornalísticas, nos artigos médicos e na legislação estadual, como o governo de São Paulo promoveu campanhas de profilaxia contra o tracoma por meio da distribuição de panfletos e cartazes as quais, aliadas à atuação sistemática dos agentes sanitários governamentais, concorreram para a disseminação de prescrições higiênicas entre a população, sinalizando quais práticas pretendiam incutir ou modificar.
Palavras-chave: educação para a saúde; doença endêmica; educação informal; saúde pública
Discutimos en este artículo de qué forma acciones de educación para la salud fuera del espacio escolar ganaron destaque como parte de las medidas preventivas de la Comisión de Profilaxis y Tratamiento del Tracoma, entre 1906 y 1908, al ir acompañadas de los cuidados terapéuticos de los tracomatosos. Buscamos poner en evidencia, a través de indicios encontrados en los informes gubernamentales, en las noticias de prensa, en los artículos médicos y en la legislación estadual cómo el gobierno de São Paulo promovió las campañas profilácticas contra el tracoma a través de distribución de panfletos y carteles que, aliados a la actuación sistemática de los agentes sanitarios gubernamentales, buscaban promover la diseminación de prescripciones higiénicas entre la población señalando cuáles prácticas pretendían inculcar o modificar.
Palabras clave: educación para la salud; enfermedad endémica; educación informal; salud pública
Introduction
In the last decades of the nineteenth century, coffee cultivation in the interior of São Paulo State expanded in parallel with the great wave of immigration from Europe to Brazil. Although they were essential for the development of coffee plantations, some of these Italian immigrants were responsible for bringing trachoma or granular conjunctivitis to the southeastern Brazilian state.
The symptoms of this contagious eye disease, which can lead to blindness if not given proper treatment1, were first recorded in Chinese, Sumerian and Egyptian documents written around two thousand years B.C. The disease is likely to have spread in Europe following outbreaks in regions of Asia in the fifth century B.C. due to population displacements caused by the Peloponnesian War. In the Middle Ages, with the movement of men who left for the Crusades (1095-1291), trachoma spread along the route taken by these individuals, beyond European borders (Al Rifai, 1988; Taylor, 2009).
However, with inconstant endemic cycles, in the following centuries, doctors and governments did not pay as much attention to trachoma as they paid to the bubonic plague, smallpox or syphilis, a situation that began to change after Napoleon Bonaparte’s Egyptian Campaign (1798-1802). On African battlefields where granular conjunctivitis was endemic, ophthalmia killed French and British soldiers indiscriminately, and when they crossed vast territories to return to their countries, they spread the disease throughout most of Europe (Al Rifai, 1988; Taylor, 2009). At the same time, the poor neighborhoods of European industrial cities where workers lived in cramped unsanitary housing were propitious spaces for the multiplication of cases of trachoma (Taylor, 2009).
In Brazil, trachoma was most likely brought to the northeast of the country in the mid-eighteenth century by gypsies from Portugal (Burnier, 1932). In 1863, newspapers in Ceará State published one of the first reports on the operation of a trachoma patient in the country, at the Santa Casa de Misericórdia hospital in Fortaleza (Lódola, & Campos, 2018). Surgery was recommended for severe cases of trachoma, which occurred after repeated reinfections, when the eyelashes curved inwards, severely deforming the eyelid and scraping the cornea. Surgical intervention sought to reverse this situation before the lesions resulted in trachomatous blindness. However, there were several proposed treatments for each stage of the disease. Among the most frequent were washing the eyes with boric water and the use of zinc sulfate or resorcinol, accompanied by eye protection with daily changes of dressings (e.g., Barreto, 1905; Ottoni, 1906). Doctors also warned about the dangers of the indiscriminate use of eye drops, and some prescribed only cleaning with ‘sublimated water’ (Vieira, 1905)2.
Around fifteen years after the surgery performed in Fortaleza, ophthalmologist David Ottoni, when traveling through the northeast region of the country, identified a large number of people with granular conjunctivitis in the Cariri valley (in the southern region of Ceará State) and neighboring areas of the interior of the states of Pernambuco and Paraíba and also in Sergipe, Rio Grande do Norte and Bahia. Short-distance navigation on minor rivers in the area and along the São Francisco River helped to spread the disease throughout the region. According to this specialist, trachoma had not reached other parts of Brazil at that time because the means of transport between the regions of the country were precarious (Ottoni, 1898; Ottoni, 1906).
Towards the end of the nineteenth century, this situation began to change. In São Paulo State, it was likely that granular conjunctivitis was brought by the large number of Italian immigrants who arrived at the port of Santos from 1887 onwards, coming from places where trachoma had become endemic3. According to Emilio Ribas (1907, p. 228), in the 1890s “[…] the first references to the disease […]” were made in the interior of the state4.
At this time, most of the immigrants underwent a quick medical exam at the port of Santos upon arrival and then made their way to Immigrant Inn in the state capital, where conditions were cramped and contagion was inevitable5. After bureaucratic procedures, these individuals boarded trains that headed for the so-called ‘west of São Paulo’ (northeast of the state). Considering that the trip could take a few days, it was not uncommon for people to walk around their carriages, and the trains made stops at several stations. Little by little, the number of cases of granular conjunctivitis increased in the interior of São Paulo and, at the beginning of the 20th century, the number of victims of the disease attracted the attention of travelers and doctors (Lódola, & Campos, 2018).
It was in this context that, in 1906, the Trachoma Prophylaxis and Treatment Commission was established as part of the restructuring of the São Paulo State Sanitation Service, under the direction of Dr. Emílio Ribas. The director admitted that there had been a delay in taking measures against trachoma and justified it by claiming that the fight against yellow fever had catalyzed state efforts regarding public health, concluding that the end of the epidemics of this disease had made it possible to take action to systematically combat trachoma (Ribas, 1907). These words were also used to praise the positive results of the fight against the aedes aegypti mosquito, yet another ratification of the thesis of Carlos Finlay (1881-82) confirmed by Walter Reed, of which Ribas was a pioneer advocate in Brazil (Martins, 2015).
At the turn of the twentieth century, the framework of prophylactic measures taken by the government in epidemics (such as yellow fever) and to combat endemics (such as trachoma) were, in general terms, based on hygienic practices that dated back to the eighteenth century and which had been renewed through changes triggered by bacteriology beginning in the second half of the nineteenth century (Faure, 2008). The main measures were: cleaning streets and houses, especially collective housing, sanitary policing services, isolation of the sick, improvement of urban infrastructure (adaptation/construction of water and sewage systems, paving of public roads) and the renovation of buildings to promote a healthy environment6. There was also a prophylactic framework mostly comprising explicit educational measures, ranging from the publication of medical ‘advice’ in the press to the justifications presented for notifications by the sanitation police.
In the early twentieth century, trachoma was considered a microbial disease with no identified causative agent. In 1905, the ophthalmologist Seraphim Vieira, in an article published in the Revista Médica de S. Paulo (São Paulo Medical Journal) stated that he agreed with the “[…] opinion of those who consider trachoma to be a malignant production analogous to the tubercle” (Vieira, 1905, p. 297). Regardless of the important discussion of the etiologic agent of granular conjunctivitis7, the doctor drew a comparison with tuberculosis. Both diseases victimized people insidiously, and in the case of trachoma, often more than once. Like tuberculosis, the possibility of maintaining or regaining health and preventing the spread of trachoma largely relied on hygienic practices. In addition to providing information about the disease and its physical consequences, it was necessary to provide education with regard to health, with verbal or written recommendations, to change people’s attitudes in everyday life.
Of the international studies on trachoma conducted from a historical perspective, most focus on the nineteenth and early twentieth century, covering the actions of government and philanthropic entities in the fight against and prophylaxis of the disease and the discussions on the etiology and treatment of trachoma, in some cases evidencing aspects related to the port and immigration policies of the time (e.g. Al Rifai, 1988; MacCallan, 2015; Milot, 2010, Taylor, 2009). Fewer studies link granular conjunctivitis and education, and these works generally focus on the school environment. These include: the article by Stephenson (1900) on the disease in London schools between 1852 and 1900; the study by Allen & Semba (2002) on the high incidence of trachoma and the prophylaxis of the disease in North American schools (including indigenous reservations) between the 1910s and the late 1950s; and the article by Di Liscia & Fernández (2014) on the project to establish a school for trachoma patients in northern Argentina in the context of organizing the national health policy in the first half of the twentieth century.
In Brazil, in several studies, trachoma is part of the discussions related to public health and the organization of the sanitation apparatus (e.g. Castro-Santos, 1998; Hochman, 1998). With specific regard to São Paulo State, we can highlight the studies by Ribeiro (1993) and Telarolli Junior (1996). Among the works that focused on granular conjunctivitis as a central theme, we have that of Scarpi (1991), who wrote a text with a summary of considerations on trachoma in Brazil, emphasizing the role of the federal government in combating the disease. As an example of a regional study, there is that of Schwartsmann (2020), who linked the spread of trachoma to the immigration flow in Rio Grande do Sul and performed a data analysis on patients treated at the Santa Casa de Misericórdia hospital in Porto Alegre in the early twentieth century. Focusing on the disease in São Paulo, we have the study by Luna (1993), who carried out an epidemiological mapping of the disease in the state of São Paulo between 1890 and 1990. There is also the research conducted by Gois (2020), who studied trachoma in the interior of São Paulo from 1880 to 1916 and who, based on medical organization and action, evidenced a process led by Emilio Ribas to expand the inclusion of the Sanitation Service in the political and governmental scope of the state. There is also the study by Lódola & Campos (2018) who discussed the medical propositions related to granular conjunctivitis before the establishment of the treatment centers set up to combat trachoma in 1906. In general, Brazilian studies of trachoma do not address educational issues.
In historical studies of Brazilian education in the latter decades of the nineteenth century and the first half of the twentieth century, the theme of health was highlighted in articles and books on educational concepts and proposals and Brazilian education (e.g., Carvalho, 1998; Souza, 1998). The theme became increasingly prominent in publications that, based on the questioning of medical and government sources, discussed health in schools and the health of those who visited them (e.g., Bertucci, 2014; Carvalho, 1997; Gondra, 2004; Stephanou, 2006). At the same time, in recent years, the number of texts in books, booklets, pamphlets and posters designed to train teachers and educate students regarding health has grown (e.g., Carvalho, 2021; Paiva & Gondra, 2017; Rocha, Viviani, & Lima, 2017).
Among the studies that focused on health education in schools, and São Paulo as a fundamental axis, is the book written by Marques (1994), which analyzed the medical-eugenic debates of the 1920s and the medical propositions for the instruction of elementary school teachers, who would inculcate hygienic practices and rules of ‘good conduct’ into students. Another pertinent work is that of Rocha (2003) who, based on considerations about the 1910s, focused on the Instituto de Higiene de São Paulo in the 1920s, emphasizing the institution’s educational endeavor to transform regular students into health educators8. An example of more recent publications is that of Soares (2022), addressing the health education experiment in 1926 for pre-school children (aged 4 to 7) at the kindergarten of the Escola Normal of the City of São Paulo. Parallels can be drawn between this public entity and nursery schools for the children of workers that were subsidized by the state government. Despite the relevance of the production of health education for schoolchildren, we perceive a gap in the historiography of prophylactic education outside the school environment, specifically linked to endemic diseases at the turn of the 19th and early 20th centuries.
Thus, bearing in mind the words of Revel (2010, p. 438), who claimed that “[…] to vary the focus of an object does not only involve increasing or decreasing its size in the viewfinder, but modifying its shape and plot […]”, in this article, we discuss how health education actions outside of school, but which also affected students, became increasingly important in São Paulo in the early twentieth century as part of the actions of the Trachoma Prophylaxis and Treatment Commission (1906-1908), combined with the therapeutic care of trachoma patients. We attempt to show, through evidence (Ginzburg, 1991) found in government reports, news reports, medical articles and state legislation, how the São Paulo government promoted prophylactic campaigns against granular conjunctivitis by circulating pamphlets and displaying posters that, together with the systematic action of government health agents, sought to promote the dissemination of hygienic prescriptions regarding which practices they intended to diffuse or change.
Health organization and education - trachoma
Initiatives to promote health education by the São Paulo state government can be seen in the legislation, beginning with the first resolutions related to the Sanitation Service. The government division was organized after the proclamation of the Republic, based on a resolution by the federal government that transferred responsibility for terrestrial public health to the states. Created in 1891, when yellow fever threatened agricultural expansion in São Paulo9, the structure of the Sanitation Service was established in 1892 and reorganized months later (Lei nº 12, 1891; Lei 43, 1892).
On 4 September 1893, Law 240 reorganized the Sanitation Service, which had a team of 22 people: 1 director, 12 health inspectors, 2 pharmacists and, in supporting positions, 1 secretary, 1 official (of the secretariat) and 2 amanuenses, 1 doorman and 2 auxiliaries (Lei nº 240, 1893). The law also determined that municipalities were responsible for public health in their jurisdictions, including sanitation, inspections, vaccinations, sanitation police and the organization of public assistance services, with the municipalities incurring all the expenses. The state government was responsible for adopting measures to keep epidemic diseases from entering the state, conducting the scientific study of matters relevant to public health, and carrying out inspections of the practice of medicine and pharmacy (Lei nº 240, 1893). Thus, the decentralization that occurred at the federal level also guided the development of the structure of the state’s Sanitation Service.
Three years later, Decree 394 regulated the Sanitation Service, and one of the director’s duties was particularly interesting:
Article 25 (...) § 5 - To give [people] advice on hygiene at times when their health is in danger, indicating the resources for preservation in cases of contagious diseases and the precautions necessary to stem the spread of these diseases, using a suitable publicity campaign for this purpose (Decreto nº 394, 1896).
Considering the way in which the text was written, the advice, in ‘times when health is in danger’, would only be required in exceptional situations, that is, during epidemics or outbreaks of endemic diseases. However, in the late nineteenth century, events of this nature, notably yellow fever epidemics, were a regular occurrence in several locations in the state and this advice, given almost every year10, could be accepted because of its results and, little by little, incorporated into everyday practices, extrapolating the specific events for which it was intended.
In 1899, as part of efforts to prevent the spread of the bubonic plague that threatened the state from the port of Santos, the Sanitation Service distributed a booklet with instructions to residents of São Paulo (Image 1). Of these recommendations, those related to hygiene stand out.
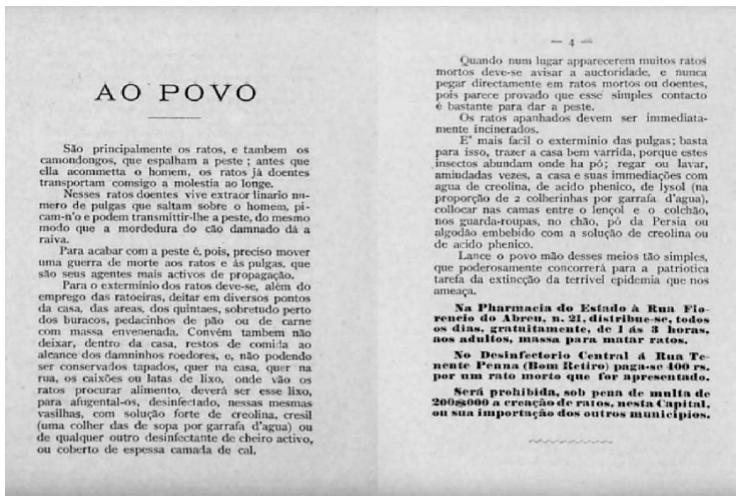
In addition to Portuguese, the text was also written in four other languages: Italian, German, French and English. The latter three were intended to facilitate communication for those who did not speak the national language or Italian, which was the language of most of the immigrants who were arriving in the state or already living in São Paulo, including the capital11.
The booklet contained information on the disease and instructions on how to kill rats and exterminate fleas (with punishments for profiteers in this dangerous situation), which occupied almost as much space as the advice that highlights the importance of daily actions to prevent the spread of the disease. The advice included not leaving scraps of food uncovered and sweeping the house well. The advice had many recommendations regarding the potential positive effects of these activities, and these are likely to have been echoed by those who read or heard about the booklet, which had a strong title: Peste (Plague).
At this time, an article in the working-class newspaper Folha do Braz, published in the largest working-class neighborhood of São Paulo, commented on the rising demand for disinfectant in the city, stating that using this product had become a common practice in the state since the days of the yellow fever epidemics (Bertucci, 2020). According to Bertucci (p. 6), these considerations were signs that a number of individuals “ […] had not only accepted the medical advice at a particular time [the epidemic], but had adopted a prescription that educated them about the importance of having a clean house [...]”. This was something that the Peste booklet reiterated, thereby helping to maintain a change in the behavior of those who lived in the state capital and interior. The institutionalization of educational practices by the sanitary movement of the second half of the 1910s and the legislative changes from the 1920s onwards, expanded actions that included the distribution of printed matter of this type. As time went by, these materials came to contain more illustrations and were eventually published in color, including material used to fight the bubonic plague (Stern & Marques, 2017).
As for the plague of 1899, it did not spread around the state, and at the beginning of the twentieth century the yellow fever epidemics in the interior of São Paulo had ended. It was in this context that the discussions on taking action to combat trachoma became more predominant on the agenda of the São Paulo government, combining efforts of the Secretary of Agriculture and the board of the Sanitation Service (subordinate to the Secretary of the Interior).
In this respect, in 1904, the secretary for Agriculture nominated an ophthalmologist to examine the immigrants arriving on ships before they came ashore at Santos port12 to prevent trachoma sufferers from entering the state (Vieira, 1905). Meanwhile, health inspector Guilherme Álvaro sent his superior, Emilio Ribas, a report written after visiting houses and schools and treating trachoma patients on several farms in the coffee region in the municipality of Ribeirão Preto (Álvaro, 1904). The health inspector had been commissioned by Ribas to carry out this inspection (Vieira, 1905).
In his report, the ophthalmologist Guilherme Álvaro affirmed that the high rates of contagiousness among the inhabitants of the region were related to contaminated objects, such as sheets and cloths use by trachoma sufferers to wipe their sweaty faces as they toiled on the farm and passed from one person to another, spreading the disease to other workers. According to the doctor, this situation, added to the precarious hygienic practices of the workers and the lack of cleanliness in their homes, aided the spread of the microorganism and more contamination (Álvaro, 1904). This is exactly what happened in a large part of the São Paulo coffee zone.
According to a statement by Emilio Ribas, it was the clarity and objectivity of Guilherme Álvaro’s report that led him to publish it in Portuguese and Italian, delivering several copies to municipal authorities and state farmers for distribution among farm workers (Ribas, 1907)13. Informing local authorities and landowners and demonstrating the importance of educating workers may also have been one of Emilio Ribas’ strategies to highlight both the importance of combating the disease and the possibility a state agency, the Sanitation Service, undertaking this medical and educational task.
Ribas’ initiative to use printed matter for educational purposes, which would become an important facet of the Sanitary Service’s actions against trachoma, met demands for the dissemination of recommendations on the disease. One of these requests came from the ophthalmologist Mello Barreto, who in 1903, criticizing the neglect of municipal authorities in the fight against granular conjunctivitis, stated in an article in O Estado de S. Paulo that it was necessary for “[...] doctors to visit the farms where there are patients with trachoma and offer advice on the necessary measures to avoid contagion” (Barreto, 1903, p.4). The distribution of printed material, in more than one language, was certainly an initiative in keeping with the ophthalmologist’s proposal.
Cheaper printed material in the early twentieth century, combined with the expansion of the railway network and the multiplication of ‘newspaper outlets’, such as railway stations, tobacconists, kiosks and bookstores, allowed the owners of periodicals and their collaborators to spread ideas and ways of life (often referred to as 'civilized' or 'modern') to remote areas distant from major cities (De Luca, 2008). The dissemination of ideas like that of Mello Barreto, as well as medical instructions regarding how to avoid trachoma, benefited from these factors.
The early 1900s were times of political upheaval in São Paulo, including the revision of the state constitution, which led to a greater concentration of administrative power in the state government. This cannot be dissociated from the demands and difficulties involved in dealing with public health issues that directly impacted the state and, evidently, the municipal economy (Telarolli Junior, 1996). The way the problem of trachoma was presented, demanding permanent action in a large part of the state, and how the Sanitation Service was highlighted (due to overcoming the yellow fever epidemics) as the best option to carry out actions of this magnitude, is emblematic of that time. The structure of the state health department was reorganized.
On 17 February 1905, the newspaper O Estado de S. Paulo published a note on this reorganization:
Two days ago, the new regulation that, we are informed by a competent source, is a modification of the old one by a commission charged with this task, was delivered to Dr Emílio Ribas, director of the State Sanitation Service [...].
In accordance with the advice of those with the greatest experience, and in keeping with the ideas expressed in the reports of the Secretary of the Interior and director of the Sanitation Service, the commission sought to centralize hygiene services as much as possible, placing them within the purview of the state government, except in cases specifically concerned with hygiene and urban improvements (Notas…, 1905, p.1).
Regarding the changes, the news did not provide many details: the new structure ‘takes better care’ of the prophylaxis of contagious diseases, such as “ […] trachoma, a disease that is already harming our credit abroad, such has been its development, especially among rural workers” (Notas…, 1905, p.1).
The next year, in January 1906, the new reorganization of the Sanitation Service, which divided the state into 14 districts, was approved14. In this new structure, health inspectors were to give advice on the execution of local sanitation services, work with municipalities to ensure that actions “ […] essential for local hygiene” were taken, and fulfill the role of the sanitation police. Among the duties of the sanitary police were the inspection of public and private buildings and school hygiene, as well as vaccination inspection and the observation of newly arrived immigrants (Decreto nº 1343, 1906).
It was also the duty of health inspectors to ‘provide the population with advice on hygiene’. When they identified a person with a contagious disease and during epidemics, they had to: direct the disinfection and isolation service for patients with communicable diseases; promote prophylactic hygiene; organize the surveillance of people who had contact with patients with contagious diseases and the disinfection of buildings where deaths from this type of disease occurred, in addition to publishing in the local press the preventive hygienic measures that people should follow (Decreto nº 1343, 1906).
Not only did the reform promoted in 1906 make it possible to centralize public health measures under state orders, but it also showed that educational activities (on the advice of the inspector or via newspaper texts) were among the measures taken to combat diseases. This was made clear in the decree that created, in the Sanitation Service Board of Directors, the service that was placed in charge of the prophylaxis and treatment of trachoma (Decreto nº1395, 1906).
To fight the ‘slowly kindled fire’
Created by Decree 1.395, of 3 September 1906, the Trachoma Prophylaxis and Treatment Commission15 was directly subordinate to the director of the Sanitation Service and headed by a doctor who, in addition to supervising its work, presented reports and proposals for action to the Commission. At the treatment centers set up around the state, doctors worked alongside assistants and disinfectors (the number of which would vary ‘according to the needs of the job’). It was the duty of the head of the Commission that, when necessary, could perform treatment and surgery on trachoma patients to: “ […] formulate advice and instructions for free distribution and widespread publicity”. As for the doctors at the treatment centers, according to Article 5 of the decree, it was their duty to:
1) Apply prophylactic means and treat those affected in treatment centers, hospitals designated by the head of the Commission and at any location where the disease manifests;
2) Distribute the printed instructions and advise on the necessary measures for the prophylaxis of the disease. (...)”. Other eye diseases, if detected, should also be properly treated (Decreto nº 1395, 1906).
At the same time, attention was redoubled with regard to elementary school children. Students with granular conjunctivitis could transmit the disease to classmates and, indirectly, to their families. This was an international concern that reverberated in the considerations of Emilio Ribas (1907, p. 230) and which in some countries even resulted in the creation of schools especially for trachoma patients (Hygiene…, 1907; Di Licia, & Fernández, 2014). Trachoma, identified by the director of the Sanitation Service as a “ […] slowly kindled fire” across São Paulo State, needed to be stopped (Ribas, 1907, p. 229).
In this respect, in 1906, based on initiatives of the Secretariat of the Interior and the Secretariat of Agriculture, the state government promoted a campaign articulating simultaneous actions by creating prophylactic and treatment centers for trachoma, monitoring the disease in schools and examining passengers in Santos. Every initiative sought to identify and treat trachoma and provide advice on cleanliness to avoid (re)infections. With the treatment centers operational, it became compulsory to report any cases of trachoma in the state (Decreto nº 1395, 1906).
The treatment centers (and sub-units) for the fight against granular conjunctivitis were officially opened in October 1906 in 36 municipalities in the state16. At the time, 45 doctors were nominated to provide treatment in these locations, some of them working in more than one treatment center with the help of assistants (who welcomed patients and sometimes bandaged them, etc.) and disinfectors (Góis, 2020). In 1908, according to a note issued by the secretary of the interior, there were 59 doctors and 362 other functionaries working in treatment centers fighting trachoma in the state (Commissão…, 1908, p. 278).
The map showing the municipalities where the treatment centers were established in 1906 (Image 2) illustrates how widespread trachoma was throughout the coffee growing zone of São Paulo State at the time. The opening of some of these treatment centers in railway towns such as Sorocaba and Botucatu is a sign of the role the railroad played in the spread of the disease. The existence of treatment centers in the port town of Santos and in the city of São Paulo (location of the Immigrant Inn), in addition to part of the actions taken in an attempt to contain the spread of the disease in the countryside, also indicate the multiplication of cases of the disease in these locations and surroundings, either through contact between newcomers and Brazilians, or because many immigrants settled in the state capital.
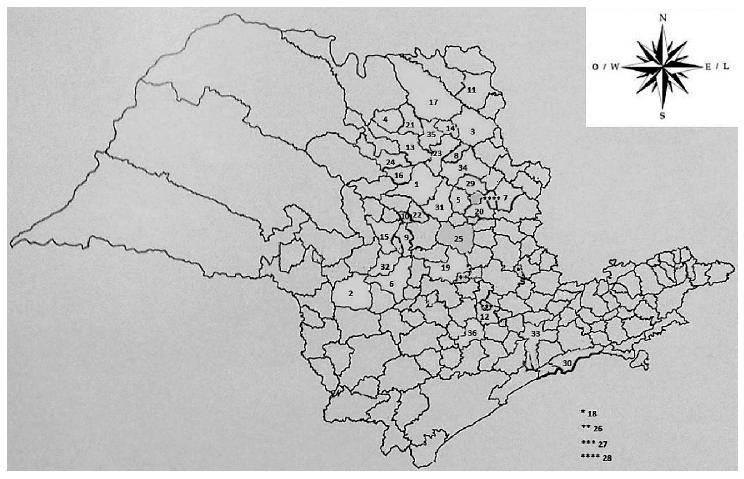
1. Araraquara, 2. Avaré, 3. Batatais, 4. Bebedouro, 5. Belém do Descalvado (Descalvado), 6. Botucatu,7. Casa Branca, 8. Cravinhos, 9. Dois Córregos, 10. Dourado, 11. Franca, 12. Itu, 13. Jaboticabal, 14. Jardinópolis, 15. Jaú, 16. Matão, 17. Nuporanga, 18. Pedreira, 19. Piracicaba, 20. Pirassununga, 21. Pitangueiras, 22. Ribeirão Bonito, 23. Ribeirão Preto, 24. Ribeirãozinho (Taquaritinga), 25. Rio Claro, 26. Rio das Pedras, 27. Salto, 28. Santa Cruz das Palmeiras, 29. Santa Rita do Passa Quadro, 30. Santos, 31. São Carlos do Pinhal (São Carlos), 32. São Manuel do Paraíso (São Manuel), 33. São Paulo, 34. São Simão, 35. Sertãozinho, 36. Sorocaba.
Source: Mapa realizado pela autoria a partir de Bassanezi et al. (2008, p. 131).
Figure 2 Map of the municipalities with Trachoma Treatment Centers - 1906 (territorial division of the state in 1904).
In trachoma prophylaxis and treatment centers, disseminating information about the disease and providing advice on how to avoid granular conjunctivitis was an obligation outlined in legislation, as well as performing eye exams and providing care for trachoma patients (other identified eye diseases were also treated) (Decreto nº 1395, 1906). At the same time, pamphlets and booklets on trachoma were constantly being distributed free to the population, and posters were displayed with warnings about the risks of the disease and ways to prevent it. The head of the Trachoma Prophylaxis and Treatment Commission, Dr Eusébio de Queiroz Mattoso, who also coordinated the ophthalmology ward at the Santa Casa hospital in São Paulo, was responsible for preparing these materials (which were standardized to facilitate educational actions) and distributing them to the treatment center (Decreto nº 1395; Serviço Sanitário, 1906; Serviço Sanitário, 1907a).
The treatment centers had to forward monthly reports to the head of the Commission with “[...] a summary of the services provided by the doctors in charge of services at the different locations, noting activities at hospitals, patient statistics, etc.” (Decreto nº 1395, 1906). However, reports were issued daily, providing information about activities at treatment centers, listing requirements and requesting materials and resources to treat trachoma patients, including ambulances. Requests were also regularly made for pamphlets that taught people how to combat granular conjunctivitis. These requests included repeated demands for copies in Italian, called Instruzzioni (sic) (Instructions) to be distributed “[…] methodically and for maximum effect to the Italian population” (e.g., Serviço Sanitário, 1907a, p. 805).
Posters were constantly displayed in the busiest locations in cities (such as train stations) and also on farms. An example of this kind of action was the report sent to the Sanitation Service Board of Directors by the doctor at the treatment center in the municipality of Ribeirão Bonito. In March of 1907, he placed a second order for over 100 posters to replace those that had been on display and were damaged by the rain (Serviço Sanitário, 1907b, p. 770)17.
The newspapers also took part in this educational initiative. In the town of Itu, which had a trachoma treatment center, A Federação, a catholic association newspaper, published an article that taught people how to avoid contamination through contact with trachoma sufferers (by not sharing towels or utensils, separating sufferers’ belongings from those of other people) and warned of the negative effects of habits such as ‘rubbing your eyes with your clothes’ and wiping the eyes ‘with the sleeve of your dress’. The text recommended that people should “ […] rub their eyes with absorbent cotton, change bed linen frequently and wash it with soap or boil it before using it again [...], avoid dust”. It also stated that “ […] flies, mosquitos and especially biting midges take the disease from the eyes of sufferers to the eyes of the healthy”. It also warned that people should “[…] not allow children to have dirty eyes; [...] talk to a doctor as soon as the eyes are affected” (Trachoma, 1907, p. 3). The format of the recommendations in the journal, in quotation marks and in sequence, with one to a line, suggests that they were reproduced from a poster or pamphlet.
Between October 1906 and June 1908, actions were intense at the Trachoma Prophylaxis and Treatment Commission treatment centers, and placing doctors among the urban and rural population can be gauged by how they intensified their actions, writing prescriptions to treat hookworm and malaria, divulging the smallpox vaccine, treating snake bites and campaigning against alcoholism (Serviço Sanitário, 1908, p. 1905). As for trachoma, during this period 410,084 individuals were examined and 104,432 were diagnosed with granular conjunctivitis, and 2,828,115 dressings were applied and 1,404 trachoma surgeries were performed (São Paulo, 1908).
In schools, in the one year and seven months that the Commission was active, around twenty thousand students were found to have the disease (São Paulo, 1908). The various letters sent to the Sanitary Service management reporting cases of trachoma among schoolchildren are also an indication of the spread of the disease both in small towns and urban centers. In February 1907, the commission’s doctor, who conducted an inspection in the village of Rebouças, in the municipality of Campinas, reported that, after it was discovered that a student at the isolated school had trachoma, he requested that she be removed from classes until she was fully recovered (Serviço Sanitario, 1907b). During the same period, in the modern school group (1903) of Araraquara (Souza, 1998), several students were identified with granular conjunctivitis, and the school principal was ordered to send these patients to the health center for treatment. The service would be carried out “[...] at a time reserved for high school students”. Male students with trachoma would be treated on Mondays, Wednesdays and Fridays, and female students with trachoma on Tuesdays, Thursdays and Saturdays (Serviço Sanitario, 1907c, p. 980)18. Times like these were propitious for the distribution of leaflets with instructions for preventing trachoma and also for oral advice on how to avoid the disease.
The results of educational activities during this period are difficult to measure. Nevertheless, the instructions and advice that were given must have contributed to several of these almost 105,000 trachoma patients and many children with granular conjunctivitis undergoing the treatments proposed by the doctors, accepting the recommended bandages and dressing or agreeing to undergo surgery. In 1908, a text with considerations on the fight against trachoma, attached to the report of the Secretary of the Interior, stated that “[...] the embarrassment shown by the adult colonist, not allowing himself to be cured so as not to lose a few days’ wages, are (sic) happily disappearing and the beneficial results of the publicity campaign are already being felt” (São Paulo, 1908, p. 12).
Final remarks
In June of 1908, Decree 1629 (1908) determined the dissolution of the Trachoma Prophylaxis and Treatment Commission, “ […] dispensing with the services of all the doctors, assistants and disinfectors that comprise it as of the first of July”.
What could have caused this resolution if the results achieved by the Commission had been so promising? In the Revista Médica de S. Paulo, published on 15 July 1908, a reproduction of the statement of Carlos Guimarães, Secretary of the Interior, forwarded to the president of São Paulo State, may provide some clues. After voicing praise for the service provided, Guimarães mentioned, without comment, the growing number of treatment centers, doctors and auxiliaries, and stated that, “ […] due to its provisional organization”, the Commission had no budgetary allocation and its expenses were paid from the “[…] public aid” budget (Commissão…, 1908, p. 278). This ‘provisional’ nature may also have facilitated the expansion of the activities of the treatment centers, from the fight against other endemic diseases to publicity against alcoholism, which may have strengthened a perspective of function deviation and extra expenses among government officials19.
Concluding his remarks, the secretary stated that trachoma was a disease that required long treatment and would need an effectively structured care service (with ‘departmental sanatoriums’). However, as there was no budget or legislative authorization for this, it was better to delegate the service to the Santa Casa de Misericórdia hospitals with a prior agreement (Commissão…, 1908, p. 278). And so it was done. In this new context, the educational activities promoted by the Trachoma Prophylaxis and Treatment Commission ceased, at least in the form they had taken from 1906 to 1908. Articles on the disease continued to appear in newspapers and at Sanitation Service treatment centers in an attempt to spread information to reduce the number of trachoma patients, but the widespread distribution of pamphlets and posters had ceased.
REFERENCES
Allen, S. K., & Semba, R. (2002). The trachoma “Menace” in the United States, 1897-1960. Survey of Ophtalmology, 47(5), 500-509. [ Links ]
Al Rifai, K. M. J. (1988). Trachoma through history. International Ophthalmology, 12, 9-14. [ Links ]
Álvaro, G. (1904). Profilaxia e tratamento das ophtalmias do oeste de São Paulo. Revista Médica de S. Paulo, 24, 580-582. [ Links ]
Barreto, M. (1903, 22 de agosto). O tracoma. O Estado de S. Paulo, p. 4. [ Links ]
Barreto, M. (1905). Traitement du trachome. Revista Medica de S. Paulo, 9, 195-199. [ Links ]
Bassanezi, M. S. C. B., Scott, A. S. V., Bacellar, C. A. P., & Truzzi, O. M. S. (2008). Atlas da imigração internacional em São Paulo 1850-1950. São Paulo, SP: Editora Unesp. [ Links ]
Benedetti, A. (1911, 31 de outubro). O trachoma. Revista Medica de S. Paulo, 20, 379-381. [ Links ]
Bertucci, L. M. (2020). A casa do trabalhador em tempos epidêmicos. São Paulo, primeiras décadas republicanas. Revista Mundos do Trabalho, 12, 1-18. Recuperado de: https://doi.org/10.5007/1984.9222.2020.e75456 [ Links ]
Bertucci, L. M. (2014). A saúde entre a lei e o costume na escola primária paranaense, final dos anos 1910. Educar em Revista, 54, 123-140. Recuperado de: https://www.scielo.br/j/er/a/ks4KcnjGJHpx6VQnHMStdQG/?lang=pt [ Links ]
Burnier, P. (1932). O tracoma no Brasil: sua origem e difusão. Arquivos do Instituto Penido Burnier, 1(1), 62-73. [ Links ]
Carvalho, L. D. (2021). Higiene brasileira: as lições de Belisário Penna para as escolas normais. Revista História da Educação, 21, e100569. Recuperado de: http://dx.doi.org/10.1590/2236-3459/100569 [ Links ]
Carvalho, M. M. C. (1998). Molde nacional e fôrma cívica. Bragança Paulista, SP: EDUSF. [ Links ]
Carvalho, M. M. C. (1997). Quando a história da educação é a história da disciplina e da higienização das pessoas. In M. C. de Freitas (Org.), História social da infância no Brasil (p. 291-309). São Paulo, SP: Cortez. [ Links ]
Castro-Santos, L. A. (1998). As origens da reforma sanitária e da modernização conservadora na Bahia durante a Primeira República. Dados, 41(3). Recuperado de: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0011-52581998000300004 [ Links ]
Commissão de Prophylaxia e Tratamento do Trachoma. (1908). Revista Medica de S. Paulo, 13, 278. [ Links ]
Centro de Vigilância Epidemiológica “Prof Alexandre Vranjac” [CVE]. (n.d.). Tracoma. Recuperado de: http://www.saude.sp.gov.br/cve-centro-de-vigilancia-epidemiologica-prof.-alexandre-vranjac/areas-de-vigilancia/oftalmologia-sanitaria/agravos/tracoma [ Links ]
Decreto nº 394, de 7 outubro de 1896. (1896). Approva o regulamento do Serviço Sanitário. Recuperado de: www.al.sp.gov.br/repositorio/legislacao /decreto/ 1896/ decreto-394-07.10.1896.html [ Links ]
Decreto nº 1.343, de 27 de janeiro de 1906. (1906). Divide o territorio do Estado em districtos sanitarios e dispõe a respeito da policia sanitaria. Recuperado de: www.al.sp.gov.br/repositorio/legislacao/decreto/1906/decreto-1343-27.01 [ Links ]
Decreto nº 1.395 de 3 de setembro de 1906. (1906). Cria na Diretoria do Serviço Sanitário, o serviço de profilaxia e tratamento do Trachoma. Recuperado de: www.al.sp.gov.br/repositorio/legislacao/decreto/1906/decreto-1395-03.09 [ Links ]
Decreto nº 1.629, de 22 de junho de 1908. (1908). Dissolve a Commissão de Prophylaxia e Tratamento do Trachoma. Disponível em: https://leisestaduais.cp,;br/sp/decreto-n-1629-1908-sao-paulo-dissolve-a-comissao-de-profilaxia-e-tratamento-do-tracoma [ Links ]
De Luca, T. R. (2008). A grande imprensa na primeira metade do século XX. In A. L. Martins, & T. R. De Luca (Orgs.), História da Imprensa no Brasil (p.149-175). São Paulo, SP: Contexto. [ Links ]
Di Liscia, M. S., & Fernández, M. E. (2014). Serapados o juntos? Contagio, escolaridad y tracoma en Argentina (1884-1940). Educar em Revista, 54, 97-121. Recuperado de: https://revistas.ufpr.br/educar/article/view/38204/23910 [ Links ]
Directoria Geral de Estatistica. (1926). Recenseamento do Brazil, realizado em 1º de setembro de 1920. 4. População. Rio de Janeiro, RJ: Typ. da Estatística. [ Links ]
Faure, O. (2008). O olhar do médico. In A. Corbin, J. J. Courtine, & G. Vigarello (Dirs.), História do corpo (2a ed., p. 13-55). Petrópolis, RJ: Vozes. [ Links ]
Ginzburg, C. (1991). Mitos, emblemas e sinais. São Paulo, SP: Companhia das Letras. [ Links ]
Góis, S. L. M. (2020). História do tracoma em São Paulo: uma rede formada entre as linhas da sociedade e os laços de uma doença (1880-1916) (Tese de Doutorado em Política Científica e Tecnológica). Universidade Estadual de Campinas, Campinas. [ Links ]
Gondra, J. G. (2004). Artes de civilizar. Rio de Janeiro, RJ: Editora UERJ. [ Links ]
Hochman, G. (1998). A era do saneamento. São Paulo, SP: Hucitec. [ Links ]
Hygiene e prophylaxia das molestias da cornea (grunulose, trachoma). (1907). Revista Medica de S. Paulo, 17, 356-359. [ Links ]
Lei nº 12, de 28 de outubro de 1891. (1891). Organiza o Serviço Sanitário do Estado. Recuperado de: https://www.al.sp.gov.br/repositorio/legislacao/lei/1891/lei-12-28.10.1891.html [ Links ]
Lei nº 43, de 18 julho de 1892. (1892). Organiza o Serviço Sanitario do Estado. Recuperado de: www.al.sp.gov.br/repositorio/legislacao/lei/1892/lei-43-18.07.1892.html [ Links ]
Lei nº 240, de 4 de setembro de 1893. (1893). Reorganiza o Serviço Sanitário de São Paulo. Recuperado de: www.al.sp.gov.br/repositorio/legislacao/lei/1893/lei-240-04.09.1893.html [ Links ]
Lódola, S., & Campos, C. (2018). “Era urgente e indispensável agir”: o tracoma em São Paulo no início do século XX. Physis - Revista de Saúde Coletiva, 28(4), 2-21. Recuperado de: https://www.scielo.br/j/physis/a/8v6crYBDWwFyVFmLFNv9Bvg/?lang=pt [ Links ]
Luna, E. J. A. (1993). A epidemiologia do tracoma no estado de São Paulo (Dissertação de Mestrado em Ciências Médicas). Universidade Estadual de Campinas, Campinas. [ Links ]
MacCallan, M. (2015). Arthur Ferguson MacCallan: trachoma pioneer in Egypt 1903-1923. British Journal Ophtalmologyh, 99(5), 577-579. Recuperado de: https://pubmed.ncbi.nlm.nih.gov/25813831/ [ Links ]
Mann, I. (1957). Probable origins of trachoma in Australasia. Bulletin de l’Organisation Mondiale de la Santé/Bulletin of the World Health Organization, 16, 1165-1187. Recuperado de: https://apps.who.int/iris/handle/10665/265705 [ Links ]
Marques, V. R. B. (1994). A medicalização da raça. Campinas, SP: Editora da Unicamp. [ Links ]
Martins, V. (2015). Cidade-laboratório: Campinas e a febre amarela na aurora republicana. História, Ciências, Saúde - Manguinhos, 22(2), 507-524. Recuperado de: https://www.scielo.br/j/hcsm/a/BFKL6SSbbDg4q7svpdNdHrn/abstract/?lang=pt [ Links ]
Milot, J. (2010). Histoire du trachome au Canada. Canadian Journal of Ophthalmology, 45, 280-285. Recuperado de: https://www.canadianjournalofophthalmology.ca/article/S0008-4182(10)80014-6/pdf [ Links ]
Notas e Informações. (1905, 17 de fevereiro). O Estado de S. Paulo, 1. [ Links ]
Organizacion Panamericana de la Salud. (1928). Tracoma. Boletin de la Oficina Panamericana, 7(7), 839. [ Links ]
Ottoni, D. (1898). Clinica ophtalmologica - conjunctivite granulosa. Brazil-Medico, 41, 362-365. [ Links ]
Ottoni, D. (1906). Do trachoma no Brazil. Revista Medica de S. Paulo, 11, 223-232. [ Links ]
Paiva, T. F., & Gondra, J. G. (2017). Em prol do ofício, da salvação pública e de uma comunidade produtiva: higiene e saúde na formação de professoras primárias. In L. M. Bertucci, A. Mota, & L. B. Schraiber (Orgs.), Saúde e educação, um encontro plural (p. 249-270). Rio de Janeiro, RJ: Editora da Fiocruz. [ Links ]
Paparcone, E. (1922). Il Tracoma e sue complicazioni. Milano, IT: Soceitá Editrice Libraria. [ Links ]
Revel, J. (2010). Micro-história, macro-história: o que as variações de escala ajudam a pensar em um mundo globalizado. Revista Brasileira de Educação, 15(45), 434-444. Recuperado de: http://educa.fcc.org.br/scielo.php?script=sci_arttext&pid=S1413-24782010000300003 [ Links ]
Ribas, E. (1907). Relatório referente ao anno de 1906, apresentado pelo Dr. Emílio Ribas, Diretor do Serviço Sanitário ao Snr. Secretário dos Negócios do Interior. Revista Médica de S. Paulo, 11, 213-235. [ Links ]
Ribeiro, M. A. R. (1993). História sem fim: um inventario da saúde pública, São Paulo, 1880-1930. São Paulo, SP: Editora Unesp. [ Links ]
Rocha, H. H. P. (2003). A higienização dos costumes. Campinas, SP: Mercado de Letras. [ Links ]
Rocha, H. H. P. (2022). “Instruir as crianças nos princípios da higiene”: notas sobre viagens, livros e conexões entre Brasil e Estados Unidos. In A. L. Ecar, R. S. Batista, & A. Mota (Orgs.), Educação Sanitária (p. 43-58). São Paulo, SP: Hucitec. [ Links ]
Rocha, H. H. P., Viviani, L. M., & Lima, A. L. G. (2017). Formação de cidadãos higienizados para a construção do progresso nacional: produção e circulação de livros escolares de higiene na primeira metade do século XX. In L. M. Bertucci, A. Mota, & L. B. Schraiber (Orgs.), Saúde e educação, um encontro plural (p. 305-326). Rio de Janeiro, RJ: Editora da Fiocruz. [ Links ]
São Paulo. (1897). Congresso paulista. Camara dos deputados. Annaes da Camara dos Deputados: Sessão Ordinária de 1896, 2º anno da 3ª legislatura. São Paulo: Imprensa Official. [ Links ]
São Paulo. (1908). Relatório da Secretaria do Interior, annos de 1907 e 1908. São Paulo: Duprat & Comp. [ Links ]
Scarpi, M. J. (1991). História do tracoma no Brasil. Arquivos Brasileiros de Oftalmologia, 54(5), 202-205. Recuperado de: https://aboonline.org.br/details/4026/pt-BR/history-of-trachoma-in-brazil [ Links ]
Schwartsmann, L. C. B. (2020). O fenômeno imigratório e o controle do tracoma: repercussões da doença. História em Revista, 26(1), 146-162. Recuperado de: https://periodicos.ufpel.edu.br/index.php/HistRev/article/view/20618 [ Links ]
Serviço Sanitario. (1906). Serviço contra o trachoma - nomeações (volume manuscrito). São Paulo, SP. [ Links ]
Serviço Sanitario. (1907a, 10 de março). Commissão de Prophylaxia e Tratmaento do Tracoma. Diario Official, p. 803-805. [ Links ]
Serviço Sanitario. (1907b, 19 de Fevereiro). Commissão de Prophylaxia e Tratamento do Trachoma. Diario Official, p. 550. [ Links ]
Serviço Sanitario. (1907c, 28 de março). Commissão de Prophylaxia e Tratamento do Trachoma. Diario Official, p. 980. [ Links ]
Serviço Sanitario. (1907d, 7 de março). Commissão de Prophylaxia e Tratmaento do Tracoma. Diario Official, p. 770. [ Links ]
Serviço Sanitario do Estado de São Paulo. (1899). Peste. São Paulo, SP: Escola Typografica Salesiana. Recuperado de: https://revistapesquisa.fapesp.br/guerra-a-peste/ [ Links ]
Soares, M. G. (2022). Educação sanitária da criança pré-escolar (São Paulo, década de 1920). In A. L. Ecar, R. S. Batista, & A. Mota (Orgs.), Educação Sanitária (p. 104-123). São Paulo, SP: Hucitec. [ Links ]
Souza, R. F. (2016). A configuração das Escolas Isoladas no estado de São Paulo (1846-1904). Revista Brasileira de História da Educação, 16(2[41]), 341-337. Recuperado de: http://educa.fcc.org.br/scielo.php?script=sci_abstract&pid=S223800942016000200341&lng=pt&nrm=iso&tlng=pt [ Links ]
Souza, R. F. (1998). Templos de civilização. São Paulo, SP: Editora Unesp. [ Links ]
Stephanou, M. (2006). Discursos médicos, educação e ciência: escola e escolares sob exame. Trabalho, Educação e Saúde, 4(1), 33-64. Recuperado de: https://www.scielo.br/j/tes/a/wTKjXHQScqMxKNdtjH58Mnj/?lang=pt [ Links ]
Stephenson, S. (1900). The ophtalmic history of an English Scholl, 1856-1900. Archives of Ophtalmology, XXIX(4), 351-373. [ Links ]
Stern, I., & Marques, V. R. B. (2017). Morte aos ratos! In L. M. Bertucci, A. Mota, & L. B. Schraiber (Orgs.), Saúde e educação, um encontro plural (p. 107-129). Rio de Janeiro, RJ: Editora da Fiocruz. [ Links ]
Taylor, H. R. (2009). Tracoma. Doyne lecture: tracoma, is it history? Eye - Journal of The Royal College of Ophthalmologists, 23, 2007-2022. Disponível em: https://www.nature. com/articles/eye2008432 [ Links ]
Telarolli Junior, R. (1996). Poder e Saúde: as epidemias e a formação dos serviços de saúde em São Paulo. São Paulo, SP: Editora Unesp. [ Links ]
Trachoma. (1907, 14 de abril). A Federação, p. 3. [ Links ]
Trento, A. (1989). Do outro lado do Atlântico. São Paulo, SP: Nobel. [ Links ]
Vieira, S. (1905). Estudo clínico sobre o trachoma: sua prophylaxia no estado de São Paulo. Revista Médica de S. Paulo, 14, 297-307. [ Links ]
Funding: The RBHE has financial support from the Brazilian Society of History of Education (SBHE) and the Editorial Program (Call No. 12/2022) of the National Council for Scientific and Technological Development (CNPq).
1The main symptoms of trachoma are tearing, foreign body sensation, purulent discharge and photophobia. Approximately 25% of trachoma cases are asymptomatic. (Epidemiological Surveillance Center 'Prof Alexandre Vranjac.'"[CVE], n.d.).
2Currently, surgery continues to be recommended for severe cases of the disease (CVE, n.d). In the late 1930s, sulfonamides began to be used, and from the 1950s onwards, tetracyclines were included in the treatment of trachoma (Luna, 1993).
3In the second half of the 19th century, a trachoma epidemic cycle spread around the world. It began in continental Asia and soon reached Africa and Europe, spreading the disease to places where trachoma had not been detected before. With the intense European immigration movement of the time, the disease reached Australia and New Guinea and countries on the American continent. In addition to Brazil, cases of the disease were identified in Canada, the United States, Mexico, Colombia, Ecuador, Peru and Bolivia (Ottoni, 1898; Organizacion Panamerinaca de le Salud, 1928; Paparcone, 1922; Mann, 1957).
4At that time, Dr. David Ottoni identified people with trachoma in the states of Minas Gerais, Paraná, Santa Catarina and Rio Grande do Sul (Ottoni, 1906).
5The disease can be transmitted directly, indirectly through contaminated objects or through mechanical vectors such as flies (CVE, n.d.).
6Vaccines would increasingly become part of the prophylactic arsenal, beginning with the smallpox vaccine.
7In the following years, reports on the identification of different bacilli in the secretions of trachomatous eyes were published ( Benedetti, 1911), while studies argued that a highly contagious virus was the cause of the disease. Years later, the identification of the bacterium Chlamydia trachomatis as the etiological agent of trachoma ended the discussion regarding this microorganism: see Luna (1993).
8In the book, the involvement of the doctors participating in this process at the international level is evidenced, which was also reflected in the printed materials that were published. The discussion of the Brazil-United States connection in this regard has been addressed by the author, see Rocha (2022).
9In 1896, during discussions on the Sanitation Service reform in the São Paulo State Chamber of Deputies, members of the Hygiene Commission recalled that the state health department had been created due to the impact caused by the yellow fever epidemics in Santos and Campinas in the late 1880s (São Paulo, 1897). In Santos, the disease killed many immigrants, but it was the 1889 epidemic in Campinas that demonstrated that the disease ‘went up into the mountains’ and could invade the coffee plantation region (Bertucci, 2020).
10The decree determined that it was the duty of health inspectors to ‘advise’ the population on prophylactic means “ […] based on the strictest personal and domestic hygiene” (Decreto nº 394, 1896).
11According to the 1900 census, there were 2,282,279 inhabitants in the state of São Paulo, of which 529,187 were foreigners or of unknown nationality. The 1890 census had reported that 75,030 people born in other countries lived in São Paulo (Directoria…, 1920). In 1900, in the state capital alone there were around 75,000 Italians in a population of 239,820 residents (Trento, 1989).
12This inspection, which could lead to extradition, was conducted on immigrants whose passage was subsidized by the state government (Vieira, 1905). The health surveillance of ports was the responsibility of the federal government.
13No information was found on the number of publications distributed. For simple comparison, in 1906, according to Emilio Ribas, 100,000 pamphlets were distributed throughout the state, written in Portuguese and Italian, with “popular instructions” for the prevention of hookworm (Ribas, 1907).
14The territorial dimension of the health districts varied greatly. Of the 14 districts, the 4 largest were in areas with few population centers in the midwestern region and part of the northeast of the state, covering more or less half of the territory of São Paulo. The other 10 health districts were in the central-eastern strip of land and part of what was considered ‘western São Paulo’. See the map in Góis (2020).
15In Decree 1395, the name Trachoma Prophylaxis and Treatment Service was used. However, in the legislative text, the word Commission appears more than once to designate this service. Commission was also the most frequently used word in consulted sources and bibliographies.
16In 1904, there were 171 municipalities in São Paulo State, cf. Bassanezi; Scott; Bacellar, & Truzzi (2008).
17No posters or pamphlets produced by the Trachoma Prophylaxis and Treatment Commission from 1906 to 1908 were found.
18The doctors reaffirmed their determination for division by sex, both in the school group, with separate classes for girls and boys, and in isolated schools (Souza, 2016), which in most cases were either female or male. A point that should be noted is that providing treatment on alternate days, if it included dressings, was not in keeping with the recommendations of specialists in trachoma, such as David Ottoni, who advocated that dressings should be changed on a daily basis.
19According to Góis (2020), at this time, Emilio Ribas intended to strengthen the power of the Sanitation Service in the state and expand its activities at trachoma treatment centers, thereby multiplying the actions already taken under the command of the district health inspectors. This would be a way of becoming more involved in the rural areas of the municipalities. Ribas was on leave from his role as director of the Sanitation Service on the date on which the end of the Commission was decreed. It had been created in 1906, when the Secretary for the Interior was Gustavo de Oliveira Godoy.
Received: February 01, 2023; Accepted: June 15, 2023; Published: September 20, 2023; Published: September 22, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
